

Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 291-294 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dehghanpour barouj M, Ghaffarpasand A, Farzan A, Tabrizi R, Alam M. Treatment of an Old Zygomaticomaxillary Complex Fracture in a 9-Year-Old Child: A Case Report. J Res Dent Maxillofac Sci 2023; 8 (4) :291-294
URL: http://jrdms.dentaliau.ac.ir/article-1-504-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-504-en.html
Mehrdad Dehghanpour barouj1 

 , Arash Ghaffarpasand1 , Avishan Farzan2 , Reza Tabrizi1 , Mostafa Alam 3
, Arash Ghaffarpasand1 , Avishan Farzan2 , Reza Tabrizi1 , Mostafa Alam 3
, Arash Ghaffarpasand1 , Avishan Farzan2 , Reza Tabrizi1 , Mostafa Alam 3
1- Department of Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- School of Dentistry, Shahid Beheshti University of Medical Sciences, Teh-ran, Iran
3- Department of Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran , mostafaalam815@gmail.com
2- School of Dentistry, Shahid Beheshti University of Medical Sciences, Teh-ran, Iran
3- Department of Oral and Maxillofacial Surgery, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran , mostafaalam815@gmail.com
Full-Text [PDF 790 kb]
(166 Downloads)
| Abstract (HTML) (602 Views)
Introduction
Full-Text: (92 Views)
|
Abstract
Background and Aim: The zygomaticomaxillary complex (ZMC) refers to a main buttress in the skeleton of the midface. When open reduction and rigid fixation is selected as the treatment of choice for a ZMC fracture in pediatric patients, several factors such as immature dentition and growth potential of patient should be taken into account. This case report describes treatment of an old ZMC fracture in a 9-year-old child.
Case Presentation: A 9-year-old child was referred due to left ZMC fracture and orbital floor fracture with severe displacement. Open reduction and internal fixation of the ZMC fracture was performed using titanium plates. The orbital floor was reconstructed with a titanium mesh and the maxillary buttress fracture was reconstructed with an iliac crest bone graft. After surgery, the patient had an appropriate recovery and showed stable results. Conclusion: In a ZMC fracture with considerable displacement and an orbital floor fracture in children, 3-point fixation with titanium plate and reconstruction of the orbital floor are recommended. Key Words: Orbital Fractures; Zygomatic Fractures; Ilium |
Introduction
The zygomaticomaxillary complex (ZMC) is important for functional, structural, and esthetic aspects of the facial skeleton. A ZMC fracture is also known as a tripod, tetrapod, quadruped, trimalar, or a malar fracture [1, 2]. In general, management of ZMC fractures is challenging. The primary clinical features of ZMC fractures include ocular signs such as enophthalmos, diplopia, subconjunctival hemorrhage, and extraocular muscle entrapment, as well as cosmetic deformities due to malar eminence depression, and the resultant facial widening. In addition, malocclusion and infraorbital nerve-associated neurosensory disturbances may occur [3]. The surgical approach is often selected according to the results of physical and radiographic examinations. It is critical to sufficiently expose and mobilize the fragments of fracture to ensure correct anatomical reduction.
Secondary deformities may occur if the treatment is delayed or the reduction is insufficient [4, 5]. When rigid fixation is scheduled for children with ZMC fracture, presence of mixed dentition must be taken into account. Plate and screw fixation in the zygomaticomaxillary buttress can traumatize permanent maxillary tooth buds in this group of patients [6]. In addition, open reduction and internal fixation in children may lead to restriction of the midface growth and plate migration. Bioresorbable plates have been developed for use in pediatric facial fractures but when a displaced or unstable ZMC fracture is encountered, rigid plate and screw fixation could be considered as an option [7]. An association between rigid fixation and adverse outcomes after treatment of pediatric facial fractures has not been shown in human studies [8]. This case report describes treatment of an old ZMC fracture in a 9-year-old child.
Case Presentation
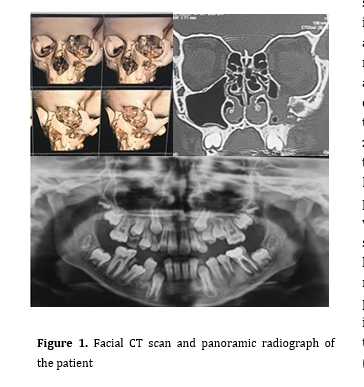
A 9-year-old patient was referred to the Department of Oral and Maxillofacial Surgery, Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. The patient reported that he had a car accident about one month earlier, which caused a left ZMC fracture and orbital floor fracture with severe displacement. A facial computed tomography (CT) scan was obtained and a panoramic radiograph was also taken (Figure 1).
Figure 1. Facial CT scan and panoramic radiograph of the patient
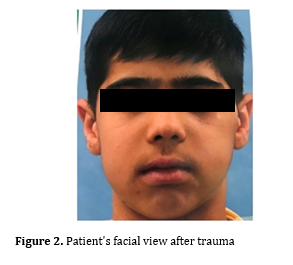
Figure 2. Patient's facial view after trauma
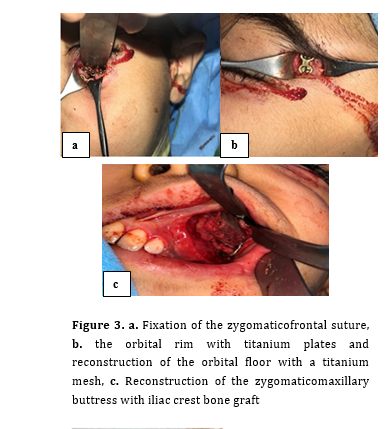
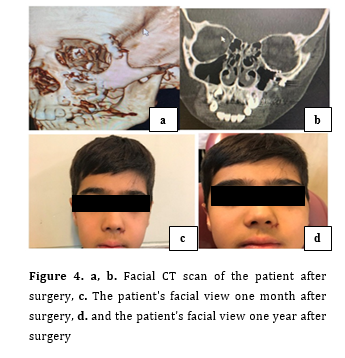
Clinical examination revealed moderate enophthalmos and hypoglobus in the left eye and left uniocular diplopia in the upper gaze, but visual acuity was found to be normal in the left side (Figure 2). Open reduction and internal fixation was planned upon admission of the patient. The patient received general anesthesia and following surgical site preparation, an intraoral vestibular incision was made. The zygomaticomaxillary buttress was accessed and the site of fracture was exposed. Then, a left lateral brow incision was performed to gain access to the zygomaticofrontal suture fracture, and finally a subtarsal incision was made to access the infraorbital rim and orbital floor fracture. After all fracture lines were detected and exposed, reduction of the ZMC complex was performed, and muscle entrapment of the orbital floor was corrected. Fixation of the fracture lines with titanium plates and screws was done in the zygomaticomaxillary buttress, zygomaticofrontal suture and the orbital rim sequentially. Moreover, a titanium mesh was formed and placed in the orbital floor defect, and was fixed with micro-screws (Figure 3 a, b). In the next step, due to the presence of large defects in the left zygomaticomaxillary buttress, a free monocortical iliac bone graft was harvested by preserving the cartilage portion of the right iliac crest. The iliac bone was then fixed to the maxillary buttress with mini-screws (Figure 3 c). A postoperative facial CT scan exhibited desirable reduction of the fracture sites. One month after the surgery, the enophthalmos, hypoglobus and diplopia, which were present preoperatively, were resolved. One year after surgery, the patient had a favorable recovery and showed a stable result (Figure 4 a-4 d).
Figure 3. a. Fixation of the zygomaticofrontal suture, b. the orbital rim with titanium plates and reconstruction of the orbital floor with a titanium mesh, c. Reconstruction of the zygomaticomaxillary buttress with iliac crest bone graft
Figure 4. a, b. Facial CT scan of the patient after surgery, c. The patient's facial view one month after surgery, d. and the patient's facial view one year after surgery
Discussion
Surgical treatment of ZMC fractures is performed when the displacement and/or rotation of the complex is significant. In fact, almost all the moderate to severely displaced ZMC fractures should be treated surgically. If reduction is not performed correctly, asymmetry of the midface may occur as a result of different three-dimensional orientations of malar projections [9]. A three-dimensional displacement usually occurs in ZMC fractures, meaning that the malar eminence can be displaced in mediolateral, superior-inferior, and anterior-posterior directions. Therefore, accurate reduction and fixation of the fractures are necessary [10]. Various incision methods can be performed in order to gain access to the zygomaticomaxillary fractures, using trans-oral and/or extraoral approaches. Subconjunctival incision, subciliary or subtarsal incision, lateral eyebrow incision, as well as coronal incisions are types of extraoral incisions. On the other hand, an intraoral gingivobuccal incision has the advantage of not leaving an external scar, while providing adequate exposure, reduction and fixation of the zygomaticomaxillary buttress. In this technique, achieving malar eminence symmetry without direct exposure of the lateral and inferior orbital rims could be challenging [11]. As opposed to the orbital growth, which is almost complete at the age of seven, ZMC fractures in children can pose a high potential for developing maxillary hypoplasia, most likely due to the involvement of the nasomaxillary growth complex [12,13]. As a consequence, a wider soft tissue exposure is necessary to ensure sufficient access to re-establish proper bony alignment. Determining the proper surgical approach for rigid fixation of the ZMC fractures in the pediatric population, however, remains controversial. For example, DeFazio et al. [14] recommend one- or two-point fixation for children with displaced or unstable ZMC fractures, while others [14,15] recommended one-point fixation with avoidance of the maxillary buttress to minimize damage to the permanent tooth buds. Sufficient data supporting the optimal number of fixation points are missing in the literature, and the frequency of damage to developing maxillary tooth buds is unclear.
Nonetheless, when a ZMC fracture is found to be notably displaced, a 3-point fixation is necessary for a stable result [16]. In the present case, we used a 3-point fixation due to severe displacement of the complex, and reconstruction of the orbital floor and the zygomaticomaxillary buttress was performed due to the large defects present.
Conclusion
In presence of severe displacement of ZMC and orbital floor fractures in children, a 3-point fixation with titanium plates and reconstruction of the orbital floor are recommended.
Secondary deformities may occur if the treatment is delayed or the reduction is insufficient [4, 5]. When rigid fixation is scheduled for children with ZMC fracture, presence of mixed dentition must be taken into account. Plate and screw fixation in the zygomaticomaxillary buttress can traumatize permanent maxillary tooth buds in this group of patients [6]. In addition, open reduction and internal fixation in children may lead to restriction of the midface growth and plate migration. Bioresorbable plates have been developed for use in pediatric facial fractures but when a displaced or unstable ZMC fracture is encountered, rigid plate and screw fixation could be considered as an option [7]. An association between rigid fixation and adverse outcomes after treatment of pediatric facial fractures has not been shown in human studies [8]. This case report describes treatment of an old ZMC fracture in a 9-year-old child.
Case Presentation
A 9-year-old patient was referred to the Department of Oral and Maxillofacial Surgery, Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. The patient reported that he had a car accident about one month earlier, which caused a left ZMC fracture and orbital floor fracture with severe displacement. A facial computed tomography (CT) scan was obtained and a panoramic radiograph was also taken (Figure 1).
Figure 1. Facial CT scan and panoramic radiograph of the patient
{kind=link}
Figure 2. Patient's facial view after trauma
{kind=link}
Clinical examination revealed moderate enophthalmos and hypoglobus in the left eye and left uniocular diplopia in the upper gaze, but visual acuity was found to be normal in the left side (Figure 2). Open reduction and internal fixation was planned upon admission of the patient. The patient received general anesthesia and following surgical site preparation, an intraoral vestibular incision was made. The zygomaticomaxillary buttress was accessed and the site of fracture was exposed. Then, a left lateral brow incision was performed to gain access to the zygomaticofrontal suture fracture, and finally a subtarsal incision was made to access the infraorbital rim and orbital floor fracture. After all fracture lines were detected and exposed, reduction of the ZMC complex was performed, and muscle entrapment of the orbital floor was corrected. Fixation of the fracture lines with titanium plates and screws was done in the zygomaticomaxillary buttress, zygomaticofrontal suture and the orbital rim sequentially. Moreover, a titanium mesh was formed and placed in the orbital floor defect, and was fixed with micro-screws (Figure 3 a, b). In the next step, due to the presence of large defects in the left zygomaticomaxillary buttress, a free monocortical iliac bone graft was harvested by preserving the cartilage portion of the right iliac crest. The iliac bone was then fixed to the maxillary buttress with mini-screws (Figure 3 c). A postoperative facial CT scan exhibited desirable reduction of the fracture sites. One month after the surgery, the enophthalmos, hypoglobus and diplopia, which were present preoperatively, were resolved. One year after surgery, the patient had a favorable recovery and showed a stable result (Figure 4 a-4 d).
Figure 3. a. Fixation of the zygomaticofrontal suture, b. the orbital rim with titanium plates and reconstruction of the orbital floor with a titanium mesh, c. Reconstruction of the zygomaticomaxillary buttress with iliac crest bone graft
{kind=link}
Figure 4. a, b. Facial CT scan of the patient after surgery, c. The patient's facial view one month after surgery, d. and the patient's facial view one year after surgery
{kind=link}
Discussion
Surgical treatment of ZMC fractures is performed when the displacement and/or rotation of the complex is significant. In fact, almost all the moderate to severely displaced ZMC fractures should be treated surgically. If reduction is not performed correctly, asymmetry of the midface may occur as a result of different three-dimensional orientations of malar projections [9]. A three-dimensional displacement usually occurs in ZMC fractures, meaning that the malar eminence can be displaced in mediolateral, superior-inferior, and anterior-posterior directions. Therefore, accurate reduction and fixation of the fractures are necessary [10]. Various incision methods can be performed in order to gain access to the zygomaticomaxillary fractures, using trans-oral and/or extraoral approaches. Subconjunctival incision, subciliary or subtarsal incision, lateral eyebrow incision, as well as coronal incisions are types of extraoral incisions. On the other hand, an intraoral gingivobuccal incision has the advantage of not leaving an external scar, while providing adequate exposure, reduction and fixation of the zygomaticomaxillary buttress. In this technique, achieving malar eminence symmetry without direct exposure of the lateral and inferior orbital rims could be challenging [11]. As opposed to the orbital growth, which is almost complete at the age of seven, ZMC fractures in children can pose a high potential for developing maxillary hypoplasia, most likely due to the involvement of the nasomaxillary growth complex [12,13]. As a consequence, a wider soft tissue exposure is necessary to ensure sufficient access to re-establish proper bony alignment. Determining the proper surgical approach for rigid fixation of the ZMC fractures in the pediatric population, however, remains controversial. For example, DeFazio et al. [14] recommend one- or two-point fixation for children with displaced or unstable ZMC fractures, while others [14,15] recommended one-point fixation with avoidance of the maxillary buttress to minimize damage to the permanent tooth buds. Sufficient data supporting the optimal number of fixation points are missing in the literature, and the frequency of damage to developing maxillary tooth buds is unclear.
Nonetheless, when a ZMC fracture is found to be notably displaced, a 3-point fixation is necessary for a stable result [16]. In the present case, we used a 3-point fixation due to severe displacement of the complex, and reconstruction of the orbital floor and the zygomaticomaxillary buttress was performed due to the large defects present.
Conclusion
In presence of severe displacement of ZMC and orbital floor fractures in children, a 3-point fixation with titanium plates and reconstruction of the orbital floor are recommended.
Type of Study: Case report |
Subject:
Oral & maxillofacial surgery
References
1. Ellstrom CL, Evans GRD. Evidence-based medicine: zygoma fractures. Plast Reconstr Surg. 2013 Dec;132(6): 1649-57. [DOI:10.1097/PRS.0b013e3182a80819] [PMID]
2. Meslemani D, Kellman RM. Zygomaticomaxillary complex fractures. Arch Facial Plast Surg. 2012 Jan-Feb;14(1):62-6. [DOI:10.1001/archfaci.2011.1415] [PMID]
3. Jung S, Yoon S, Nam SH. Proposal for a modified classification of isolated zygomatic arch fractures. Arch Craniofac Surg. 2022 Jun;23(3):111-8. [DOI:10.7181/acfs.2022.00045] [PMID] []
4. Pau CY, Barrera JE, Kwon J, Most SP. Three-dimensional analy-sis of zygomatic-maxillary complex fracture patterns. Cranio-maxillofac Trauma Reconstr. 2010 Sep;3(3):167-76. [DOI:10.1055/s-0030-1263082] [PMID] []
5. Uda H, Kamochi H, Sugawara Y, Sarukawa S, Sunaga A. The concept and method of closed reduction and internal fixation: a new approach for the treatment of simple zygoma fractures. Plast Reconstr Surg. 2013 Nov;132(5):1231-40. [DOI:10.1097/PRS.0b013e3182a48d8c] [PMID]
6. Juncar RI, Moca AE, Juncar M, Moca RT, Țenț PA. Clinical Pat-terns and Treatment of Pediatric Facial Fractures: A 10-Year Retrospective Romanian Study. Children (Basel). 2023 Apr 28;10(5):800. [DOI:10.3390/children10050800] [PMID] []
7. da Silva BCL, Souto-Souza D, de Souza GM, Magesty RA, de Cassia Ávila B, Galvão EL, Falci SGM. Comparison between re-sorbable plates vs. titanium plates for treatment of zygomatic fractures: a systematic review with meta-analysis. Oral Maxillofac Surg. 2021 Sep;25(3):289-301. [DOI:10.1007/s10006-020-00937-5] [PMID]
8. Liu FC, Le TT, Oleck NC, Halsey JN, Hoppe IC, Lee ES, Granick MS. Pediatric Pedestrian Facial Fracture Patterns and Manage-ment Following Motor Vehicle Collisions. J Craniofac Surg. 2020 Jan/Feb;31(1):265-8. [DOI:10.1097/SCS.0000000000006034] [PMID]
9. Huang W, Lynham A, Wullschleger M. Orbitozygomatic Frac-ture Repairs: Are Antibiotics Necessary? Craniomaxillofac Trauma Reconstr. 2015 Dec;8(4):271-6. [DOI:10.1055/s-0034-1399795] [PMID] []
10. Han SW, Kim JH, Kim SW, Kim SH, Kang DR, Kim J. Sensory change and recovery of infraorbital area after zygomaticomaxillary and orbital floor fractures. Arch Craniofac Surg. 2022 Dec;23(6):262-8. [DOI:10.7181/acfs.2022.01011] [PMID] []
11. El-Anwar MW, Elsheikh E, Hussein AM, Tantawy AA, Abdel-baki YM. Transconjunctival versus subciliary approach to the infraorbital margin for open reduction of zygomaticomaxillary complex fractures: a randomized feasibility study. Oral Maxillofac Surg. 2017 Jun;21(2):187-92. [DOI:10.1007/s10006-017-0617-2] [PMID]
12. Welkoborsky HJ, Plontke SK. Möglichkeiten des chirurgischen Zugangs zur Orbita . HNO. 2018 Nov;66(11): 812-26. [DOI:10.1007/s00106-018-0570-x] [PMID]
13. Tripathi N, Goyal M, Mishra B, Dhasmana S. Zygomatic com-plex fracture: A comparative evaluation of stability using titani-um and bio-resorbable plates as one point fixation. Natl J Maxil-lofac Surg. 2013 Jul;4(2):181-7. [DOI:10.4103/0975-5950.127648] [PMID] []
14. DeFazio MV, Fan KL, Avashia YJ, Danton GH, Thaller SR. Frac-tures of the pediatric zygoma: a review of the clinical trends, management strategies, and outcomes associated with zygomat-ic fractures in children. J Craniofac Surg. 2013 Nov;24(6):1891-7 [DOI:10.1097/SCS.0b013e3182a24659] [PMID]
15. Wong FK, Adams S, Coates TJ, Hudson DA. Pediatric Facial Fractures. J Craniofac Surg. 2016 Jan;27(1):128-30. [DOI:10.1097/SCS.0000000000002185] [PMID]
16. Mittal G, Agarwal A, Garg R, Sharma S, Rathi A, Kapse P. Effi-cacy of Microplates versus Miniplates in the Management of Maxillofacial Fractures. Ann Maxillofac Surg. 2020 Jan-Jun; 10(1):31-6. [DOI:10.4103/ams.ams_30_20] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
