

Volume 9, Issue 1 (3-2024)
J Res Dent Maxillofac Sci 2024, 9(1): 49-56 |
Back to browse issues page


Ethics code: IR.ZUMS.REC.1398.363
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Taheri S S, Farsadeghi M, Mostanadi M, Ansari A, Ghasemi N, Rafieyan S. Oral Health Literacy and Its Correlation with Socioeconomic Status in an Iranian Population. J Res Dent Maxillofac Sci 2024; 9 (1) :49-56
URL: http://jrdms.dentaliau.ac.ir/article-1-503-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-503-en.html
Seyyed Solmaz Taheri1 

 , Mahya Farsadeghi2 , Maedeh Mostanadi2 , Amin Ansari2 , Nikoo Ghasemi2 , Sona Rafieyan 3
, Mahya Farsadeghi2 , Maedeh Mostanadi2 , Amin Ansari2 , Nikoo Ghasemi2 , Sona Rafieyan 3
, Mahya Farsadeghi2 , Maedeh Mostanadi2 , Amin Ansari2 , Nikoo Ghasemi2 , Sona Rafieyan 3
1- Research Committee, Department of Biostatistics, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Dental School, Zanjan University of Medical Sciences, Zanjan, Iran.
3- Department of Oral and Maxillofacial Pathology, Dental School, Zanjan University of Medical Sciences, Zanjan, Iran , sona_rafieyan@yahoo.com
2- Dental School, Zanjan University of Medical Sciences, Zanjan, Iran.
3- Department of Oral and Maxillofacial Pathology, Dental School, Zanjan University of Medical Sciences, Zanjan, Iran , sona_rafieyan@yahoo.com
Full-Text [PDF 293 kb]
(126 Downloads)
| Abstract (HTML) (471 Views)
Table 1. Correlation of answers to the OHL questions with SES
Table 2. Results of the Chi-square and ANOVA for the correlation of OHL with SES, sex, and age
Results
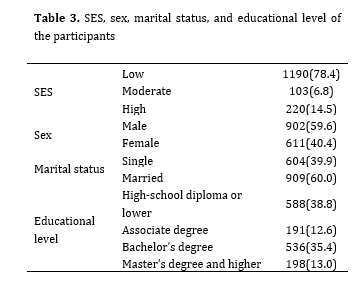
A total of 1,513 individuals participated in this study including 902 males (59.6%) and 611 females (40.4%) with a mean age of 33.3±9.93 years (range 18 to 61 years). Table 3 presents the characteristics of the participants. One participant did not completely answer the questions; nonetheless, questionnaires with only one or two unanswered questions were not omitted. The Cronbach’s alpha was 0.71, and the intra-class correlation coefficient was found to be 0.81, indicating good reliability and internal consistency. SES had a significant correlation with OHL (P<0.05, Tables 1 and 2). However, the correlation of OHL and age was not significant (P=0.9).
Table 3. SES, sex, marital status, and educational level of the participants
Discussion
According to the present results, the OHL of 33.3% of the participants was adequate (high), which was close to the value of 40% reported in a recent study [27]. However, Mohammadi et al. [28] considered 37.5% OHL as marginal level, and reported that 62% of their participants had moderate OHL.
In the present study, the OHL of those with lower SES was lower than others while Mohammadi et al. [28] and Naghibi Sistani et al. [29] concluded that OHL was independent of educational level and other determinants of SES.
Since income information is not reliable in Iran, SES is usually evaluated according to a combination of level of income, level of education, owning or renting a house, and surface area of the house.
Poor OHL can cause problems in receipt of preventive services, limit self-management skills, delay the diagnosis in diseased conditions, lead to poor hygiene outcomes, and increase the healthcare costs [30].
In the recent decade, OHL has gained increasing significance in dental literature [8]. The significance of OHL, similar to health literacy, in promotion of oral health and reduction of its variance has been well documented [31]. Also, it has been demonstrated that individuals with inadequate OHL are at high risk of oral and dental diseases and their consequences [32]. The World Health Organization has emphasized on OHL as a major parameter involved in oral health status [33]. Despite the increase in investigations on OHL, the main causes of inadequate OHL include lack of oral hygiene information, complex oral health instructions, and incompetent dentists. Assessment of OHL of patients can help improve their level of OHL in developing countries and reorganization of shortcomings in this respect [7].
Evidence shows that the mean level of OHL of females is higher than that of males, which is in agreement with the present results [27-29]. They also more commonly use oral health information available in the media. However, Sabbahi et al. [21] evaluated the OHL of adults in Canada and showed that gender had no significant effect on OHL. Similar results were reported by Atchison et al. [34], and Jones et al [35]. This difference may be explained by the fact that women often pay more attention to hygienic behaviors and take better care of their oral and dental health. The present results also showed low OHL in those with low SES. However, the correlation of OHL and age was not significant.
Considering the present results, it appears that knowledge enhancement of the public regarding oral health through the media can promote OHL of the general population. Studies on OHL have shown shortcomings in OHL of some specific groups such as those with lower educational level, the elderly, and the deprived individuals [35,36]. Information about the knowledge level of general population about important parameters in oral health is required for correct strategy planning for oral health knowledge enhancement in different communities. Considering the present results, educational interventions are required particularly for those with low SES to enhance their OHL.
Due to the large sample size, persuading the individuals to participate in the study was difficult. However, large sample size enabled generalizability of the results to the entire population of Zanjan city. The correlation of OHL and SES had not been evaluated in any previous study, and the present study appears to be the first to address this correlation in this geographical region. The results in this respect can aid in strategy planning for oral health knowledge enhancement in specific groups.
Conclusion
The OHL of the study population was moderate. Since there is no specific practical method for enhancement of OHL of the general population, educational OHL programs are recommended with particular attention to older individuals and those with lower SES.
Full-Text: (99 Views)
Abstract
Background and Aim: This study aimed to assess the oral health literacy (OHL) and its correlation with socioeconomic status (SES) in residents of Zanjan city, Iran by introducing a new questionnaire for this purpose.
Materials and Methods: This cross-sectional study was conducted on 1,513 individuals residing in Zanjan city, Iran, in 2019. The demographic information, OHL, and SES of the participants were evaluated by using relevant questionnaires. The reliability of the questionnaire designed for assessment of OHL was evaluated by calculation of the intra-class correlation coefficient and Cronbach’s alpha, while its validity was assessed by calculation of content validity index and content validity ratio. Data were analyzed by the Chi-square test and one-way ANOVA (alpha=0.05).
Results: Data of 1,513 individuals with a mean age of 33.3±9.93 years were analyzed, including 59.6% males and 40.4% females. The Cronbach’s alpha and intra-class correlation coefficient were found to be 0.71 and 0.81, respectively. OHL was inadequate in 29.1%, marginal in 37.4%, and adequate in 33.4% of the participants. The mean level of OHL of females was higher than males. Those with low SES had low OHL and this correlation was statistically significant (P<0.001).
Conclusion: The OHL of the study population was moderate. Since there is no specific practical method for enhancement of OHL of the general population, educational OHL programs are recommended with particular attention to older individuals and those with lower SES.
Key Words: Oral Health; Dental Health Surveys; Patient Health Questionnaire
Materials and Methods: This cross-sectional study was conducted on 1,513 individuals residing in Zanjan city, Iran, in 2019. The demographic information, OHL, and SES of the participants were evaluated by using relevant questionnaires. The reliability of the questionnaire designed for assessment of OHL was evaluated by calculation of the intra-class correlation coefficient and Cronbach’s alpha, while its validity was assessed by calculation of content validity index and content validity ratio. Data were analyzed by the Chi-square test and one-way ANOVA (alpha=0.05).
Results: Data of 1,513 individuals with a mean age of 33.3±9.93 years were analyzed, including 59.6% males and 40.4% females. The Cronbach’s alpha and intra-class correlation coefficient were found to be 0.71 and 0.81, respectively. OHL was inadequate in 29.1%, marginal in 37.4%, and adequate in 33.4% of the participants. The mean level of OHL of females was higher than males. Those with low SES had low OHL and this correlation was statistically significant (P<0.001).
Conclusion: The OHL of the study population was moderate. Since there is no specific practical method for enhancement of OHL of the general population, educational OHL programs are recommended with particular attention to older individuals and those with lower SES.
Key Words: Oral Health; Dental Health Surveys; Patient Health Questionnaire
Introduction
Literacy is a necessity for a healthy normal living in the 21st century [1]. People have to continuously enhance their knowledge to reach their goals, improve their level of literacy, use their potentials, and have a more solid presence in the society [2]. Literacy is no longer limited to reading and writing. It currently encompasses several skills such as reading and writing, counting, and verbal communication. The outcomes of poor health literacy are costly for the people and governments [3]. Several definitions are available for health literacy describing it as the necessary skills to achieve, perceive, and properly use health information to promote and preserve health [4-6].
Oral health literacy (OHL) is commonly defined as the required literacy for an individual to perceive and process the necessary information about oral and dental health and its related services [7]. OHL remains an important determinant of oral health in the literature [3,8-11]. Tehrani Banihashemi et al. [12] in their national survey of OHL of five provinces of Iran in 2007 reported a generally low level of OHL.
Several studies have proposed socioeconomic status (SES) as a determinant of OHL and clinical oral health status in different age groups [13-15]. Those with lower SES have shown poorer oral health status than those with higher SES [16-19].
The currently available questionnaires for assessment of OHL such as the Test of Functional Health Literacy in Dentistry [20], Oral Health Literacy Instrument [21], and the Comprehensive Measure of Oral Health Knowledge [22] have limited objectives. They measure the OHL according to the ability of individuals to perceive specific oral health terms or their ability in reading and interpretation of oral health data. Also, these tools are highly complex [20,21], and some of them are not applicable to all individuals. They are not self-reported questionnaires and some of them require a special place to play a sound for filling out some parts of the questionnaire [20-22]. Considering the significance of OHL, and having a comprehensive and understandable questionnaire that includes culturally qualified new criteria for verbal literacy skills, this study aimed to assess the OHL and its correlation with SES in residents of Zanjan city, Iran by introducing a new questionnaire for this purpose.
Materials and Methods
This cross-sectional study was conducted in Zanjan city, Iran from April to December 2019. The protocol of this study was ethically approved by Zanjan University of Medical Sciences (IR.ZUMS.REC.1398.363).
After designing the appropriate instrument, participants from Zanjan city were enrolled for a pilot study. The questionnaire was completed by 25 individuals from different SES [23] presenting to the dental clinic of Zanjan University of Medical Sciences to assess the validity, clarity, and readability of the items. To design a valid and reliable questionnaire to assess the OHL of adults, some of the previous OHL questionnaires [20-22,24] were also used. The initially designed questionnaire had 25 questions. The content validity of the questionnaire was then evaluated. For this purpose, 8 experts (4 oral medicine specialists, 2 methodologists, and 2 health instruction specialists) were asked to assess the validity, clarity, simplicity, and necessity of each question to calculate the content validity index and content validity ratio of the questionnaire.
The experts were asked to analyze each question by using a 3-point scale of necessary, beneficial but not necessary, and not necessary. After evaluation of all 25 questions, 2 questions were omitted, and the content validity index and content validity ratio were calculated to be 0.93 and 0.87, respectively. Although the results of the pilot study confirmed that the questionnaire was acceptably readable and perceivable, some questions were slightly modified. For example, some answer choices were added, or the writing style or order of questions were changed. The final version of the questionnaire had 23 questions. All questions and answer choices are presented in Tables 1 and 2. The SES questionnaire was used to assess the SES of the participants, which is reliable (with a Cronbach’s alpha of 0.83) and valid according to Eslami et al [25]. Some important demographic factors such as age, gender, marital status, and level of education of the participants were also assessed through the questionnaire. Thus, the final questionnaire had three sections of demographics, SES, and OHL. The OHL section of the questionnaire with 23 questions asked for the public knowledge about oral and dental health, and oral health maintenance in daily life.
The participants were selected by stratified random sampling to prevent bias. Two districts from each of the north, west, east, south and center of Zanjan city were randomly selected. In each district, five blocks were randomly chosen, and 15 households in each block were systematically selected. The participants who met the eligibility criteria (the ability to read and write, and age between 18 to 65 years) were randomly selected from the members of each household. The questionnaire was administered after giving instructions on how to fill out the different parts.
A total of 1548 questionnaires were filled out by eligible participants; out of which, 35 were excluded. Finally, data of 1,513 questionnaires were statistically analyzed. To assess the reliability of the questionnaires, 230 participants received a gift and were asked to fill out the questionnaire again after a one-week interval. The reliability of the questionnaire was then analyzed by test-retest reliability assessment using the intraclass correlation coefficient [26].
Also, the Cronbach’s alpha was calculated to analyze the internal consistency. According to the final total score of the questionnaire, the participants were categorized into three groups with inadequate (scores 0-12), marginal (scores 13-15), and adequate (scores 16-23] OHL using the S-TOFHLA categories (0-53: inadequate, 54-66: marginal, and 67-100: adequate).
Literacy is a necessity for a healthy normal living in the 21st century [1]. People have to continuously enhance their knowledge to reach their goals, improve their level of literacy, use their potentials, and have a more solid presence in the society [2]. Literacy is no longer limited to reading and writing. It currently encompasses several skills such as reading and writing, counting, and verbal communication. The outcomes of poor health literacy are costly for the people and governments [3]. Several definitions are available for health literacy describing it as the necessary skills to achieve, perceive, and properly use health information to promote and preserve health [4-6].
Oral health literacy (OHL) is commonly defined as the required literacy for an individual to perceive and process the necessary information about oral and dental health and its related services [7]. OHL remains an important determinant of oral health in the literature [3,8-11]. Tehrani Banihashemi et al. [12] in their national survey of OHL of five provinces of Iran in 2007 reported a generally low level of OHL.
Several studies have proposed socioeconomic status (SES) as a determinant of OHL and clinical oral health status in different age groups [13-15]. Those with lower SES have shown poorer oral health status than those with higher SES [16-19].
The currently available questionnaires for assessment of OHL such as the Test of Functional Health Literacy in Dentistry [20], Oral Health Literacy Instrument [21], and the Comprehensive Measure of Oral Health Knowledge [22] have limited objectives. They measure the OHL according to the ability of individuals to perceive specific oral health terms or their ability in reading and interpretation of oral health data. Also, these tools are highly complex [20,21], and some of them are not applicable to all individuals. They are not self-reported questionnaires and some of them require a special place to play a sound for filling out some parts of the questionnaire [20-22]. Considering the significance of OHL, and having a comprehensive and understandable questionnaire that includes culturally qualified new criteria for verbal literacy skills, this study aimed to assess the OHL and its correlation with SES in residents of Zanjan city, Iran by introducing a new questionnaire for this purpose.
Materials and Methods
This cross-sectional study was conducted in Zanjan city, Iran from April to December 2019. The protocol of this study was ethically approved by Zanjan University of Medical Sciences (IR.ZUMS.REC.1398.363).
After designing the appropriate instrument, participants from Zanjan city were enrolled for a pilot study. The questionnaire was completed by 25 individuals from different SES [23] presenting to the dental clinic of Zanjan University of Medical Sciences to assess the validity, clarity, and readability of the items. To design a valid and reliable questionnaire to assess the OHL of adults, some of the previous OHL questionnaires [20-22,24] were also used. The initially designed questionnaire had 25 questions. The content validity of the questionnaire was then evaluated. For this purpose, 8 experts (4 oral medicine specialists, 2 methodologists, and 2 health instruction specialists) were asked to assess the validity, clarity, simplicity, and necessity of each question to calculate the content validity index and content validity ratio of the questionnaire.
The experts were asked to analyze each question by using a 3-point scale of necessary, beneficial but not necessary, and not necessary. After evaluation of all 25 questions, 2 questions were omitted, and the content validity index and content validity ratio were calculated to be 0.93 and 0.87, respectively. Although the results of the pilot study confirmed that the questionnaire was acceptably readable and perceivable, some questions were slightly modified. For example, some answer choices were added, or the writing style or order of questions were changed. The final version of the questionnaire had 23 questions. All questions and answer choices are presented in Tables 1 and 2. The SES questionnaire was used to assess the SES of the participants, which is reliable (with a Cronbach’s alpha of 0.83) and valid according to Eslami et al [25]. Some important demographic factors such as age, gender, marital status, and level of education of the participants were also assessed through the questionnaire. Thus, the final questionnaire had three sections of demographics, SES, and OHL. The OHL section of the questionnaire with 23 questions asked for the public knowledge about oral and dental health, and oral health maintenance in daily life.
The participants were selected by stratified random sampling to prevent bias. Two districts from each of the north, west, east, south and center of Zanjan city were randomly selected. In each district, five blocks were randomly chosen, and 15 households in each block were systematically selected. The participants who met the eligibility criteria (the ability to read and write, and age between 18 to 65 years) were randomly selected from the members of each household. The questionnaire was administered after giving instructions on how to fill out the different parts.
A total of 1548 questionnaires were filled out by eligible participants; out of which, 35 were excluded. Finally, data of 1,513 questionnaires were statistically analyzed. To assess the reliability of the questionnaires, 230 participants received a gift and were asked to fill out the questionnaire again after a one-week interval. The reliability of the questionnaire was then analyzed by test-retest reliability assessment using the intraclass correlation coefficient [26].
Also, the Cronbach’s alpha was calculated to analyze the internal consistency. According to the final total score of the questionnaire, the participants were categorized into three groups with inadequate (scores 0-12), marginal (scores 13-15), and adequate (scores 16-23] OHL using the S-TOFHLA categories (0-53: inadequate, 54-66: marginal, and 67-100: adequate).
Table 1. Correlation of answers to the OHL questions with SES
Table 2. Results of the Chi-square and ANOVA for the correlation of OHL with SES, sex, and age
{kind=link}
Results
A total of 1,513 individuals participated in this study including 902 males (59.6%) and 611 females (40.4%) with a mean age of 33.3±9.93 years (range 18 to 61 years). Table 3 presents the characteristics of the participants. One participant did not completely answer the questions; nonetheless, questionnaires with only one or two unanswered questions were not omitted. The Cronbach’s alpha was 0.71, and the intra-class correlation coefficient was found to be 0.81, indicating good reliability and internal consistency. SES had a significant correlation with OHL (P<0.05, Tables 1 and 2). However, the correlation of OHL and age was not significant (P=0.9).
Table 3. SES, sex, marital status, and educational level of the participants
{kind=link}
Discussion
According to the present results, the OHL of 33.3% of the participants was adequate (high), which was close to the value of 40% reported in a recent study [27]. However, Mohammadi et al. [28] considered 37.5% OHL as marginal level, and reported that 62% of their participants had moderate OHL.
In the present study, the OHL of those with lower SES was lower than others while Mohammadi et al. [28] and Naghibi Sistani et al. [29] concluded that OHL was independent of educational level and other determinants of SES.
Since income information is not reliable in Iran, SES is usually evaluated according to a combination of level of income, level of education, owning or renting a house, and surface area of the house.
Poor OHL can cause problems in receipt of preventive services, limit self-management skills, delay the diagnosis in diseased conditions, lead to poor hygiene outcomes, and increase the healthcare costs [30].
In the recent decade, OHL has gained increasing significance in dental literature [8]. The significance of OHL, similar to health literacy, in promotion of oral health and reduction of its variance has been well documented [31]. Also, it has been demonstrated that individuals with inadequate OHL are at high risk of oral and dental diseases and their consequences [32]. The World Health Organization has emphasized on OHL as a major parameter involved in oral health status [33]. Despite the increase in investigations on OHL, the main causes of inadequate OHL include lack of oral hygiene information, complex oral health instructions, and incompetent dentists. Assessment of OHL of patients can help improve their level of OHL in developing countries and reorganization of shortcomings in this respect [7].
Evidence shows that the mean level of OHL of females is higher than that of males, which is in agreement with the present results [27-29]. They also more commonly use oral health information available in the media. However, Sabbahi et al. [21] evaluated the OHL of adults in Canada and showed that gender had no significant effect on OHL. Similar results were reported by Atchison et al. [34], and Jones et al [35]. This difference may be explained by the fact that women often pay more attention to hygienic behaviors and take better care of their oral and dental health. The present results also showed low OHL in those with low SES. However, the correlation of OHL and age was not significant.
Considering the present results, it appears that knowledge enhancement of the public regarding oral health through the media can promote OHL of the general population. Studies on OHL have shown shortcomings in OHL of some specific groups such as those with lower educational level, the elderly, and the deprived individuals [35,36]. Information about the knowledge level of general population about important parameters in oral health is required for correct strategy planning for oral health knowledge enhancement in different communities. Considering the present results, educational interventions are required particularly for those with low SES to enhance their OHL.
Due to the large sample size, persuading the individuals to participate in the study was difficult. However, large sample size enabled generalizability of the results to the entire population of Zanjan city. The correlation of OHL and SES had not been evaluated in any previous study, and the present study appears to be the first to address this correlation in this geographical region. The results in this respect can aid in strategy planning for oral health knowledge enhancement in specific groups.
Conclusion
The OHL of the study population was moderate. Since there is no specific practical method for enhancement of OHL of the general population, educational OHL programs are recommended with particular attention to older individuals and those with lower SES.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Kanj M, Mitic W, editors. Health literacy and health promotion: Definitions, concepts and examples in the Eastern Mediterranean region. 7th Global Conference on Health Promotion Promoting Health and Development: Closing the Implementation Gap; 2009.
2. UNESCO Education Sector. The Plurality of Literacy and I, ts Implications for Policies and Programs: Position Paper. Paris: United Nationals Educational, Scientific and Cultural Organization; 2004. p.13.
3. Horowitz AM, Kleinman DV. Oral health literacy: the new imperative to better oral health. Dental Clinics of North America. 2008;52(2):333-44. [DOI:10.1016/j.cden.2007.12.001] [PMID]
4. World Health Organization. Division of Health Promotion E, Communication. Health promotion glossary. Geneva: World Health Organization; 1998.
5. Ratzan S, Parker R. Health literacy. National library of medicine current bibliographies in medicine Bethesda: National Institutes of Health, US Department of Health and Human Services. 2000.
6. Healthy people 2010 final review. Hyattsville (MD): National Center for Health Statistics; 2012. http://www.cdc.gov/nchs/data/hpdata2010/hp2010_final_review.pdf.
7. National Institute of Dental and Craniofacial Research, National Institute of Health, U.S. Public Health Service, Department of Health and Human Services. The invisible barrier: literacy and its relationship with oral health. A report of a workgroup sponsored by the National Institute of Dental and Craniofacial Research, National Institute of Health, U.S. Public Health Service, Department of Health and Human Services. J Public Health Dent. 2005 Summer;65(3):174-82. [DOI:10.1111/j.1752-7325.2005.tb02808.x] [PMID]
8. Borrelli P, Henrik K, Enqvist O, Polymeri E, Ohlsson M, Elin T, et al. Prognostic value of automatically acquired biomarkers using artificial intelligence in 18F-Choline PET/CT in high-risk prostate cancer. Journal of Nuclear Medicine. 2019;60.
9. Horowitz A. The public's oral health: the gaps between what we know and what we practice. Advances in Dental Research. 1995;9(2):91-5. [DOI:10.1177/08959374950090022201] [PMID]
10. Parker EJ, Jamieson LM. Associations between indigenous Australian oral health literacy and self-reported oral health outcomes. BMC Oral Health. 2010;10(1):1-8. [DOI:10.1186/1472-6831-10-3] [PMID] []
11. Office of Disease Prevention and Health Promotion. Older Adults-Healthy People 2030. Available from: https://health. gov/healthypeople/objectives-and-data/browse-objectives/ older-adults
12. Tehrani Banihashemi SA, Haghdoost AA, Amirkhani MA, Alavian S-M, Asgharifard H, Baradaran H, et al. Health literacy and the influencing factors: a study in five provinces of Iran. Strides in Development of Medical Education. 2007;4(1):1-9.
13. Alwadi MAM, Vettore MV. Are school and home environmental characteristics associated with oral health‐related quality of life in Brazilian adolescents and young adults? Community Dentistry and Oral Epidemiology. 2017;45(4):356-64. [DOI:10.1111/cdoe.12298] [PMID]
14. Rebelo MA, de Castro PH, Rebelo Vieira JM, Robinson PG, Vettore MV. Low social position, periodontal disease, and poor oral health‐related quality of life in adults with systemic arterial hypertension. Journal of Periodontology. 2016;87(12):1379-87. [DOI:10.1902/jop.2016.160204] [PMID]
15. Vettore MV, Aqeeli A. The roles of contextual and individual social determinants of oral health-related quality of life in Brazilian adults. Quality of Life Research. 2016;25(4):1029-42. [DOI:10.1007/s11136-015-1118-0] [PMID]
16. Schwendicke F, Dörfer C, Schlattmann P, Page LF, Thomson W, Paris S. Socioeconomic inequality and caries: a systematic review and meta-analysis. Journal of Dental Research. 2015;94(1):10-8. [DOI:10.1177/0022034514557546] [PMID]
17. Tomazoni F, Vettore MV, Zanatta FB, Tuchtenhagen S, Moreira CHC, Ardenghi TM. The associations of socioeconomic status and social capital with gingival bleeding among schoolchildren. Journal of Public Health Dentistry. 2017;77(1):21-9. [DOI:10.1111/jphd.12166] [PMID]
18. Ariji Y, Sugita Y, Nagao T, Nakayama A, Fukuda M, Kise Y, et al. CT evaluation of extranodal extension of cervical lymph node metastases in patients with oral squamous cell carcinoma using deep learning classification. Oral Radiol. 2020;36(2):148-55. [DOI:10.1007/s11282-019-00391-4] [PMID]
19. Mohamed S, Vettore MV. Oral clinical status and oral health-related quality of life: is socioeconomic position a mediator or a moderator? International Dental Journal. 2019;69(2):119-29. [DOI:10.1111/idj.12420] [PMID] []
20. Gong DA, Lee JY, Rozier RG, Pahel BT, Richman JA, Vann Jr WF. Development and testing of the test of functional health literacy in dentistry (TOFHLiD). Journal of Public Health Dentistry. 2007;67(2):105-12. [DOI:10.1111/j.1752-7325.2007.00023.x] [PMID]
21. Sabbahi DA, Lawrence HP, Limeback H, Rootman I. Development and evaluation of an oral health literacy instrument for adults. Community Dentistry and Oral Epidemiology. 2009;37(5):451-62. [DOI:10.1111/j.1600-0528.2009.00490.x] [PMID]
22. Macek MD, Haynes D, Wells W, Bauer‐Leffler S, Cotten PA, Parker RM. Measuring conceptual health knowledge in the context of oral health literacy: preliminary results. Journal of Public Health Dentistry. 2010;70(3):197-204. [DOI:10.1111/j.1752-7325.2010.00165.x] [PMID] []
23. Moutselos K, Berdouses E, Oulis C, Maglogiannis I. Recognizing Occlusal Caries in Dental Intraoral Images Using Deep Learning. Annu Int Conf IEEE Eng Med Biol Soc. 2019 Jul;2019:1617-20. [DOI:10.1109/EMBC.2019.8856553] [PMID]
24. Naghibi Sistani MM, Montazeri A, Yazdani R, Murtomaa H. New oral health literacy instrument for public health: development and pilot testing. Journal of Investigative and Clinical Dentistry. 2014;5(4):313-21. [DOI:10.1111/jicd.12042] [PMID]
25. Eslami A, Mahmoudi A, Khabiri M, Najafiyan Razavi SM. The role of socioeconomic conditions in the citizens' motivation for participating in public sports. Applied Research in Sport Management, 2014; 2(3): 89-104.
26. Humphries SM, Centeno JP, Notary AM, Gerow J, Cicchetti G, Katial RK, et al. Volumetric assessment of paranasal sinus opacification on computed tomography can be automated using a convolutional neural network. Int Forum Allergy Rhinol. 2020;10(11):1218-25. [DOI:10.1002/alr.22588] [PMID]
27. Sistani M, Yazdani R, Virtanen J, Pakdaman A, Murtomaa H. Oral health literacy and information sources among adults in Tehran, Iran. Community Dent Health. 2013;30(3):178-82.
28. Mohammadi TM, Malekmohammadi M, Hajizamani HR, Mahani SA. Oral health literacy and its determinants among adults in Southeast Iran. European Journal of Dentistry. 2018;12(03):439-42. [DOI:10.4103/ejd.ejd_429_17] [PMID] []
29. Naghibi Sistani MM, Yazdani R, Virtanen J, Pakdaman A, Murtomaa H. Determinants of oral health: does oral health literacy matter? International Scholarly Research Notices. 2013;2013. [DOI:10.1155/2013/249591] [PMID] []
30. Schillinger D, Grumbach K, Piette J, Wang F, Osmond D, Daher C, et al. Poor health literacy may contribute to excess diabetes-related complications among disadvantaged groups. Journal of the American Medical Association. 2002;288(4):475-82. [DOI:10.1001/jama.288.4.475] [PMID]
31. Horowitz AM, Kleinman DV. Oral health literacy: a pathway to reducing oral health disparities in Maryland. Journal of Public Health Dentistry. 2012;72:S26-S30. [DOI:10.1111/j.1752-7325.2012.00316.x]
32. Batista MJ, Lawrence HP, Sousa MDLR. Oral health literacy and oral health outcomes in an adult population in Brazil. BMC Public Health. 2017 Jul 26;18(1):60. [DOI:10.1186/s12889-017-4443-0] [PMID] []
33. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International. 2000;15(3):259-67. [DOI:10.1093/heapro/15.3.259]
34. Atchison KA, Gironda MW, Messadi D, Der‐Martirosian C. Screening for oral health literacy in an urban dental clinic. Journal of Public Health Dentistry. 2010;70(4):269-75. [DOI:10.1111/j.1752-7325.2010.00181.x] [PMID] []
35. Jones M, Lee JY, Rozier RG. Oral health literacy among adult patients seeking dental care. J Am Dent Assoc. 2007 Sep;138(9):1199-208; quiz 1266-7. [DOI:10.14219/jada.archive.2007.0344] [PMID]
36. Lee JY, Divaris K, Baker AD, Rozier RG, Lee SYD, Vann Jr WF. Oral health literacy levels among a low‐income WIC population. Journal of Public Health Dentistry. 2011;71(2):152-60. [DOI:10.1111/j.1752-7325.2011.00244.x] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
