Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 274-279 |
Back to browse issues page


Ethics code: Not applicable
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mirzaee S, Shoorgashti R, Sadri D, Farhadi S. Comparison of EGFR Expression in Ameloblastoma and Odontogenic Keratocyst. J Res Dent Maxillofac Sci 2023; 8 (4) :274-279
URL: http://jrdms.dentaliau.ac.ir/article-1-502-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-502-en.html



1- Private Dentistry Practice, Tehran, Iran
2- Oral and Maxillofacial Pathology Department, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Oral and Maxillofacial Pathology Department, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,dr.sfarhadi@gmail.com
2- Oral and Maxillofacial Pathology Department, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Oral and Maxillofacial Pathology Department, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,
Full-Text [PDF 742 kb]
(836 Downloads)
| Abstract (HTML) (2490 Views)
Introduction
Ameloblastoma (AM) is a benign odontogenic tumor derived from the odontogenic epithelium with aggressive behavior and a high potential for recurrence (50-90% recurrence rate). This tumor is often asymptomatic and is identified accidentally in radiographic examination [1, 2]. Odontogenic keratocyst (OKC) is a developmental cyst with specific histopathological and clinical features. Unlike other odontogenic cysts, this cyst tends to recur after treatment with no clinical symptoms. OKC is derived from epithelial cells and expresses proliferating cell nuclear antigen, Ki67, P53, and protein patched homolog more than other odontogenic cysts, which makes it a unique cyst. Due to its tumor-like behavior, some researchers believe that OKC should be categorized as a benign tumor rather than a cyst [3-6].
Epidermal growth factor receptor (EGFR) is a growth factor receptor with a molecular weight of 170 kDa belonging to the family of receptor tyrosine kinase transmembrane. This receptor is naturally expressed by epithelial cells with a high proliferation rate, and plays an essential role in cell development and differentiation, tissue homeostasis, and signal transmission [7-9]. EGFR has excessive activity in the lung, breast, prostate, and cervical cancers [7, 10-13].
Considering the determining role of EGFR in head and neck cancers and high recurrence rate of AM and OKC after surgery and enucleation, it seems necessary to investigate more about the molecular background of these lesions to enhance their early detection and provide more treatment options. Thus, the present study was conducted to evaluate the expression of EGFR in AM and OKC.
Materials and Methods
The methodology of this study was approved by the Dental Research Committee and Dental Ethics Committee of Faculty of Dentistry, Islamic Azad Tehran Medical University (IR.IAU.DENTAL.REC.1397.053). This descriptive study was conducted on 20 AM and 26 OKC specimens. First, 5 µm slices were prepared for hematoxylin-eosin staining. Next, two oral and maxillofacial pathologists selected slides with adequate tissue and proper fixation without excessive bleeding and swelling. Specimens of recurrent lesions were excluded.
Immunohistochemical analysis of EGFR was performed using super-sensitive one-step polymer-HRP. The paraffin blocks were sectioned into 4 to 5 µm slices and placed in (3-Aminopropyl) triethoxysilane solution (Sigma-Aldrich, Germany). Then, sections were deparaffinized and rehydrated with xylene and graded concentrations of alcohol (Merck, Germany). TRIS EDTA buffer (pH=8) (Gibco, Germany) was applied on the sections at 96°C using a commercial microwave antigen retrieval system, and then antigen retrieval was performed 3 times for 8 minutes.
After washing with phosphate buffered saline (Bio-Idea, Iran), the sections were impregnated with a peroxidase block (3% hydrogen peroxide in water; Merck, Germany) for 15 minutes to prevent endogenous peroxidase activity. Then, before incubation with optimally pre-diluted antibodies against EGFR (Invitrogen, USA) at room temperature for one hour, a 20-minute power block (BioGenex, USA) was applied to inactivate any non-specific antigen. Next, the sections were washed with phosphate buffered saline and incubated again. Incubation was done for 30 minutes with polymer-HRP reagent (BioGenex, USA), and detection was done using DAB (3,3′-Diaminobenzidine) (Sigma-Aldrich, Germany). The sections were counter-stained with Harris hematoxylin (Sigma-Aldrich, Germany).
In this study, squamous cell carcinoma and normal oral mucosa were used as the positive control. Also, endothelial lining of blood vessels, non-reactive to EGFR, served as the internal negative control [14].
Expression of EGFR was evaluated based on the method described by Li et al, [15] at ×400 magnification in five random sections.
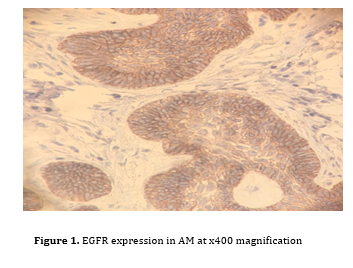
Evaluation was done quantitatively by measuring the count of membrane- and/or cytoplasm-stained epithelial cells in AM (ameloblastoma-like cells, stellate reticulum, and all epithelial cell layers) and OKC (basal layer, suprabasal and basal layers, and all epithelial cell layers). Next, each specimen's mean percentage of stained cells was scored and classified into four groups (less than 5%, 5-25%, 25-50%, and more than 50% stained cells). Based on this scoring system, the intensity of EGFR expression was determined. Scores < 5% indicated no marker expression, 5%- 25% indicated poor marker expression, 26%-50% indicated moderate expression, and scores >50% showed severe marker expression (Figures 1 and 2).
The data were analyzed using t-test and Mann-Whitney test to compare the mean EGFR expression and the percentage of stained cells in each score. Also, the Chi-square test was used to compare the location of EGFR expression. P<0.05 was considered statistically significant.
Figure 1. EGFR expression in AM at x400 magnification
Figure 2. EGFR expression in OKC at x100 magnification [5]
Results
This study was conducted on 46 specimens, including 26 OKC and 20 AM specimens.
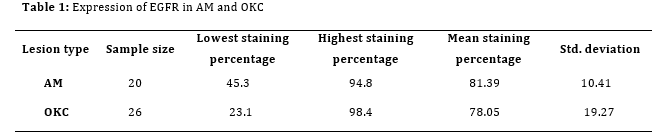
Table 1 shows the EGFR expression in AM and OKC. The lowest and the highest percentage of staining in AM were 45.3%±10.41% and 94.8%±10.41%, respectively; while these values for OKC were 23.1%±19.27% and 98.4%±19.27%, respectively. The mean percentage of stained cells in AM and OKC was 81.39±10.41% and 78.05±19.27%, respectively.
T-test showed no significant difference between AM and OKC regarding EGFR expression (P=0.528).
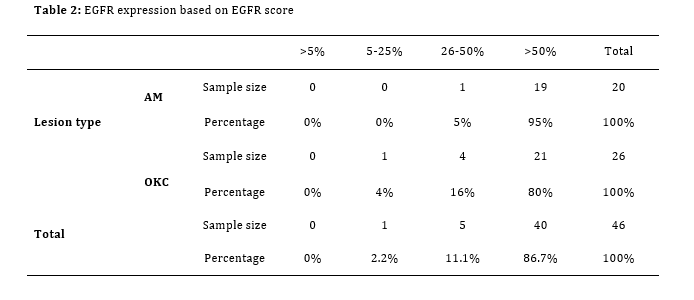
Table 2 shows EGFR expression in AM and OKC based on the scoring system. In the AM group, 95% of specimens scored > 50%, and only one (5%) scored 26-50%. In the OKC group, 80% of specimens scored > 50%, 16% scored 26-50%, and only one (4%) scored 5-25%.
Based on the Mann-Whitney test, no significant difference was found between AM and OKC in EGFR score (P=0.141).
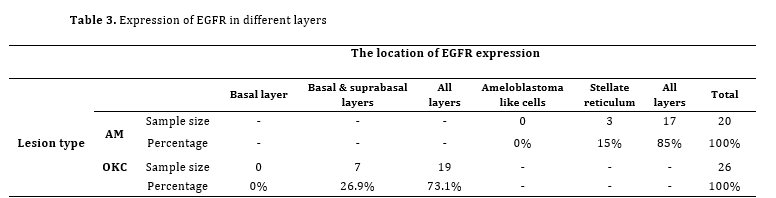
Table 3 shows the frequency and percentage of specimens based on the location of EGFR expression in AM and OKC. None of the specimens expressed EGFR in the basal layer in the two groups. Three specimens in AM (15%) and seven in OKC (26.9%) group expressed EGFR in the basal and suprabasal layers. Seventeen specimens in AM and 19 in OKC showed EGFR expression in all layers (85% and 73.1%, respectively). The Chi-square test showed no statistically significant difference in location of EGFR expression between the two groups (P=0.303).
Table 1: Expression of EGFR in AM and OKC
Table 2: EGFR expression based on EGFR score
Table 3. Expression of EGFR in different layers
Discussion
This study showed no significant difference between AM and OKC regarding the percentage and intensity of EGFR expression (P=0.141). The location of EGFR expression was not significantly different either (P=0.303).
Li et al. [15] analyzed 35 odontogenic cysts, 6 AMs, and 7 periapical granulomas and found that although the cytoplasm of epithelial cells stained for endothelial growth factor, most of the basal layer cells in theepithelium stained weakly [15]. In the present study, the location of EGFR expression was not significantly different between AM and OKC. However, EGFR expression increased by analyzing more layers of epithelium. The expression of EGFR in odontogenic and resting cysts can be affected by inflammation. In previous studies,odontogenic cysts like OKC and dentigerous cysts showed higher EGFR staining than inflammatory cysts, and they stained weakly in inflamed areas [4, 15, 16]. In a study by Razavi et al. [17], none of the OKC specimens were stained for EGFR. It might be because of inflammation or using a different staining method compared with the present study.
Razavi et al. [17] used biotin-streptavidin; while we used super-sensitive one step polymer-HRP.
Odontogenic tumors have unique properties and are only found in the oral cavity. These tumors originate from tissues contributing to odontogenesis and can be benign or malignant [18-21]. Tumor growth and metastasis depend on angiogenesis and its contributing factors. Vascular endothelial growth factors and epidermal growth factors are the most well-known factors that can play important roles in angiogenesis. These factors stimulate endothelial growth, differentiation, and migration, leading to tumor growth and metastasis [22-24].
In the present study, most of the specimens in AM and OKC groups showed more than 50% stained cells. Thus, they all scored by the same level, and no significant difference was found in this regard among them. However, the mean percentage of EGFR expression in AM was slightly more than that in OKC (3.34%), and the lowest percentage of AM staining was considerably more than that in OKC (45.3% and 23.1%, respectively). These findings can suggest more aggressive behavior of AM, which is a true neoplasm compared with OKC as an aggressive cyst.
The EGFR expression patterns may vary in epithelial cells [16, 25, 26], and its high expression in AM and OKC can be predictable based on their aggressive behavior. In a study conducted by de-Vicente et al. [16], all odontogenic epithelial tumors positively reacted to monoclonal antibodies of EGFR, but AM specimens expressed EGFR significantly more than others. Also, 100% of AM and 73% of OKC specimens were stained with EGFR.
AM and OKC behave aggressively with a high potential for recurrence. Today, clinical management of both tumors entirely depends on surgical approaches. Some mutations like a mutation in protein patched homolog 1 and loss of heterozygosity of tumor suppressor genes have been seen in OKC. Also, recent discoveries in AM regarding BRAF V600E provide new choices for targeted therapy. Nonetheless, the molecular backgrounds of AM and OKC have yet to be fully elucidated [7, 16, 27,28]. Studies like the present investigation enhance the current molecular knowledge about AM and OKC, leading to more practical non-aggressive treatment opportunities.
Conclusion
The present study showed no significant difference between AM and OKC regarding EGFR expression. The majority of specimens in both groups highly expressed EGFR, and the marginal disparity seen between OKC and AM can be a reason for the tumor-like behavior of OKC. However, further studies should be conducted to precisely clarify the molecular background of AM and OKC.
Full-Text: (949 Views)
|
Abstract
Background and Aim: Ameloblastoma (AM) and odontogenic keratocyst (OKC) are common lesions with a high recurrence rate. Epidermal growth factor receptor (EGFR) regulates cell proliferation and survival. Considering the controversial results of previous studies regarding the expression of EGFR in odontogenic cysts, this study aimed to compare the expression of EGFR in AM and OKC.
Materials and Methods: In this descriptive study, 49 specimens (20 AM and 26 OKC) were evaluated. Five micrometer sections were made for immunohistochemical staining. Immunohistochemical analysis was performed using super-sensitive one-step polymer-HRP. Expression of EGFR was first assessed quantitatively by measuring the count of membrane- and/or cytoplasm-stained epithelial cells in AM (ameloblastoma-like cells, stellate reticulum, and all epithelial cell layers) and OKC (basal layer, suprabasal and basal layers, and all epithelial cell layers). Next, each specimen's mean percentage of stained cells was scored and classified into four groups (less than 5%, 5-25%, 25-50%, and more than 50% stained cells). Data were analyzed by t-test and Mann-Whitney test to compare the mean EGFR expression and the percentage of stained cells. The Chi-square test was used to compare the location of EGFR expression. Results: The mean percentage of EGFR expression was 81.39±10.41% in AM and 78.05±19.27% in OKC. The results showed no significant difference between AM and OKC regarding EGFR expression, EGFR score (P=0.141), or EGFR expression in different layers (P=0.303). Conclusion: EGFR expression showed no significant difference between AM and OKC. Key Words: Ameloblastoma; ErbB Receptors; Odontogenic Cysts |
Introduction
Ameloblastoma (AM) is a benign odontogenic tumor derived from the odontogenic epithelium with aggressive behavior and a high potential for recurrence (50-90% recurrence rate). This tumor is often asymptomatic and is identified accidentally in radiographic examination [1, 2]. Odontogenic keratocyst (OKC) is a developmental cyst with specific histopathological and clinical features. Unlike other odontogenic cysts, this cyst tends to recur after treatment with no clinical symptoms. OKC is derived from epithelial cells and expresses proliferating cell nuclear antigen, Ki67, P53, and protein patched homolog more than other odontogenic cysts, which makes it a unique cyst. Due to its tumor-like behavior, some researchers believe that OKC should be categorized as a benign tumor rather than a cyst [3-6].
Epidermal growth factor receptor (EGFR) is a growth factor receptor with a molecular weight of 170 kDa belonging to the family of receptor tyrosine kinase transmembrane. This receptor is naturally expressed by epithelial cells with a high proliferation rate, and plays an essential role in cell development and differentiation, tissue homeostasis, and signal transmission [7-9]. EGFR has excessive activity in the lung, breast, prostate, and cervical cancers [7, 10-13].
Considering the determining role of EGFR in head and neck cancers and high recurrence rate of AM and OKC after surgery and enucleation, it seems necessary to investigate more about the molecular background of these lesions to enhance their early detection and provide more treatment options. Thus, the present study was conducted to evaluate the expression of EGFR in AM and OKC.
Materials and Methods
The methodology of this study was approved by the Dental Research Committee and Dental Ethics Committee of Faculty of Dentistry, Islamic Azad Tehran Medical University (IR.IAU.DENTAL.REC.1397.053). This descriptive study was conducted on 20 AM and 26 OKC specimens. First, 5 µm slices were prepared for hematoxylin-eosin staining. Next, two oral and maxillofacial pathologists selected slides with adequate tissue and proper fixation without excessive bleeding and swelling. Specimens of recurrent lesions were excluded.
Immunohistochemical analysis of EGFR was performed using super-sensitive one-step polymer-HRP. The paraffin blocks were sectioned into 4 to 5 µm slices and placed in (3-Aminopropyl) triethoxysilane solution (Sigma-Aldrich, Germany). Then, sections were deparaffinized and rehydrated with xylene and graded concentrations of alcohol (Merck, Germany). TRIS EDTA buffer (pH=8) (Gibco, Germany) was applied on the sections at 96°C using a commercial microwave antigen retrieval system, and then antigen retrieval was performed 3 times for 8 minutes.
After washing with phosphate buffered saline (Bio-Idea, Iran), the sections were impregnated with a peroxidase block (3% hydrogen peroxide in water; Merck, Germany) for 15 minutes to prevent endogenous peroxidase activity. Then, before incubation with optimally pre-diluted antibodies against EGFR (Invitrogen, USA) at room temperature for one hour, a 20-minute power block (BioGenex, USA) was applied to inactivate any non-specific antigen. Next, the sections were washed with phosphate buffered saline and incubated again. Incubation was done for 30 minutes with polymer-HRP reagent (BioGenex, USA), and detection was done using DAB (3,3′-Diaminobenzidine) (Sigma-Aldrich, Germany). The sections were counter-stained with Harris hematoxylin (Sigma-Aldrich, Germany).
In this study, squamous cell carcinoma and normal oral mucosa were used as the positive control. Also, endothelial lining of blood vessels, non-reactive to EGFR, served as the internal negative control [14].
Expression of EGFR was evaluated based on the method described by Li et al, [15] at ×400 magnification in five random sections.
Evaluation was done quantitatively by measuring the count of membrane- and/or cytoplasm-stained epithelial cells in AM (ameloblastoma-like cells, stellate reticulum, and all epithelial cell layers) and OKC (basal layer, suprabasal and basal layers, and all epithelial cell layers). Next, each specimen's mean percentage of stained cells was scored and classified into four groups (less than 5%, 5-25%, 25-50%, and more than 50% stained cells). Based on this scoring system, the intensity of EGFR expression was determined. Scores < 5% indicated no marker expression, 5%- 25% indicated poor marker expression, 26%-50% indicated moderate expression, and scores >50% showed severe marker expression (Figures 1 and 2).
The data were analyzed using t-test and Mann-Whitney test to compare the mean EGFR expression and the percentage of stained cells in each score. Also, the Chi-square test was used to compare the location of EGFR expression. P<0.05 was considered statistically significant.
Figure 1. EGFR expression in AM at x400 magnification
{kind=link}
Figure 2. EGFR expression in OKC at x100 magnification [5]
![Figure 2. EGFR expression in OKC at x100 magnification [5]](./files/site1/images/20234/fig2_shorghash.png){kind=link}
Results
This study was conducted on 46 specimens, including 26 OKC and 20 AM specimens.
Table 1 shows the EGFR expression in AM and OKC. The lowest and the highest percentage of staining in AM were 45.3%±10.41% and 94.8%±10.41%, respectively; while these values for OKC were 23.1%±19.27% and 98.4%±19.27%, respectively. The mean percentage of stained cells in AM and OKC was 81.39±10.41% and 78.05±19.27%, respectively.
T-test showed no significant difference between AM and OKC regarding EGFR expression (P=0.528).
Table 2 shows EGFR expression in AM and OKC based on the scoring system. In the AM group, 95% of specimens scored > 50%, and only one (5%) scored 26-50%. In the OKC group, 80% of specimens scored > 50%, 16% scored 26-50%, and only one (4%) scored 5-25%.
Based on the Mann-Whitney test, no significant difference was found between AM and OKC in EGFR score (P=0.141).
Table 3 shows the frequency and percentage of specimens based on the location of EGFR expression in AM and OKC. None of the specimens expressed EGFR in the basal layer in the two groups. Three specimens in AM (15%) and seven in OKC (26.9%) group expressed EGFR in the basal and suprabasal layers. Seventeen specimens in AM and 19 in OKC showed EGFR expression in all layers (85% and 73.1%, respectively). The Chi-square test showed no statistically significant difference in location of EGFR expression between the two groups (P=0.303).
Table 1: Expression of EGFR in AM and OKC
{kind=link}
Table 2: EGFR expression based on EGFR score
{kind=link}
Table 3. Expression of EGFR in different layers
{kind=link}
Discussion
This study showed no significant difference between AM and OKC regarding the percentage and intensity of EGFR expression (P=0.141). The location of EGFR expression was not significantly different either (P=0.303).
Li et al. [15] analyzed 35 odontogenic cysts, 6 AMs, and 7 periapical granulomas and found that although the cytoplasm of epithelial cells stained for endothelial growth factor, most of the basal layer cells in theepithelium stained weakly [15]. In the present study, the location of EGFR expression was not significantly different between AM and OKC. However, EGFR expression increased by analyzing more layers of epithelium. The expression of EGFR in odontogenic and resting cysts can be affected by inflammation. In previous studies,odontogenic cysts like OKC and dentigerous cysts showed higher EGFR staining than inflammatory cysts, and they stained weakly in inflamed areas [4, 15, 16]. In a study by Razavi et al. [17], none of the OKC specimens were stained for EGFR. It might be because of inflammation or using a different staining method compared with the present study.
Razavi et al. [17] used biotin-streptavidin; while we used super-sensitive one step polymer-HRP.
Odontogenic tumors have unique properties and are only found in the oral cavity. These tumors originate from tissues contributing to odontogenesis and can be benign or malignant [18-21]. Tumor growth and metastasis depend on angiogenesis and its contributing factors. Vascular endothelial growth factors and epidermal growth factors are the most well-known factors that can play important roles in angiogenesis. These factors stimulate endothelial growth, differentiation, and migration, leading to tumor growth and metastasis [22-24].
In the present study, most of the specimens in AM and OKC groups showed more than 50% stained cells. Thus, they all scored by the same level, and no significant difference was found in this regard among them. However, the mean percentage of EGFR expression in AM was slightly more than that in OKC (3.34%), and the lowest percentage of AM staining was considerably more than that in OKC (45.3% and 23.1%, respectively). These findings can suggest more aggressive behavior of AM, which is a true neoplasm compared with OKC as an aggressive cyst.
The EGFR expression patterns may vary in epithelial cells [16, 25, 26], and its high expression in AM and OKC can be predictable based on their aggressive behavior. In a study conducted by de-Vicente et al. [16], all odontogenic epithelial tumors positively reacted to monoclonal antibodies of EGFR, but AM specimens expressed EGFR significantly more than others. Also, 100% of AM and 73% of OKC specimens were stained with EGFR.
AM and OKC behave aggressively with a high potential for recurrence. Today, clinical management of both tumors entirely depends on surgical approaches. Some mutations like a mutation in protein patched homolog 1 and loss of heterozygosity of tumor suppressor genes have been seen in OKC. Also, recent discoveries in AM regarding BRAF V600E provide new choices for targeted therapy. Nonetheless, the molecular backgrounds of AM and OKC have yet to be fully elucidated [7, 16, 27,28]. Studies like the present investigation enhance the current molecular knowledge about AM and OKC, leading to more practical non-aggressive treatment opportunities.
Conclusion
The present study showed no significant difference between AM and OKC regarding EGFR expression. The majority of specimens in both groups highly expressed EGFR, and the marginal disparity seen between OKC and AM can be a reason for the tumor-like behavior of OKC. However, further studies should be conducted to precisely clarify the molecular background of AM and OKC.
Type of Study: Original article |
Subject:
Oral pathology
References
1. Henriques ÁC, Vasconcelos MG, Galvão HC, de Souza LB, de Almeida Freitas R. Comparative analysis of the immunohisto-chemical expression of collagen IV, MMP-9, and TIMP-2 in odon-togenic cysts and tumors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Oct;112(4):468-75. [DOI:10.1016/j.tripleo.2011.05.033] [PMID]
2. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillo-facial Pathology. 3th ed. Philadelphia: Saunders; 2008. 984 p.
3. Arkhipov A, Shan Y, Das R, Endres NF, Eastwood MP, Wem-mer DE, Kuriyan J, Shaw DE. Architecture and membrane interactions of the EGF receptor. Cell. 2013 Jan 31;152(3):557-69. [DOI:10.1016/j.cell.2012.12.030] [PMID] []
4. Briki S, Elleuch W, Karray F, Abdelmoula M, Tanoubi I. Cysts and tumors of the jaws treated by marsupialization: A descrip-tion of 4 clinical cases. J Clin Exp Dent. 2019;11 (6):e565-9. [DOI:10.4317/jced.55563] [PMID] []
5. Shoorgashti R, Sadri D, Farhadi S. Expression of Epidermal Growth Factor Receptor by Odontogenic Cysts: A comparative Study of Dentigerous Cyst and Odontogenic Kera-tocyst.J Res Dent Sci. 2020;17(2):127-36. [DOI:10.29252/jrds.17.2.127]
6. Al-Moraissi EA, Kaur A, Gomez RS, Ellis E 3rd. Effectiveness of different treatments for odontogenic keratocyst: a network meta-analysis. Int J Oral Maxillofac Surg. 2023 Jan;52(1):32-43. [DOI:10.1016/j.ijom.2022.09.004] [PMID]
7. Ceresa BP, Peterson JL. Cell and molecular biology of epidermal growth factor receptor. Int Rev Cell Mol Biol. 2014;313:145-78. [DOI:10.1016/B978-0-12-800177-6.00005-0] [PMID]
8. de Oliveira MG, Lauxen Ida S, Chaves AC, Rados PV, Sant'Ana Filho M. Odontogenic epithelium: immunolabeling of Ki-67, EGFR and survivin in pericoronal follicles, dentigerous cysts and keratocystic odontogenic tumors. Head Neck Pathol. 2011 Mar;5(1):1-7. [DOI:10.1007/s12105-010-0216-0] [PMID] []
9. Sabbah DA, Hajjo R, Sweidan K. Review on Epidermal Growth Factor Receptor (EGFR) Structure, Signaling Pathways, Interactions, and Recent Updates of EGFR Inhibitors. Curr Top Med Chem. 2020;20(10):815-34. [DOI:10.2174/1568026620666200303123102] [PMID]
10. Iradyan M, Iradyan N, Hulin P, Hambardzumyan A, Gyulkhandanyan A, Alves de Sousa R, Hessani A, Roussakis C, Bollot G, Bauvais C, Sakanyan V. Targeting Degradation of EGFR through the Allosteric Site Leads to Cancer Cell Detachment-Promoted Death. Cancers (Basel). 2019 Aug 1; 11(8):1094. [DOI:10.3390/cancers11081094] [PMID] []
11. He J, Huang Z, Han L, Gong Y, Xie C. Mechanisms and manage-ment of 3rd‑generation EGFR‑TKI resistance in advanced non‑small cell lung cancer (Review). Int J Oncol. 2021 Nov;59(5):90. [DOI:10.3892/ijo.2021.5270] [PMID] []
12. Harrison PT, Vyse S, Huang PH. Rare epidermal growth fac-tor receptor (EGFR) mutations in non-small cell lung cancer. Semin Cancer Biol. 2020 Apr;61:167-79. [DOI:10.1016/j.semcancer.2019.09.015] [PMID] []
13. Ayati A, Moghimi S, Salarinejad S, Safavi M, Pouramiri B, Foroumadi A. A review on progression of epidermal growth factor receptor (EGFR) inhibitors as an efficient approach in cancer targeted therapy. Bioorg Chem. 2020 Jun;99:103811. [DOI:10.1016/j.bioorg.2020.103811] [PMID]
14. Speight PM, Takata T. New tumour entities in the 4th edition of the World Health Organization Classification of Head and Neck tumours: odontogenic and maxillofacial bone tumours. Virchows Arch. 2018 Mar;472(3):331-9. [DOI:10.1007/s00428-017-2182-3] [PMID] []
15. Li TJ, Browne RM, Matthews JB. Expression of epidermal growth factor receptors by odontogenic jaw cysts. Virchows Arch A Pathol Anat Histopathol. 1993;423(2):137-44. [DOI:10.1007/BF01606588] [PMID]
16. de Vicente JC, Torre-Iturraspe A, Gutiérrez AM, Lequerica-Fernández P. Immunohistochemical comparative study of the odontogenic keratocysts and other odontogenic lesions. Med Oral Patol Oral Cir Bucal. 2010 Sep 1;15(5):e 709-15. [DOI:10.4317/medoral.15.e709] [PMID]
17. Razavi SM, Torabinia N, Mohajeri MR, Shahriyary S, Ghalego-lab S, Nouri S. Expression of Bcl-2 and epithelial growth factor receptor proteins in keratocystic odontogenic tumor in com-parison with dentigerous cyst and ameloblastoma. Dent Res J (Isfahan). 2015 Jul-Aug; 12(4): 342-7. [DOI:10.4103/1735-3327.161451] [PMID] []
18. Siwach P, Joy T, Tupkari J, Thakur A. Controversies in Odon-togenic Tumours: Review. Sultan Qaboos Univ Med J. 2017 Aug;17(3):e268-76. [DOI:10.18295/squmj.2017.17.03.003] [PMID] []
19. Mosqueda-Taylor A. New findings and controversies in odontogenic tumors. Med Oral Patol Oral Cir Bucal. 2008 Sep 1;13(9):E555-8.
20. El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ. WHO Classification of Head and Neck Tumours. 4th ed. Lyon: IARC Press; 2017..
21. Rajendra Santosh AB. Odontogenic Cysts. Dent Clin North Am. 2020 Jan;64(1):105-19. [DOI:10.1016/j.cden.2019.08.002] [PMID]
22. Maruthanila VL, Elancheran R, Kunnumakkara AB, Kabilan S, Kotoky J. Recent development of targeted approaches for the treatment of breast cancer. Breast Cancer. 2017 Mar;24(2):191-219. [DOI:10.1007/s12282-016-0732-1] [PMID]
23. Alaeddini M, Salah S, Dehghan F, Eshghyar N, Etemad-Moghadam S. Comparison of angiogenesis in keratocystic odontogenic tumours, dentigerous cysts and ame-loblastomas. Oral Dis. 2009 Sep;15(6):422-7. [DOI:10.1111/j.1601-0825.2009.01566.x] [PMID]
24. Kaufman NEM, Dhingra S, Jois SD, Vicente MDGH. Molecular Targeting of Epidermal Growth Factor Receptor (EGFR) and Vascular Endothelial Growth Factor Receptor (VEGFR). Molecules. 2021 Feb 18;26(4):1076. [DOI:10.3390/molecules26041076] [PMID] []
25. Schreier B, Dubourg V, Hübschmann S, Rabe S, Mildenberger S, Gekle M. Synergy of epidermal growth factor (EGFR) and angiotensin II (AT1R) receptor determines composition and temporal pattern of transcriptome variation. Cell Mol Life Sci. 2021 Dec 18;79(1):57. [DOI:10.1007/s00018-021-04065-5] [PMID] []
26. Wu L, Cheng Y, Geng D, Fan Z, Lin B, Zhu Q, Li J, Qin W, Yi W. O-GlcNAcylation regulates epidermal growth factor receptor intracellular trafficking and signaling. Proc Natl Acad Sci U S A. 2022 Mar 8;119(10):e2107453119. [DOI:10.1073/pnas.2107453119] [PMID] []
27. Arce K, Streff CS, Ettinger KS. Pediatric Odontogenic Cysts of the Jaws. Oral Maxillofac Surg Clin North Am. 2016 Feb;28(1):21-30. [DOI:10.1016/j.coms.2015.07.003] [PMID]
28. de Oliveira MG, Lauxen Ida S, Chaves AC, Rados PV, Sant'Ana Filho M. Odontogenic epithelium: immunolabeling of Ki-67, EGFR and survivin in pericoronal follicles, dentigerous cysts and keratocystic odontogenic tumors. Head Neck Pathol. 2011 Mar;5(1):1-7. [DOI:10.1007/s12105-010-0216-0] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |