Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 265-273 |
Back to browse issues page

Ethics code: (IR.MAZUMS.REC.1396.88).
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Namdar P, Molania T, Hoshyari N, Lotfizadeh A, Alimohammadi M, Khojastehfar M et al . Evaluation of Root and Canal Morphology of
Maxillary First and Second Molars by Cone Beam Computed Tomography in a Northern Iranian
Population. J Res Dent Maxillofac Sci 2023; 8 (4) :265-273
URL: http://jrdms.dentaliau.ac.ir/article-1-490-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-490-en.html
Parasto Namdar1 
 , Tahereh Molania2 , Narjes Hoshyari3 , Anahita Lotfizadeh4 , Mona Alimohammadi5 , Mana Khojastehfar4 , Azam Haddadi Kohsar *6
, Tahereh Molania2 , Narjes Hoshyari3 , Anahita Lotfizadeh4 , Mona Alimohammadi5 , Mana Khojastehfar4 , Azam Haddadi Kohsar *6 
, Tahereh Molania2 , Narjes Hoshyari3 , Anahita Lotfizadeh4 , Mona Alimohammadi5 , Mana Khojastehfar4 , Azam Haddadi Kohsar *6
1- Department of Orthodontics, Dental Research Center, Mazandaran University of Medical Sciences, Sari, Iran
2- Department of Oral Medicine, Dental Research Center, Mazandaran University of Medical Sciences, Sari, Iran
3- Department of Endodontics, Dental Research Center, Dental School, Mazandaran University of Medical Sciences, Sari, Iran
4- Private Dental Practice, Tehran, Iran
5- Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran
6- Department of Endodontics, Dental Research Center, Dental School, Mazandaran University of Medical Sciences, Sari, Iran ,haddadi_azam@yahoo.com
2- Department of Oral Medicine, Dental Research Center, Mazandaran University of Medical Sciences, Sari, Iran
3- Department of Endodontics, Dental Research Center, Dental School, Mazandaran University of Medical Sciences, Sari, Iran
4- Private Dental Practice, Tehran, Iran
5- Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran
6- Department of Endodontics, Dental Research Center, Dental School, Mazandaran University of Medical Sciences, Sari, Iran ,
Full-Text [PDF 877 kb]
(820 Downloads)
| Abstract (HTML) (3299 Views)
Full-Text: (1119 Views)
| Abstract Background and Aim: A thorough understanding of tooth and root canal morphology is required for successful root canal treatment. The current study aimed to assess the canal and root morphology of maxillary first molars (MFMs) and maxillary second molars (MSMs) using cone-beam computed tomography (CBCT). Materials and Methods: In this cross-sectional study, CBCT scans of 400 patients were used. The number of roots and canals, as well as the morphology of the root canal system of MFMs and MSMs were assessed according to the Vertucci’s classification, separately sorted by gender and by using OnDemand3D dental software. To compare the variables, the Chi-square test was used with a significance level of 0.05. Results: All the MFMs and MSMs had three roots. The most common morphologies according to the Vertucci’s classification in mesiobuccal (MB) roots of MFMs were type II (43.1%), followed by types I (28.7%), and IV (19.8%); while, types I (63.5%) and II (18.7%) were more commonly found in the MB roots of MSMs. All distobuccal (DB) and palatal roots were type I. The frequency of the second mesiobuccal (MB2) canal in MFMs and MSMs was 71.3% and 36.6%, respectively. Gender had no significant correlation with presence of MB2 canal (P>0.05). Conclusion: Three roots with four canals were the most common in MFMs while three roots with three canals were the most frequent in MSMs. Variations in MB roots were greater than in other roots. The frequency of MB2 in MFMs was greater than that in MSMs. |
Key Words: Cone-Beam Computed Tomography; Dental Pulp Cavity; Maxilla; Molar; Tooth Root
Introduction
Thorough chemo-mechanical cleaning and three-dimensional (3D) obturation of the root canal system are required for a favorable root canal procedure. Inability to locate, prepare, or obturate one or more root canals is a common cause of endodontic treatment failure (1).
Previous studies have reported diversities in the number and morphology of roots and canals in different ethnicities (2). As a result, the clinicians should be well aware of the typical configurations as well as potential anatomical variations of the root canal system to minimize the risk of treatment failure due to missing a canal (3). Maxillary permanent molars are often affected by caries at a young age and may require root canal therapy (4).
Studies have shown that the second mesiobuccal canals (MB2) of maxillary molars are generally present in 59.3% of the teeth. Due to the high prevalence of MB2 canals and the challenge of finding calcified and narrow canals, MB2 canals may be missed during treatment, and cause treatment failure (5, 6). Sadeghi and Sadr Lahijani (7) evaluated the prevalence of different root canal types of maxillary molars in an Iranian population and found variations in the number and configuration of root canals, particularly in mesiobuccal (MB)roots. Therefore, adequate knowledge about the root canal anatomy before root canal therapy is a critical factor for a favorable outcome and long-term prognosis (8).
A variety of methods such as sectioning (7), canal staining and tooth clearing technique (9), radiography (10), enhanced-medium contrast radiography (11), cone-beam computed-tomography (CBCT) (12), and micro computed-tomography (13) have been used to investigate the root and canal morphologies. The canal staining and clearing techniques and their modifications are believed to be the gold standard for assessment of the anatomy of the root canal system. However, these procedures are performed on extracted teeth (14). Since periapical radiographs are two-dimensional, and there is a possibility of superimposition of structures and root canals in the buccolingual plane, some root canals may not be detected on periapical radiographs (15, 16).
CBCT has been used in endodontics since 1990. It is non-invasive and enables more precise examination of the canals (17).
Moreover, it provides useful anatomical information about the teeth in the coronal, axial, and sagittal sections (18).
There is a gap of information about the morphology of the roots and canals using CBCT in the Iranian population. Considering the complexity of the morphology of maxillary first molars (MFMs) and maxillary second molars (MSMs), the current study aimed to evaluate the morphology of the roots and canals of MFMs and MSMs in a northern Iranian population.
Materials and Methods
The ethics committee of Mazandaran University of Medical Sciences in Sari, Iran, approved the research protocol of this study (IR.MAZUMS.REC.1396.88).
The current cross-sectional study collected 400 archived CBCT scans (173 females and 227 males) of MFMs and MSMs of patients referred to private oral and maxillofacial radiology centers in Sari. Maxillary molars with immature roots, apical periodontitis, root canal filling, posts, and crowns were excluded from the study. Finally, CBCT scans of 348 MFMs and 402 MSMs were analyzed.
All CBCT scans had been obtained by CranexTM 3D scanner (Soredex, Helsinki, Finland) with a 6×8 cm field of view, 75 µm resolution voxel size, and 90kV. Two endodontists observed the scans using OnDemand 3D Dental Viewer software (Cybermed Inc, Irvine, CA). They evaluated all teeth in axial, sagittal, and coronal planes and assessed the frequency of roots and canals, their morphology, and configuration according to the Vertucci's classification, along with the fused and C-shaped canals (19, 20).
The collected data were analyzed by SPSS version 23. Descriptive statistics were reported for the prevalence and demographic features of the samples, and the Chi-square test was run to find differences between the variables at a significance level of 0.05.
Results
Canal configuration:
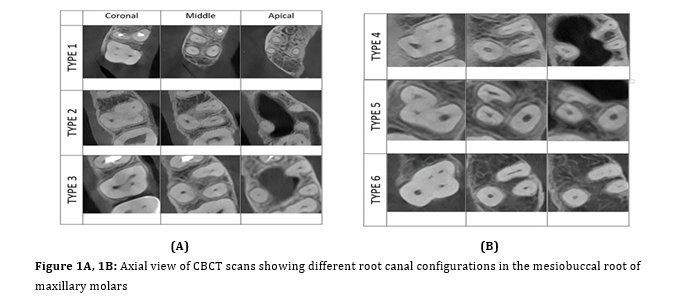
According to the Vertucci's classification, type II was the most common in the MB roots of MFMs, followed by type I and type IV in both males and females. On the other hand, the most prevalent types in the MB root of MSMs were types I, II, and IV, respectively in both sexes. All palatal and distobuccal (DB) roots of MFMs and MSMs demonstrated Vertucci's type I configuration (Table 1, Figures 1A, 1B, and 2).
The frequency of MB2 canal of MFMs was 67.4% and 76.1% in females and males, respectively; while these values were 31.3% and 43.7%, respectively in MSMs. Although the frequency of MB2 canals in MFMs and MSMs was greater in males than females, the difference was not statistically significant (P>0.05). Altogether, MB2 canals were discovered in 71.3% of MFMs and 37.1% of MSMs.
Number of root canals:
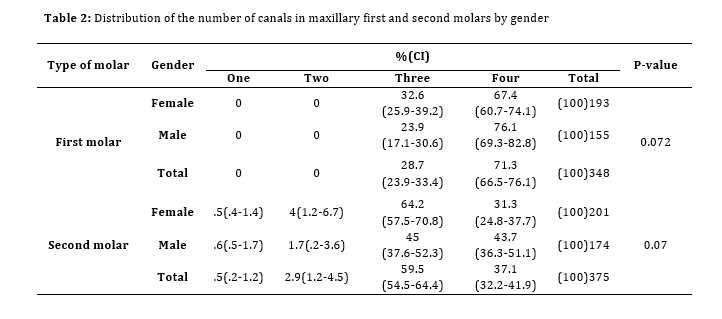
Table 2 illustrates the frequency of canals in maxillary molars. Accordingly, 28.7% of MFMs had three, and 71.3% had four root canals. MSMs with three root canals had the highest prevalence in both males and females. Of 375 MSMs, 2 (0.5%), 11 (2.9%), 223 (59.5%), and 139 (37.1%) had one, two, three, and four canals, respectively. The difference was not significant between males and females(P>0.05).
Number of roots:
Each MFM had three distinct roots;
whereas, most MSMs (95.7%) had three roots (only 2.7% had two roots). Table 3 shows MSMs with one (0.8%) and four (0.8%) roots.
Since teeth with fused roots and C-shaped canals cannot be classified according to the Vertucci's classification, they were reported separately. C-shaped canals were observed in 5 MSMs (1.2%), and 5.4% had fused root (14 females and 8 males) (Figure 3).
Table 1: Configuration of the root canal system in the mesiobuccal root of maxillary first and second molars by gender
Figure 1A, 1B: Axial view of CBCT scans showing different root canal configurations in the mesiobuccal root of maxillary molars
Figure 2: Cross-sectional view of CBCT scans showing different root canal configurations in the mesiobuccal root of maxillary molars
Table 2: Distribution of the number of canals in maxillary first and second molars by gender
Table 3: Number of roots in maxillary second molars by gender
Figure 3: C-shaped and fused root canal configurations in maxillary second molars (A: Type V, B: Type II, C:Type III, D: Type VII)
Discussion
This study assessed the morphology, number, and configuration of maxillary molar roots and canals according to the Vertucci’s classification using CBCT. The findings of the current study demonstrated that type II and type I were the most frequent in MB roots of MFMs and MSMs, respectively. Type I configuration was discovered in all palatal roots of the samples. Four root canals were found in 71.3% of MFMs. All MFMs had three roots, as did 95.7% of MSMs.
Permanent MFMs and MSMs have the highest complexities and variations in the root canal system; therefore, they have the highest failure rate in endodontic treatment and are a challenge for dental clinicians (21). In the present study, the morphology and anatomy of MFMs and MSMs were evaluated using CBCT.
The current investigation found that type II (43.1%), followed by type I (28.7%) and type IV (19.8%), were the most frequent canal types. Similarly, Al Mheiri et al. (5) evaluated an Emirati population and Alrahabi et al. studied a Saudi population and claimed that most of the MB roots were type II, type I, and type IV, respectively(22). Contrastingly, a previous study on an Iranian population discovered that the commonest types were type II (53.1%) and type I (29.8%) in the MB root of MFMs (6). In contrast to the present study, Kim et al. (23) evaluated a Korean population and Ratanajirasut et al. (24) assessed a Thai population using CBCT, and demonstrated type I to be the most frequent. One reason for such variations in the results can be the racial differences.
In the MB root of MSMs in the current study, the commonest types were type I (63.5%) and type II (18.7%). Correspondingly, Kim et al. (23) revealed that out of 644 MSMs, 63.48% were type I and 16.6% were type II. According to Ratanajirasut et al. (24), the most frequent canal morphology in the MB roots of MSMs was type I (70.6%) followed by type II (14.6%). On the other hand, Xia et al. (25) in their study on a Chinese population used CBCT and demonstrated that the MB root of 74.25% of MSMs was type I, followed by type IV (16.25%.). In contrast to the present results, Naseri et al. (26) found that in MB roots of MFMs of an Iranian population, type IV had the highest and type III had the lowest frequency.
This study revealed that in all palatal and DB roots of MFMs and MSMs, one single canal (type I) was observed. In a study by Al Mheiri et al.(5), only 1.2% and 2% of the examined teeth showed type II in the palatal and DB roots, respectively. Single canal configuration (type I) was more prevalent in these roots. Moreover, Alrahabi et al. (22) revealed that all DB and palatal roots of the examined teeth in their study were type I. Likewise, Ratanajirasut et al. (24) reported type I canal configuration as the most frequent in MFMs and MSM DB and palatal roots. In the study by Naseri et al. (26), type I and V palatal root canals had the highest and lowest frequency, respectively, in MFMs. In the DB roots, type I with the highest prevalence and type V with the lowest prevalence were the only observed canal types. Consistent with the present study, type I root canals were the most frequent in palatal and DB roots.
Ghoncheh et al. (27) used CBCT and suggested that in MFMs, type I had the highest and type V had the lowest frequency in MB and DB roots. All palatal roots were type I. In MSMs, type I and type II had the highest and lowest prevalence in MB roots, respectively. Additionally, all DB and palatal roots were type I. However, in the current study, the most frequent root canal type morphology in the MB root of MFMs was type II. The prevalence of type I root canal in the MB root of MSMs and the frequency of type I root canal in palatal and distal canals were consistent with the results of the present study.
In line with the present findings, Naseri et al. (26) did not discover any significant correlation between root canal configuration and age or gender. Similar to Pawar et al. (28) and Al Mheiri et al. (5), this study demonstrated that sex had no significant effect on canal configuration in maxillary molars' MB root.
Regarding the number of roots, all (100%) MFMs in the current study had three separate roots. The findings of the current study were consistent with those of Goncheh et al. (27) who reported 3 separate root morphology as the most prevalent morphology in MFMs and MSMs; however, the frequency of 3 separate roots in MFMs and MSMs in the current study was higher. Correspondingly, Zhang et al. (29) and Ghobashy et al. (20) discovered that all MFMs examined by CBCT had three roots. Moreover, after examining 974 MFMs, Pawar et al. (28) found that 99.1% had three and 0.8% had two roots. Another study by Kalender et al. (30) showed that 97.8% of the teeth had three, only 0.5% had two, and 1.6% had four roots. Finally, Ratanajirasut et al. (24) showed that out of 476 MFMs, 99.8% had three, and only one case (0.2%) had four roots.
In the present study, MSMs showed more variations in the morphology and number of roots compared to MFMs. Most MSMs had three (95.7%), while only 2.7% had two roots. However, MSMs with one (0.8%) and four (0.8%) roots were also found.
Zhang et al. (29) showed that out of 210 MSMs, 10% had one root, 9% had two, and 82% had three separate roots. However, the present study revealed no MSM with four roots. In a study by Kalender et al. (30), 3.1% of the teeth had one, 5.9% had two, 89.4% had three, and 1.3% had four roots.
Introduction
Thorough chemo-mechanical cleaning and three-dimensional (3D) obturation of the root canal system are required for a favorable root canal procedure. Inability to locate, prepare, or obturate one or more root canals is a common cause of endodontic treatment failure (1).
Previous studies have reported diversities in the number and morphology of roots and canals in different ethnicities (2). As a result, the clinicians should be well aware of the typical configurations as well as potential anatomical variations of the root canal system to minimize the risk of treatment failure due to missing a canal (3). Maxillary permanent molars are often affected by caries at a young age and may require root canal therapy (4).
Studies have shown that the second mesiobuccal canals (MB2) of maxillary molars are generally present in 59.3% of the teeth. Due to the high prevalence of MB2 canals and the challenge of finding calcified and narrow canals, MB2 canals may be missed during treatment, and cause treatment failure (5, 6). Sadeghi and Sadr Lahijani (7) evaluated the prevalence of different root canal types of maxillary molars in an Iranian population and found variations in the number and configuration of root canals, particularly in mesiobuccal (MB)roots. Therefore, adequate knowledge about the root canal anatomy before root canal therapy is a critical factor for a favorable outcome and long-term prognosis (8).
A variety of methods such as sectioning (7), canal staining and tooth clearing technique (9), radiography (10), enhanced-medium contrast radiography (11), cone-beam computed-tomography (CBCT) (12), and micro computed-tomography (13) have been used to investigate the root and canal morphologies. The canal staining and clearing techniques and their modifications are believed to be the gold standard for assessment of the anatomy of the root canal system. However, these procedures are performed on extracted teeth (14). Since periapical radiographs are two-dimensional, and there is a possibility of superimposition of structures and root canals in the buccolingual plane, some root canals may not be detected on periapical radiographs (15, 16).
CBCT has been used in endodontics since 1990. It is non-invasive and enables more precise examination of the canals (17).
Moreover, it provides useful anatomical information about the teeth in the coronal, axial, and sagittal sections (18).
There is a gap of information about the morphology of the roots and canals using CBCT in the Iranian population. Considering the complexity of the morphology of maxillary first molars (MFMs) and maxillary second molars (MSMs), the current study aimed to evaluate the morphology of the roots and canals of MFMs and MSMs in a northern Iranian population.
Materials and Methods
The ethics committee of Mazandaran University of Medical Sciences in Sari, Iran, approved the research protocol of this study (IR.MAZUMS.REC.1396.88).
The current cross-sectional study collected 400 archived CBCT scans (173 females and 227 males) of MFMs and MSMs of patients referred to private oral and maxillofacial radiology centers in Sari. Maxillary molars with immature roots, apical periodontitis, root canal filling, posts, and crowns were excluded from the study. Finally, CBCT scans of 348 MFMs and 402 MSMs were analyzed.
All CBCT scans had been obtained by CranexTM 3D scanner (Soredex, Helsinki, Finland) with a 6×8 cm field of view, 75 µm resolution voxel size, and 90kV. Two endodontists observed the scans using OnDemand 3D Dental Viewer software (Cybermed Inc, Irvine, CA). They evaluated all teeth in axial, sagittal, and coronal planes and assessed the frequency of roots and canals, their morphology, and configuration according to the Vertucci's classification, along with the fused and C-shaped canals (19, 20).
The collected data were analyzed by SPSS version 23. Descriptive statistics were reported for the prevalence and demographic features of the samples, and the Chi-square test was run to find differences between the variables at a significance level of 0.05.
Results
Canal configuration:
According to the Vertucci's classification, type II was the most common in the MB roots of MFMs, followed by type I and type IV in both males and females. On the other hand, the most prevalent types in the MB root of MSMs were types I, II, and IV, respectively in both sexes. All palatal and distobuccal (DB) roots of MFMs and MSMs demonstrated Vertucci's type I configuration (Table 1, Figures 1A, 1B, and 2).
The frequency of MB2 canal of MFMs was 67.4% and 76.1% in females and males, respectively; while these values were 31.3% and 43.7%, respectively in MSMs. Although the frequency of MB2 canals in MFMs and MSMs was greater in males than females, the difference was not statistically significant (P>0.05). Altogether, MB2 canals were discovered in 71.3% of MFMs and 37.1% of MSMs.
Number of root canals:
Table 2 illustrates the frequency of canals in maxillary molars. Accordingly, 28.7% of MFMs had three, and 71.3% had four root canals. MSMs with three root canals had the highest prevalence in both males and females. Of 375 MSMs, 2 (0.5%), 11 (2.9%), 223 (59.5%), and 139 (37.1%) had one, two, three, and four canals, respectively. The difference was not significant between males and females(P>0.05).
Number of roots:
Each MFM had three distinct roots;
whereas, most MSMs (95.7%) had three roots (only 2.7% had two roots). Table 3 shows MSMs with one (0.8%) and four (0.8%) roots.
Since teeth with fused roots and C-shaped canals cannot be classified according to the Vertucci's classification, they were reported separately. C-shaped canals were observed in 5 MSMs (1.2%), and 5.4% had fused root (14 females and 8 males) (Figure 3).
Table 1: Configuration of the root canal system in the mesiobuccal root of maxillary first and second molars by gender
{kind=link}
Figure 1A, 1B: Axial view of CBCT scans showing different root canal configurations in the mesiobuccal root of maxillary molars
{kind=link}
Figure 2: Cross-sectional view of CBCT scans showing different root canal configurations in the mesiobuccal root of maxillary molars
{kind=link}
Table 2: Distribution of the number of canals in maxillary first and second molars by gender
{kind=link}
Table 3: Number of roots in maxillary second molars by gender
{kind=link}
Figure 3: C-shaped and fused root canal configurations in maxillary second molars (A: Type V, B: Type II, C:Type III, D: Type VII)
{kind=link}
Discussion
This study assessed the morphology, number, and configuration of maxillary molar roots and canals according to the Vertucci’s classification using CBCT. The findings of the current study demonstrated that type II and type I were the most frequent in MB roots of MFMs and MSMs, respectively. Type I configuration was discovered in all palatal roots of the samples. Four root canals were found in 71.3% of MFMs. All MFMs had three roots, as did 95.7% of MSMs.
Permanent MFMs and MSMs have the highest complexities and variations in the root canal system; therefore, they have the highest failure rate in endodontic treatment and are a challenge for dental clinicians (21). In the present study, the morphology and anatomy of MFMs and MSMs were evaluated using CBCT.
The current investigation found that type II (43.1%), followed by type I (28.7%) and type IV (19.8%), were the most frequent canal types. Similarly, Al Mheiri et al. (5) evaluated an Emirati population and Alrahabi et al. studied a Saudi population and claimed that most of the MB roots were type II, type I, and type IV, respectively(22). Contrastingly, a previous study on an Iranian population discovered that the commonest types were type II (53.1%) and type I (29.8%) in the MB root of MFMs (6). In contrast to the present study, Kim et al. (23) evaluated a Korean population and Ratanajirasut et al. (24) assessed a Thai population using CBCT, and demonstrated type I to be the most frequent. One reason for such variations in the results can be the racial differences.
In the MB root of MSMs in the current study, the commonest types were type I (63.5%) and type II (18.7%). Correspondingly, Kim et al. (23) revealed that out of 644 MSMs, 63.48% were type I and 16.6% were type II. According to Ratanajirasut et al. (24), the most frequent canal morphology in the MB roots of MSMs was type I (70.6%) followed by type II (14.6%). On the other hand, Xia et al. (25) in their study on a Chinese population used CBCT and demonstrated that the MB root of 74.25% of MSMs was type I, followed by type IV (16.25%.). In contrast to the present results, Naseri et al. (26) found that in MB roots of MFMs of an Iranian population, type IV had the highest and type III had the lowest frequency.
This study revealed that in all palatal and DB roots of MFMs and MSMs, one single canal (type I) was observed. In a study by Al Mheiri et al.(5), only 1.2% and 2% of the examined teeth showed type II in the palatal and DB roots, respectively. Single canal configuration (type I) was more prevalent in these roots. Moreover, Alrahabi et al. (22) revealed that all DB and palatal roots of the examined teeth in their study were type I. Likewise, Ratanajirasut et al. (24) reported type I canal configuration as the most frequent in MFMs and MSM DB and palatal roots. In the study by Naseri et al. (26), type I and V palatal root canals had the highest and lowest frequency, respectively, in MFMs. In the DB roots, type I with the highest prevalence and type V with the lowest prevalence were the only observed canal types. Consistent with the present study, type I root canals were the most frequent in palatal and DB roots.
Ghoncheh et al. (27) used CBCT and suggested that in MFMs, type I had the highest and type V had the lowest frequency in MB and DB roots. All palatal roots were type I. In MSMs, type I and type II had the highest and lowest prevalence in MB roots, respectively. Additionally, all DB and palatal roots were type I. However, in the current study, the most frequent root canal type morphology in the MB root of MFMs was type II. The prevalence of type I root canal in the MB root of MSMs and the frequency of type I root canal in palatal and distal canals were consistent with the results of the present study.
In line with the present findings, Naseri et al. (26) did not discover any significant correlation between root canal configuration and age or gender. Similar to Pawar et al. (28) and Al Mheiri et al. (5), this study demonstrated that sex had no significant effect on canal configuration in maxillary molars' MB root.
Regarding the number of roots, all (100%) MFMs in the current study had three separate roots. The findings of the current study were consistent with those of Goncheh et al. (27) who reported 3 separate root morphology as the most prevalent morphology in MFMs and MSMs; however, the frequency of 3 separate roots in MFMs and MSMs in the current study was higher. Correspondingly, Zhang et al. (29) and Ghobashy et al. (20) discovered that all MFMs examined by CBCT had three roots. Moreover, after examining 974 MFMs, Pawar et al. (28) found that 99.1% had three and 0.8% had two roots. Another study by Kalender et al. (30) showed that 97.8% of the teeth had three, only 0.5% had two, and 1.6% had four roots. Finally, Ratanajirasut et al. (24) showed that out of 476 MFMs, 99.8% had three, and only one case (0.2%) had four roots.
In the present study, MSMs showed more variations in the morphology and number of roots compared to MFMs. Most MSMs had three (95.7%), while only 2.7% had two roots. However, MSMs with one (0.8%) and four (0.8%) roots were also found.
Zhang et al. (29) showed that out of 210 MSMs, 10% had one root, 9% had two, and 82% had three separate roots. However, the present study revealed no MSM with four roots. In a study by Kalender et al. (30), 3.1% of the teeth had one, 5.9% had two, 89.4% had three, and 1.3% had four roots.
Ratanajirasut et al. (24) demonstrated that among 457 MSMs, the percentage of one, two, three, and four rooted teeth was 3.5%, 9.2%, 87.1%, and 0.2%, respectively.
The present study showed that 71.3% of MFMs and 36.6% of MSMs exhibited the MB2 canal. In other studies conducted on the Iranian population, including the study by Khosravifard et al. (31), the authors discovered MB2 canals in 44.8% of MFMs and 18.5% of MSMs. Naseri et al. (26) claimed the presence of MB2 canals in 86.6% of the studied MB roots. Variations in methodologies, study protocols (in vivo or in vitro), sample size, techniques used to identify canal configurations, and study population's age, gender, and ethnicity all contribute to the difference in the incidence of MB2 canals (32). Martins et al. (33) calibrated observers from 21 regions to obtain a similar CBCT evaluation methodology. The results showed that the frequency of MB2 canal varied from 48.0% to 97.6% across regions, with a global frequency of 73.8%. Moreover, Singh and Pawar (34) used the dye penetration and clearing technique and found that 18% of MSMs and 28% of MFMs had MB2 canals. The prevalence of MB2 canals reported in their study was lower than that in the present study. Khademi et al. (6) examined 389 MFMs and 460 MSMs in an Iranian population using CBCT. The frequency of MB2 canal in MFMs and MSMs was reported to be 70.2% and 43.4%, respectively.
There is controversy regarding the effect of gender on the prevalence of MB2 canal. Mohara et al. (35) in their study on a Brazilian population observed that the frequency of MB2 canal in MSMs was significantly higher in females than males. In contrast, Kim et al. (23), in their study on a Korean population reported that males predominated females in the frequency of MB2 canal in MFMs, while no gender difference was observed in MB2 canals of MSMs. In line with the current study, Ghobashy et al. (20) showed that the MB2 canal was not affected by gender. In the present investigation, the frequency of MB2 in both MFMs and MSMs was slightly higher in males than females; nevertheless, the difference was not statistically significant.
Endodontic treatment of MFMs is considered difficult owing to the complex anatomy and high frequency of MB2 canal (5). CBCT offers a non-invasive approach for identifying anatomical variations of root canals. Nevertheless, CBCT imaging should be used only when complex morphology or anatomy is suspected. Intraoperative CBCT imaging is always an excellent choice when unexpected complex anatomy is observed after access cavity preparation or when canals are not discovered (28).
Conclusion
All MFMs and most MSMs had three roots in the present study. A higher prevalence of type II and type I canal configurations was observed In the MB root of MFMs and MSMs, respectively.
All DB and palatal roots presented type I configuration. The incidence of MB2 canal was higher in MFMs than in MSMs. There was no significant relationship between gender and presence of MB2.
Acknowledgement
The authors would like to thank the Research Center and Research Vice-Chancellor of Mazandaran University of Medical Sciences for their cooperation in implementation of this research project.
The present study showed that 71.3% of MFMs and 36.6% of MSMs exhibited the MB2 canal. In other studies conducted on the Iranian population, including the study by Khosravifard et al. (31), the authors discovered MB2 canals in 44.8% of MFMs and 18.5% of MSMs. Naseri et al. (26) claimed the presence of MB2 canals in 86.6% of the studied MB roots. Variations in methodologies, study protocols (in vivo or in vitro), sample size, techniques used to identify canal configurations, and study population's age, gender, and ethnicity all contribute to the difference in the incidence of MB2 canals (32). Martins et al. (33) calibrated observers from 21 regions to obtain a similar CBCT evaluation methodology. The results showed that the frequency of MB2 canal varied from 48.0% to 97.6% across regions, with a global frequency of 73.8%. Moreover, Singh and Pawar (34) used the dye penetration and clearing technique and found that 18% of MSMs and 28% of MFMs had MB2 canals. The prevalence of MB2 canals reported in their study was lower than that in the present study. Khademi et al. (6) examined 389 MFMs and 460 MSMs in an Iranian population using CBCT. The frequency of MB2 canal in MFMs and MSMs was reported to be 70.2% and 43.4%, respectively.
There is controversy regarding the effect of gender on the prevalence of MB2 canal. Mohara et al. (35) in their study on a Brazilian population observed that the frequency of MB2 canal in MSMs was significantly higher in females than males. In contrast, Kim et al. (23), in their study on a Korean population reported that males predominated females in the frequency of MB2 canal in MFMs, while no gender difference was observed in MB2 canals of MSMs. In line with the current study, Ghobashy et al. (20) showed that the MB2 canal was not affected by gender. In the present investigation, the frequency of MB2 in both MFMs and MSMs was slightly higher in males than females; nevertheless, the difference was not statistically significant.
Endodontic treatment of MFMs is considered difficult owing to the complex anatomy and high frequency of MB2 canal (5). CBCT offers a non-invasive approach for identifying anatomical variations of root canals. Nevertheless, CBCT imaging should be used only when complex morphology or anatomy is suspected. Intraoperative CBCT imaging is always an excellent choice when unexpected complex anatomy is observed after access cavity preparation or when canals are not discovered (28).
Conclusion
All MFMs and most MSMs had three roots in the present study. A higher prevalence of type II and type I canal configurations was observed In the MB root of MFMs and MSMs, respectively.
All DB and palatal roots presented type I configuration. The incidence of MB2 canal was higher in MFMs than in MSMs. There was no significant relationship between gender and presence of MB2.
Acknowledgement
The authors would like to thank the Research Center and Research Vice-Chancellor of Mazandaran University of Medical Sciences for their cooperation in implementation of this research project.
Type of Study: Original article |
Subject:
Endodontics
References
1. Ahmad IA, Alenezi MA. Root and Root Canal Morphology of Maxillary First Premolars: A Literature Review and Clinical Considerations. J Endod. 2016 Jun;42(6):861-72. [DOI:10.1016/j.joen.2016.02.017] [PMID]
2. Al-Zubaidi SM, Almansour MI, Al Mansour NN, Alshammari AS, Alshammari AF, Altamimi YS, Madfa AA. Assessment of root morphology and canal configuration of maxillary premolars in a Saudi subpopulation: a cone-beam computed tomographic study. BMC Oral Health. 2021 Aug 13;21(1): 397. [DOI:10.1186/s12903-021-01739-1] [PMID] []
3. Ghasemi N, Rahimi S, Shahi S, Samiei M, Frough Reyhani M, Ranjkesh B. A Review on Root Anatomy and Canal Configuration of the Maxillary Second Molars. Iran Endod J. 2017 Winter;12(1):1-9.
4. Shenoi RP, Ghule HM. CBVT analysis of canal configuration of the mesio-buccal root of maxillary first permanent molar teeth: An in vitro study. Contemp Clin Dent. 2012 Jul;3(3): 277-81. [DOI:10.4103/0976-237X.103618] [PMID] []
5. Al Mheiri E, Chaudhry J, Abdo S, El Abed R, Khamis AH, Jamal M. Evaluation of root and canal morphology of maxillary permanent first molars in an Emirati population; a cone-beam computed tomography study. BMC Oral Health. 2020 Oct 7;20(1):274. [DOI:10.1186/s12903-020-01269-2] [PMID] []
6. Khademi A, Zamani Naser A, Bahreinian Z, Mehdizadeh M, Najarian M, Khazaei S. Root Morphology and Canal Configuration of First and Second Maxillary Molars in a Selected Iranian Population: A Cone-Beam Computed Tomography Evaluation. Iran Endod J. 2017 Summer;12(3): 288-92.
7. Sadeghi M, Sadr Lahijani M. An in vitro study on root canal anatomy in maxillary molars. J Islam Dent Assoc Iran 2004; 16(49):14-21.
8. Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first mo-lar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969 Sep;28(3):419-25. [DOI:10.1016/0030-4220(69)90237-0] [PMID]
9. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984 Nov;58(5):589-99. [DOI:10.1016/0030-4220(84)90085-9] [PMID]
10. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol. 1972 Jan;33(1):101-10. [DOI:10.1016/0030-4220(72)90214-9] [PMID]
11. Fan B, Gao Y, Fan W, Gutmann JL. Identification of a C-shaped canal system in mandibular second molars-part II: the effect of bone image superimposition and intraradicular con-trast medium on radiograph interpretation. J Endod. 2008 Feb;34(2):160-5. [DOI:10.1016/j.joen.2007.10.010] [PMID]
12. Park JW, Lee JK, Ha BH, Choi JH, Perinpanayagam H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using mi-cro-computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Sep;108(3):437-42. [DOI:10.1016/j.tripleo.2009.01.022] [PMID]
13. Wolf TG, Paqué F, Woop AC, Willershausen B, Briseño-Marroquín B. Root canal morphology and configuration of 123 maxillary second molars by means of mi-cro-CT. Int J Oral Sci. 2017 Mar;9(1):33-7. [DOI:10.1038/ijos.2016.53] [PMID] []
14. Weng XL, Yu SB, Zhao SL, Wang HG, Mu T, Tang RY, Zhou XD. Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: a new modified root canal staining technique. J Endod. 2009 May;35(5):651-6. [DOI:10.1016/j.joen.2009.02.010] [PMID]
15. Levin MD. Endodontics Using Cone Beam Computed Tomography. Cone Beam Computed To-mography 2013. p. 211-47. [DOI:10.1002/9781118769027.ch10]
16. Deepak BS, Subash TS, Narmatha VJ, Anamika T, Snehil TK, Nandini DB. Imaging techniques in endodontics: an overview. J Clin Imaging Sci. 2012;2:13. [DOI:10.4103/2156-7514.94227] [PMID] []
17. Karobari MI, Noorani TY, Halim MS, Ahmed HMA. Root and canal morphology of the anterior permanent dentition in Malay-sian population using two classification systems: A CBCT clini-cal study. Aust Endod J. 2021 Aug;47(2):202-16. [DOI:10.1111/aej.12454] [PMID]
18. Kantilieraki E, Delantoni A, Angelopoulos C, Beltes P. Evalua-tion of Root and Root Canal Morphology of Mandibular First and Second Molars in a Greek Population: A CBCT Study. Eur Endod J. 2019 Jul 18;4(2):62-68. [DOI:10.14744/eej.2019.19480] [PMID] []
19. Grove CJ. The biology of multi-canaliculated roots. Dent Cosmos. 1916;58:728-33.
20. Ghobashy AM, Nagy MM, Bayoumi AA. Evaluation of Root and Canal Morphology of Maxillary Permanent Molars in an Egyptian Population by Cone-beam Computed Tomography. J Endod. 2017 Jul;43(7):1089-1092.. [DOI:10.1016/j.joen.2017.02.014] [PMID]
21. Betancourt P, Navarro P, Muñoz G, Fuentes R. Prevalence and location of the secondary mesiobuccal canal in 1,100 maxil-lary molars using cone beam computed tomography. BMC Med Imaging. 2016 Dec 1;16(1):66. [DOI:10.1186/s12880-016-0168-2] [PMID] []
22. Alrahabi M, Sohail Zafar M. Evaluation of root canal morphology of maxillary molars using cone beam computed tomography. Pak J Med Sci. 2015 Mar-Apr;31(2):426-30. [DOI:10.12669/pjms.312.6753] [PMID] []
23. Kim Y, Lee SJ, Woo J. Morphology of maxillary first and sec-ond molars analyzed by cone-beam computed tomography in a korean population: variations in the number of roots and canals and the incidence of fusion. J Endod. 2012 Aug;38(8):1063-8. [DOI:10.1016/j.joen.2012.04.025] [PMID]
24. Ratanajirasut R, Panichuttra A, Panmekiate S. A Cone-beam Computed Tomographic Study of Root and Canal Morphology of Maxillary First and Second Permanent Molars in a Thai Population. J Endod. 2018 Jan;44(1):56-61. [DOI:10.1016/j.joen.2017.08.020] [PMID]
25. Xia Y, Qiao X, Huang YJ, Li YH, Zhou Z. Root Anatomy and Root Canal Morphology of Maxillary Second Permanent Molars in a Chongqing Population: A Cone-Beam Computed Tomography Study. Med Sci Monit. 2020 Aug 18;26:e 922794. [DOI:10.12659/MSM.922794]
26. Naseri M, Safi Y, Akbarzadeh Baghban A, Khayat A, Eftekhar L. Survey of Anatomy and Root Canal Morphology of Maxillary First Molars Regarding Age and Gender in an Iranian Population Using Cone-Beam Computed Tomography. Iran Endod J. 2016 Fall;11(4):298-303.
27. Ghoncheh Z, Zade BM, Kharazifard MJ. Root Morphology of the Maxillary First and Second Molars in an Iranian Population Using Cone Beam Computed Tomography. J Dent (Tehran). 2017 May;14(3):115-22.
28. Pawar A, Thakur B, Machado R, Kwak SW, Kim HC. An In-Vivo cone-beam computed tomography analysis of root and canal morphology of maxillary first permanent molars in an Indian population. Indian J Dent Res. 2021 Jan-Feb;32(1): 104-9. [DOI:10.4103/ijdr.IJDR_782_19] [PMID]
29. Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J. 2011 Feb;44(2):162-9. [DOI:10.1111/j.1365-2591.2010.01826.x] [PMID]
30. Kalender A, Celikten B, Tufenkci P, Aksoy U, Basmacı F, Ke-lahmet U, et al. Cone beam computed tomography evaluation of maxillary molar root canal morphology in a Turkish Cypriot population. Biotechnology & Biotechnological Equipment. 2016;30(1):145-50. [DOI:10.1080/13102818.2015.1092885]
31. Khosravifard N, Kajan ZD, Hasanpoor H. Cone beam comput-ed tomographic survey of the mesiobuccal root canal anatomy in the maxillary first and second molar teeth of an Iranian popu-lation. Eur J Dent. 2018 Jul-Sep;12(3):422-7. [DOI:10.4103/ejd.ejd_60_18] [PMID] []
32. Olczak K, Pawlicka H. The morphology of maxillary first and second molars analyzed by cone-beam computed tomography in a polish population. BMC Med Imaging. 2017 Dec 29;17(1):68. [DOI:10.1186/s12880-017-0243-3] [PMID] []
33. Martins JNR, Alkhawas MAM, Altaki Z, Bellardini G, Berti L, Boveda C, et al. Worldwide Analyses of Maxillary First Molar Second Mesiobuccal Prevalence: A Multicenter Cone-beam Computed Tomographic Study. J Endod. 2018 Nov;44(11):1641-1649.e1. [DOI:10.1016/j.joen.2018.07.027] [PMID]
34. Singh S, Pawar M. Root canal morphology of South Asian Indian maxillary molar teeth. Eur J Dent. 2015 Jan-Mar; 9 (1):133-44. [DOI:10.4103/1305-7456.149662] [PMID] []
35. Mohara NT, Coelho MS, de Queiroz NV, Borreau MLS, Nish-ioka MM, de Jesus Soares A, Frozoni M. Root Anatomy and Canal Configuration of Maxillary Molars in a Brazilian Subpopulation: A 125-μm Cone-Beam Computed Tomographic Study. Eur J Dent. 2019 Feb;13(1):82-7. [DOI:10.1055/s-0039-1688736] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |