Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 286-290 |
Back to browse issues page


Ethics code: Not Applicable
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Shirani A M, Khosravi M, Ardestani M, Ashtari F. Pemphigus Vulgaris in a Patient with Multiple
Sclerosis: A Case Report with 7 Years of Follow Up. J Res Dent Maxillofac Sci 2023; 8 (4) :286-290
URL: http://jrdms.dentaliau.ac.ir/article-1-477-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-477-en.html



1- Department of Oral Medicine, School of Dentistry, Isfahan Branch, Islamic Azad University, Isfahan, Iran
2- Faculty of Dentistry, Isfahan Branch, Islamic Azad University, Isfahan, Iran ,khosravi.mari@yahoo.com
3- Faculty of Dentistry, Isfahan Branch, Islamic Azad University, Isfahan, Iran
4- Neurosurgery Department, Medical Faculty, Isfahan University of Medical Sciences, Isfahan, Iran
2- Faculty of Dentistry, Isfahan Branch, Islamic Azad University, Isfahan, Iran ,
3- Faculty of Dentistry, Isfahan Branch, Islamic Azad University, Isfahan, Iran
4- Neurosurgery Department, Medical Faculty, Isfahan University of Medical Sciences, Isfahan, Iran
Full-Text [PDF 648 kb]
(959 Downloads)
| Abstract (HTML) (2459 Views)
Introduction
A 40-year-old female was referred to the Oral Medicine Department of School of Dentistry, Isfahan Branch of IAU in 2014 with a chief complaint of ulcers in anterior labial gingiva of the mandible from 6 months earlier (Figure 1). Her medical history revealed that she had MS from 2004 and was under treatment by a neurologist. Since 2011, interferon (IFN) beta 1-b=betaferon (250 mcg/mL subcutaneous injections every other day) had been started for her and after 2 years (in 2014) IFN-beta 1-a=Avonex (30 mcg intramuscular injections weekly) was also added to her treatment regimen. She also had iron deficiency anemia. Desquamative gingivitis and ulceration in her anterior mandibular gingiva were noted but the oral mucosa was normal in other areas (Figure 1).
Figure 1. Desquamative gingivitis
Skin and other mucosa were also normal. Clinically, the lesions were similar to benign mucous membrane pemphigoid but the ikolsky’s sign was positive; thus, PV or drug-induced pemphigus related to INF-beta administration was more likely.
Biopsy was done and PV was reported. Indirect immunoassay was conducted and antibody against desmoglein III was found.
Since her MS was under control with this medication and PV was mild, the dug was not changed by her neurologist and PV was controlled by administration of 50 mg prednisolone daily (to be taken in the morning), 100 mg azathioprine daily bid for 2 weeks and Ca-D supplementation every 3 days and folic acid supplementation daily [11]. Prednisolone and azathioprine are used as the gold standard for treatment of pemphigus but as the signs and symptoms were insignificant and she was taking an immunosuppressive drug for MS, the corticosteroid dosage and durations were modified for the patient compared with the standard dosage routinely administered for pemphigus. The prednisolone dosage was then tapered by 10 mg/week for 2-week periods to reach 20 mg per day and then azathioprine was used (1 tablet per night) for 2 weeks. Next, prednisolone was tapered to 5 mg per day and then after 2 weeks azathioprine was discontinued, and PV was controlled with 5 mg prednisolone daily for years [11]. A corticosteroid mouthwash [a specific mouthwash was prepared by a pharmacist that included 16 mg betamethasone (12 amp), nystatin suspension (100,000 U/mL) (1 suspension), and 240 mL of milk of magnesia (1 bottle)]. This combination is presented in reference books but 16 mg betamethasone was selected for this patient as instructed by her oral medicine specialist. The patient was instructed to swish the mouthwash after each meal for 15 minutes (as instructed by her oral medicine specialist). As association of MS and PV is rare, no recommendations were found regarding the medications of choice, and this drug combination was selected by her oral medicine specialist.
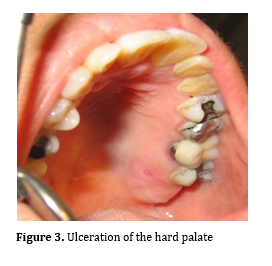
At the times of relapse of PV (2016, 2017, 2018 and 2019), the prednisolone dosage was increased between 15-40 mg per day for 2 weeks and was then tapered to 5 mg per day. Other oral mucosal sites (buccal mucosa and palate) were also involved over the years with small shallow ulcers (Figures 2 and 3).
Figure 2. Ulcer on the buccal mucosa
Figure 3. Ulceration of the hard palate
In 2018, the patient developed hand tremor. Her neurologist suspected possible corticosteroid-related myopathy; thus, prednisolone was discontinued, but it had no effect on the tremor, and PV relapsed. Thus, prednisolone was started again. Hand tremor was diagnosed to be related to progression of MS. Her neurologist discontinued INF-beta, and dimethyl fumarate (Diphosel) (240 mg capsules every 12 hours) was prescribed to control MS. The pemphigus lesions reappeared occasionally as small ulcers indicating that PV was not related to INF-beta administration.
In 2020, her neurologist prescribed rituximab (100 mg/10 mL injections every 6 months) to control MS. As rituximab is also used to control pemphigus, prednisolone was discontinued and pemphigus was completely controlled. It has now been 1.5 years with no development of a new lesion, and anti-desmoglein 1 and 3 have been negative. Alterations in the level of anti-desmoglein 3 through the years are presented in Figure 4.
Figure 4. Alterations in the level of anti-desmoglein 3 within 7 years
Discussion
It is necessary to pay attention to mild oral ulcers in MS patients because they may be related to severe blistering diseases like pemphigus or immunosuppressive drugs used for treatment of MS and this may cause misdiagnosis and mistreatment. Rituximab in the present patient showed good results to control both MS and PV.
Full-Text: (1401 Views)
|
Abstract
Background and Aim: Pemphigus vulgaris (PV) is a severe life-threatening autoimmune disease that causes intraepithelial blisters. PV has been reported in association with some autoimmune diseases. But only few cases (fewer than 10 reports according to literature search) have been reported regarding the association of PV with multiple sclerosis (MS). MS is a life-threatening, inflammatory demyelinating disease, causing severe disability.
Case Presentation: Our patient was a 40-year-old female complaining of gingival ulcers. She had MS for the past 10 years. Biopsy and immunoassay were done and PV was confirmed. The patient has been followed up for 7 years so far. Conclusion: It is necessary to pay attention to mild oral ulcers in MS patients because they may be related to severe blistering diseases like PV. Key Words: Pemphigus; Multiple Sclerosis; Oral Ulcer |
Introduction
Pemphigus vulgaris (PV) is an autoimmune dermatosis characterized by blistering of the epidermis and/or mucous membranes. The affected patients develop autoantibodies against the desmoglein 1 and/or desmoglein 3 adhesion molecules [1]. It usually occurs between the 4th and 6th decades of life [2]. The etiology of PV has a complex polygenic basis, involving multiple genetic and environmental factors. Most predisposing factors directly originate from the environment (e.g., drug intake, viral infections, physical stimuli, contact allergens, and diet) [3]. PV may be accompanied by some autoimmune disorders [4].
Multiple sclerosis (MS) is a life-threatening, inflammatory demyelinating disease, causing neuronal cell death in the central nervous system. It affects more than two million people Worldwide [5,6]. The neurological condition in MS causes painful motor and sensory disturbances. Although the etiology of MS is still unknown, some factors can be named as risk factors such as geographical location and environmental factors. Environmental factors such as vitamin D deficiency, cigarette smoking, and infectious agents may be implicated in the development of MS as well. The progression and symptoms of MS are unpredictable. MS is usually associated with pain such as orofacial pain, trigeminal neuralgia, myofascial palsy, and neck pain. The prevalence of migraine is also three times higher in patients with MS than in the general population. Many of the medications used for symptomatic management of MS have the potential to cause dry mouth and associated oral diseases [7, 8].
According to the literature, occurrence of oral PV in MS patients is rare (fewer than 10 reports available in this respect) [9,10]. Herein, a patient with MS and PV is reported with 7 years of follow up, and a review of the literature is also performed.
Case Presentation
Multiple sclerosis (MS) is a life-threatening, inflammatory demyelinating disease, causing neuronal cell death in the central nervous system. It affects more than two million people Worldwide [5,6]. The neurological condition in MS causes painful motor and sensory disturbances. Although the etiology of MS is still unknown, some factors can be named as risk factors such as geographical location and environmental factors. Environmental factors such as vitamin D deficiency, cigarette smoking, and infectious agents may be implicated in the development of MS as well. The progression and symptoms of MS are unpredictable. MS is usually associated with pain such as orofacial pain, trigeminal neuralgia, myofascial palsy, and neck pain. The prevalence of migraine is also three times higher in patients with MS than in the general population. Many of the medications used for symptomatic management of MS have the potential to cause dry mouth and associated oral diseases [7, 8].
According to the literature, occurrence of oral PV in MS patients is rare (fewer than 10 reports available in this respect) [9,10]. Herein, a patient with MS and PV is reported with 7 years of follow up, and a review of the literature is also performed.
Case Presentation
A 40-year-old female was referred to the Oral Medicine Department of School of Dentistry, Isfahan Branch of IAU in 2014 with a chief complaint of ulcers in anterior labial gingiva of the mandible from 6 months earlier (Figure 1). Her medical history revealed that she had MS from 2004 and was under treatment by a neurologist. Since 2011, interferon (IFN) beta 1-b=betaferon (250 mcg/mL subcutaneous injections every other day) had been started for her and after 2 years (in 2014) IFN-beta 1-a=Avonex (30 mcg intramuscular injections weekly) was also added to her treatment regimen. She also had iron deficiency anemia. Desquamative gingivitis and ulceration in her anterior mandibular gingiva were noted but the oral mucosa was normal in other areas (Figure 1).
Figure 1. Desquamative gingivitis
{kind=link}
Skin and other mucosa were also normal. Clinically, the lesions were similar to benign mucous membrane pemphigoid but the ikolsky’s sign was positive; thus, PV or drug-induced pemphigus related to INF-beta administration was more likely.
Biopsy was done and PV was reported. Indirect immunoassay was conducted and antibody against desmoglein III was found.
Since her MS was under control with this medication and PV was mild, the dug was not changed by her neurologist and PV was controlled by administration of 50 mg prednisolone daily (to be taken in the morning), 100 mg azathioprine daily bid for 2 weeks and Ca-D supplementation every 3 days and folic acid supplementation daily [11]. Prednisolone and azathioprine are used as the gold standard for treatment of pemphigus but as the signs and symptoms were insignificant and she was taking an immunosuppressive drug for MS, the corticosteroid dosage and durations were modified for the patient compared with the standard dosage routinely administered for pemphigus. The prednisolone dosage was then tapered by 10 mg/week for 2-week periods to reach 20 mg per day and then azathioprine was used (1 tablet per night) for 2 weeks. Next, prednisolone was tapered to 5 mg per day and then after 2 weeks azathioprine was discontinued, and PV was controlled with 5 mg prednisolone daily for years [11]. A corticosteroid mouthwash [a specific mouthwash was prepared by a pharmacist that included 16 mg betamethasone (12 amp), nystatin suspension (100,000 U/mL) (1 suspension), and 240 mL of milk of magnesia (1 bottle)]. This combination is presented in reference books but 16 mg betamethasone was selected for this patient as instructed by her oral medicine specialist. The patient was instructed to swish the mouthwash after each meal for 15 minutes (as instructed by her oral medicine specialist). As association of MS and PV is rare, no recommendations were found regarding the medications of choice, and this drug combination was selected by her oral medicine specialist.
At the times of relapse of PV (2016, 2017, 2018 and 2019), the prednisolone dosage was increased between 15-40 mg per day for 2 weeks and was then tapered to 5 mg per day. Other oral mucosal sites (buccal mucosa and palate) were also involved over the years with small shallow ulcers (Figures 2 and 3).
Figure 2. Ulcer on the buccal mucosa
{kind=link}
Figure 3. Ulceration of the hard palate
{kind=link}
In 2018, the patient developed hand tremor. Her neurologist suspected possible corticosteroid-related myopathy; thus, prednisolone was discontinued, but it had no effect on the tremor, and PV relapsed. Thus, prednisolone was started again. Hand tremor was diagnosed to be related to progression of MS. Her neurologist discontinued INF-beta, and dimethyl fumarate (Diphosel) (240 mg capsules every 12 hours) was prescribed to control MS. The pemphigus lesions reappeared occasionally as small ulcers indicating that PV was not related to INF-beta administration.
In 2020, her neurologist prescribed rituximab (100 mg/10 mL injections every 6 months) to control MS. As rituximab is also used to control pemphigus, prednisolone was discontinued and pemphigus was completely controlled. It has now been 1.5 years with no development of a new lesion, and anti-desmoglein 1 and 3 have been negative. Alterations in the level of anti-desmoglein 3 through the years are presented in Figure 4.
Figure 4. Alterations in the level of anti-desmoglein 3 within 7 years
{kind=link}
Discussion
PV is an autoimmune disorder. It is postulated that autoreactive T cells are involved in induction and maintenance of auto-antibody production in PV[12,13].
Autoimmune bullous disorders (ABDs) encompass a number of heterogeneous conditions linked by the loss of tolerance to structural proteins of the skin. PV is among the diseases in the heterogeneous clinical spectrum of ABDs [14]. ABDs are usually diagnosed using three criteria: 1) the overall clinical picture, including patient history and physical examination, 2)histopathology, and 3) positive direct immunofluorescence microscopy [15].
PV may also be associated with other autoimmune diseases such as systemic lupus erythematosus, myasthenia gravis, rheumatoid arthritis, and pernicious anemia [16]. PV is a potentially life-threatening skin disorder that requires early recognition and prompt treatment 17,18]. The treatment plans for PV may include application of pastes, ointments and mouthwashes with systemic medications [19].
Drug-induced pemphigus is a rare type of drug eruption. Among drugs, thiol-containing drugs cause pemphigus foliaceus, and non-thiol drugs cause PV [20]. It is reported that INF can cause autoimmune reactions like PV, but in this case, after discontinuing it, no effects on the severity of PV were seen.
In this case, PV oral ulcers were mild and different from the usual form of PV. It may be related to intake of immunosuppressive medications for MS. Treatment for this patient was different from the routine treatment recommended for pemphigus in terms of drug dosage and duration of use. In the literature review, no similar condition in terms of severity and treatment modalities was found.
A previous study reported a 58-year-old female with MS who developed PV [10]. She had MS for 27 years and had paraplegia and bilateral paresis of the high limbs [20]. But in the present report, MS was controlled and the patient had mild symptoms.
Other case reports reported associations between pemphigoid and MS. A review of case reports and case series showed that pemphigus and pemphigoid were associated with autoimmune conditions, including myasthenia gravis, systemic lupus erythematosus, vitiligo, alopecia, polymyositis, and autoimmune thrombocytopenia. However, some others demonstrated conflicting results about such associations [21-28]. Recently, researchers published the results of a study that analyzed the association between pemphigus and 4 neurologic diseases namely dementia, Parkinson’s disease, epilepsy, and MS [29]. Another study reported possible association of pemphigus and autoimmune diseases such as MS [30].
Conclusion
Autoimmune bullous disorders (ABDs) encompass a number of heterogeneous conditions linked by the loss of tolerance to structural proteins of the skin. PV is among the diseases in the heterogeneous clinical spectrum of ABDs [14]. ABDs are usually diagnosed using three criteria: 1) the overall clinical picture, including patient history and physical examination, 2)histopathology, and 3) positive direct immunofluorescence microscopy [15].
PV may also be associated with other autoimmune diseases such as systemic lupus erythematosus, myasthenia gravis, rheumatoid arthritis, and pernicious anemia [16]. PV is a potentially life-threatening skin disorder that requires early recognition and prompt treatment 17,18]. The treatment plans for PV may include application of pastes, ointments and mouthwashes with systemic medications [19].
Drug-induced pemphigus is a rare type of drug eruption. Among drugs, thiol-containing drugs cause pemphigus foliaceus, and non-thiol drugs cause PV [20]. It is reported that INF can cause autoimmune reactions like PV, but in this case, after discontinuing it, no effects on the severity of PV were seen.
In this case, PV oral ulcers were mild and different from the usual form of PV. It may be related to intake of immunosuppressive medications for MS. Treatment for this patient was different from the routine treatment recommended for pemphigus in terms of drug dosage and duration of use. In the literature review, no similar condition in terms of severity and treatment modalities was found.
A previous study reported a 58-year-old female with MS who developed PV [10]. She had MS for 27 years and had paraplegia and bilateral paresis of the high limbs [20]. But in the present report, MS was controlled and the patient had mild symptoms.
Other case reports reported associations between pemphigoid and MS. A review of case reports and case series showed that pemphigus and pemphigoid were associated with autoimmune conditions, including myasthenia gravis, systemic lupus erythematosus, vitiligo, alopecia, polymyositis, and autoimmune thrombocytopenia. However, some others demonstrated conflicting results about such associations [21-28]. Recently, researchers published the results of a study that analyzed the association between pemphigus and 4 neurologic diseases namely dementia, Parkinson’s disease, epilepsy, and MS [29]. Another study reported possible association of pemphigus and autoimmune diseases such as MS [30].
Conclusion
It is necessary to pay attention to mild oral ulcers in MS patients because they may be related to severe blistering diseases like pemphigus or immunosuppressive drugs used for treatment of MS and this may cause misdiagnosis and mistreatment. Rituximab in the present patient showed good results to control both MS and PV.
Type of Study: Case report |
Subject:
Oral medicine
References
1. Chesworth BM, Hamilton CB, Walton DM, Benoit M, Blake TA, Bredy H, et al. Reliability and validity of two versions of the upper extremity functional index. Physiother Can. 2014 Sum-mer;66(3):243-53. [DOI:10.3138/ptc.2013-45] [PMID] []
2. Zawar V, Pawar M, Kumavat S. Recurrent Paronychia as a Presenting Manifestation of Pemphigus Vulgaris: A Case Report. Skin Appendage Disord. 2017 Mar;3(1):28-31. [DOI:10.1159/000455881] [PMID] []
3. Ruocco V, Ruocco E, Lo Schiavo A, Brunetti G, Guerrera LP, Wolf R. Pemphigus: etiology, pathogenesis, and inducing or trig-gering factors: facts and controversies. Clin Dermatol. 2013 Jul-Aug;31(4):374-81. [DOI:10.1016/j.clindermatol.2013.01.004] [PMID]
4. Kavala M, Kural E, Kocaturk E, Zindanci I, Turkoglu Z, Can B. The evaluation of thyroid diseases in patients with pemphigus vulgaris. ScientificWorldJournal. 2012;2012: 146897. [DOI:10.1100/2012/146897] [PMID] []
5. Cruickshank TM, Reyes AR, Ziman MR. A systematic review and meta-analysis of strength training in individuals with multiple sclerosis or Parkinson disease. Medicine (Baltimore). 2015 Jan;94(4):e411. [DOI:10.1097/MD.0000000000000411] [PMID] []
6. Dutta R, Trapp BD. Relapsing and progressive forms of multi-ple sclerosis: insights from pathology. Curr Opin Neurol. 2014 Jun;27(3):271-8. [DOI:10.1097/WCO.0000000000000094] [PMID] []
7. Zhang GQ, Meng Y. Oral and craniofacial manifestations of multiple sclerosis: implications for the oral health care provider. Eur Rev Med Pharmacol Sci. 2015 Dec;19(23): 4610-20.
8. McGraw CA, Lublin FD. Interferon beta and glatiramer acetate therapy. Neurotherapeutics. 2013 Jan;10(1):2-18. [DOI:10.1007/s13311-012-0163-4] [PMID] []
9. Meiner Z, Zlotogorski A, Brautbar C. Pemphigus associated with multiple sclerosis. Clin Exp Dermatol. 1992 May; 17(3): 217. [DOI:10.1111/j.1365-2230.1992.tb00213.x] [PMID]
10. Friedel J, Jeandel C, Abensour M, Heid E. Multiple sclerosis and autoimmune skin bullae: a case of pemphigus vul-garis. Dermatologica. 1987;175(3):159-60. [DOI:10.1159/000248818] [PMID]
11. Burket's oral medicine.Glick M,Greenberg M,Lockhart PB,ChallacombehSJ.Wiley Blackwell.13th edition,2021,61.
12. El-Darouti MA, Hegazy RA, Abdel Hay RM, El Hawary MS, Tawdy AM, Fawzy MM, et al. Study of T helper 1 and T helper 2 responses in pemphigus vulgaris patients receiving interferon alpha 2a injections in addition to a standard protocol therapy: a randomized controlled trial. Arch Dermatol Res. 2015 May;307(4):299-307. [DOI:10.1007/s00403-014-1522-2] [PMID]
13. Lee SH, Hong WJ, Kim SC. Analysis of Serum Cytokine Profile in Pemphigus. Ann Dermatol. 2017 Aug;29(4):438-45. [DOI:10.5021/ad.2017.29.4.438] [PMID] []
14. Kridin K. Pemphigus group: overview, epidemiology, mortal-ity, and comorbidities. Immunol Res. 2018 Apr;66(2): 255-70. [DOI:10.1007/s12026-018-8986-7] [PMID]
15. Pollmann R, Schmidt T, Eming R, Hertl M. Pemphigus: a Comprehensive Review on Pathogenesis, Clinical Presentation and Novel Therapeutic Approaches. Clin Rev Allergy Immunol. 2018 Feb;54(1):1-25. [DOI:10.1007/s12016-017-8662-z] [PMID]
16. Yoshimura K, Ishii N, Hamada T, Abe T, Ono F, Hashikawa K, et al. Clinical and immunological profiles in 17 Japanese patients with drug-induced pemphigus studied at Kurume University. Br J Dermatol. 2014 Sep;171(3):544-53. [DOI:10.1111/bjd.12925] [PMID]
17. Ramseur WL, Richards F, 2nd, Duggan DB. A case of fatal pemphigus vulgaris in association with beta interferon and interleukin-2 therapy. Cancer. 1989 May 15;63(10):2005-7.
https://doi.org/10.1002/1097-0142(19890515)63:10<2005::AID-CNCR2820631023>3.0.CO;2-P [DOI:10.1002/1097-0142(19890515)63:103.0.CO;2-P] [PMID]
18. Feliciani C, Cozzani E, Marzano AV, Caproni M, Di Zenzo G, Calzavara-Pinton P; "Cutaneous Immunology" group of SIDe-MaST. Italian Guidelines in Pemphigus - adapted from the Euro-pean Dermatology Forum (EDF) and European Academy of Dermatology and Venerology (EADV). G Ital Dermatol Venereol. 2018 Oct;153(5):599-608. [DOI:10.23736/S0392-0488.18.06073-X]
19. Feliciani C, Joly P, Jonkman MF, Zambruno G, Zillikens D, Ioannides D, Kowalewski C, Jedlickova H, Kárpáti S, Marinovic B, Mimouni D, Uzun S, Yayli S, Hertl M, Borradori L. Management of bullous pemphigoid: the European Dermatology Forum consensus in collaboration with the Euro-pean Academy of Dermatology and Venereology. Br J Dermatol. 2015 Apr;172(4):867-77. [DOI:10.1111/bjd.13717] [PMID]
20. Arpita R, Monica A, Venkatesh N, Atul S, Varun M. Oral Pem-phigus Vulgaris: Case Report. Ethiop J Health Sci. 2015 Oct;25(4):367-72. [DOI:10.4314/ejhs.v25i4.11]
21. Das D, Anand V, Khandpur S, Sharma VK, Sharma A. T helper type 1 polarizing gammadelta T cells and Scavenger receptors contribute to the pathogenesis of Pemphigus vulgaris. Immunology. 2018 Jan;153(1):97-104. [DOI:10.1111/imm.12814] [PMID] []
22. Narla S, Silverberg JI. Associations of pemphigus or pemphigoid with autoimmune disorders in US adult inpatients. J Am Acad Dermatol. 2020 Mar;82(3):586-95. [DOI:10.1016/j.jaad.2019.07.029] [PMID]
23. Ljubojević S, Lipozencić J, Brenner S, Budimcić D. Pemphigus vulgaris: a review of treatment over a 19-year peri-od. J Eur Acad Dermatol Venereol. 2002 Nov;16(6):599-603. [DOI:10.1046/j.1468-3083.2002.00504.x] [PMID]
24. Shabbir SG, Hassan M, Kazmi SA, Suhail S. Myasthenia gravis and pemphigus vulgaris. J Pak Med Assoc. 1984 Nov; 34(11):349-51.
25. Leshem YA, Katzenelson V, Yosipovitch G, David M, Mimouni D. Autoimmune diseases in patients with pemphigus and their first-degree relatives. Int J Dermatol. 2011 Jul;50(7):827-31. [DOI:10.1111/j.1365-4632.2010.04818.x] [PMID]
26. Langan SM, Groves RW, West J. The relationship between neurological disease and bullous pemphigoid: a population-based case-control study. J Invest Dermatol. 2011 Mar;131(3):631-6. [DOI:10.1038/jid.2010.357] [PMID]
27. Amber KT, Zikry J, Hertl M. A multi-hit hypothesis of bullous pemphigoid and associated neurological disease: Is HLA-DQB1*03:01, a potential link between immune privileged antigen exposure and epitope spreading? HLA. 2017 Mar;89(3):127-34. [DOI:10.1111/tan.12960] [PMID]
28. Daneshpazhooh M, Behjati J, Hashemi P, Shamohammadi S, Mortazavi H, Nazemi MJ, et al. Thyroid autoimmunity and pem-phigus vulgaris: is there a significant association? J Am Acad Dermatol. 2010 Feb;62(2):349-51. [DOI:10.1016/j.jaad.2009.05.024] [PMID]
29. Marrie RA, Reider N, Cohen J, Stuve O, Sorensen PS, Cutter G, et al. A systematic review of the incidence and preva-lence of autoimmune disease in multiple sclerosis. Mult Scler. 2015 Mar;21(3):282-93. [DOI:10.1177/1352458514564490] [PMID] []
30. Kridin K, Zelber-Sagi S, Comaneshter D, Cohen AD.Association Between Pemphigus and Neurologic Diseases. JAMA Dermatol. 2018 Mar 1;154(3):281-5. [DOI:10.1001/jamadermatol.2017.5799] [PMID] []
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |