

Volume 8, Issue 3 (8-2023)
J Res Dent Maxillofac Sci 2023, 8(3): 179-186 |
Back to browse issues page


Ethics code: IR.IAU.DENTAL.REC.1398.052
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Amini S, Fazlyab M, Moshari A A, Soltani N. Comparative Effects of Calcium Hydroxide in
Combination with Ciprofloxacin or Betamethasone Against Enterococcus Faecalis Biofilm. J Res Dent Maxillofac Sci 2023; 8 (3) :179-186
URL: http://jrdms.dentaliau.ac.ir/article-1-475-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-475-en.html



1- Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
2- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,soltaninika@yahoo.com
2- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,
Full-Text [PDF 1078 kb]
(561 Downloads)
| Abstract (HTML) (1598 Views)
Introduction
Elimination of root canal bacteria is a perquisite for a successful root canal treatment. To achieve this goal, a combination of mechanical and chemical irrigation is necessary [1]. However, not all bacteria are eliminated through chemomechanical preparation, and some species can survive in inaccessible areas of the canal such as delta, isthmi and dentinal tubules [2]. Application of inter-appointment canal medicaments may help to decrease these persistent bacteria [3].
Evidence shows that bacterial elimination may be achieved by the application of calcium hydroxide (CH) as an intra-canal medicament [1]. First suggested by Hermann in 1920, CH is the most commonly used medicament due to its denaturizing effects on proteins as well as its antimicrobial qualities that are believed to be due to its very high pH resulting from the dissociation of hydroxyl ions. Water must be present for the antimicrobial effect of CH [4]. The dissociation of CH particles allows the diffusion of hydroxyl and calcium ions through the dentinal tubules [5]. The high pH promotes microbial inhibition through an irreversible enzymatic reaction [6]. Not only does calcium act by clearing the carbon dioxide used by bacteria for anaerobic respiration [7], but also it has the ability to promote inactivation of bacterial lipopolysaccharides found in the outer membrane of Gram-negative bacteria [8]. The mechanism of action for this phenomenon is the increase in pH, which might stimulate genetic cascades that modify the characteristics of the bacterial cells [5]. However, the effects of CH are limited in persistent infections [9].
Enterococcus faecalis (E. faecalis), is a facultative anaerobic Gram-positive coccus and is the most commonly isolated species from teeth with persistent periapical lesions (predominantly in endodontic failures) [10]. However, more recent studies believe that CH is unable to kill E. faecalis [11]. Evidence shows that E. faecalis may benefit from a CH challenge and grow in mixed biofilms [12]. It has been demonstrated that, when exposed to calcium hydroxide, E. faecalis uses a proton pump which can drive protons to the cytoplasm of the bacterium [13] to control intracellular pH and confer resistance [5].
For this reason, combination of CH with antibiotics has been proposed to improve the action against this microorganism [5]. The use of triple (TAP) and double antibiotic paste (DAP) (a combination of metronidazole and ciprofloxacin with/without minocycline) during endodontic regeneration is an accepted and essential step [14]. Ciprofloxacin is classified as a second-generation fluoroquinolone and is effective against enteric bacteria such as Enterococcus species with high tubular penetration [15]. According to de Freitas et al, [5] the highest pH values were found for CH paste containing ciprofloxacin.
Another goal in root canal treatment is to reduce inflammation and post-treatment pain. Local steroids, systemic steroids and non-steroidal anti-inflammatory drugs were introduced to achieve this purpose [16]. It has been stated that local steroids like betamethasone do not change antibacterial effectiveness of CH against planktonic E. faecalis but there is no information about E. faecalis biofilm [17]. Conversely, some have reported the combination of CH with hydrocortisone being non effective against E. faecalis [18]. Also, it has been shown that antibacterial effectiveness of CH on E. faecalis improves in combination with non-steroidal anti-inflammatory drugs [5]. Considering the conflicting data, this study was designed to assess the antibacterial efficacy of CH alone and in combination with betamethasone and ciprofloxacin on intracanal 8-week biofilm of E. faecalis.
Materials and Methods
After approval by the ethics committee of the Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran (IR.IAU.DENTAL.REC.1398.064), this ex vivo study was conducted on 95 single-rooted extracted human teeth with mature apices. The teeth included in this study were extracted due to periodontal attachment loss, orthodontic purposes, or unrestorable crown. After surface cleaning and disinfection, the teeth were examined under a laboratory microscope (Stemi DV4 Spot; Carl Zeiss, Oberkochen, Germany) at ×20 magnification to exclude teeth with cracks, caries, or restoration. Digital radiographs were obtained from buccal and proximal directions for detection of any anatomical complexity, internal resorption, and calcification. Selected teeth had root curvatures not greater than 20 degrees according to the Schneider’s method [19].
The whole procedure included root canal preparation and sterilization, bacterial inoculation, incubation for biofilm formation for 8 weeks, preparation and application of intra-canal medicaments, and culturing and microbial analysis by means of counting the number of colony-forming units (CFUs).
Canal preparation:
The crowns were cut to prepare root lengths of 12 mm from cervical to apical. Canals from orifice to apex were prepared with # 1 to #3 Gates Glidden drills (Dentsply-Maillefer, Ballaigues, Switzerland). Afterwards, for smear layer removal, the canals were irrigated with 5 mL of 17% EDTA solution (Darupakhsh, Tehran, Iran) followed by 5 mL of 0.9% saline (Darupakhsh, Tehran, Iran) and then 5 mL of 5.25% NaOCl (Darupakhsh, Tehran, Iran). Teeth were autoclaved for 30 minutes and were incubated at 37ºC for 48 hours. Sterilization was repeated if any opacity was detected in brain heart infusion broth [1,2].
Biofilm formation:
Fresh suspension of E. faecalis (ATCC 29212) was obtained from the Biological Resource Center (Tehran, Iran) and incubated in fresh brain heart infusion broth (Merck, Darmstadt, Germany) in aerobic atmosphere at 37°C for 4-5 hours, until the optical density of 600 nm was adjusted to a concentration of 1.0×106 CFUs per milliliter (CFUs/mL), and was verified spectrophotometric ally (OD600: 0.01–0.02). This suspension was inoculated into the canals by a 30-gauge needle. The samples were incubated at 37ºC for 8 weeks while placed on a shaker operating at 150 rpm [1].
Biofilm control:
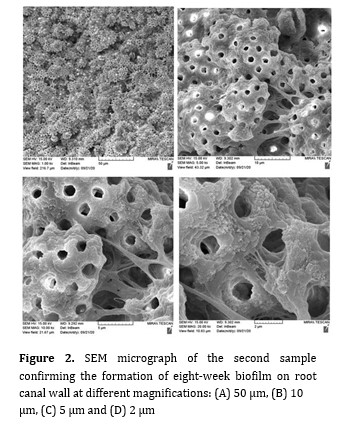
By the end of 8 weeks, two samples were randomly removed from the incubator, fixed and observed under a scanning electron microscope (SEM; Jeol-JSM 5600LV, Noran Instruments, Tokyo, Japan) at 15 kW, to confirm biofilm formation (Figures 1 and 2). Also, three samples were randomly selected to determine the number of pre-intervention CFUs. In order to determine the colony count, the biofilm was ultrasonically disrupted and transferred to phosphate buffer saline (Dulbecco's Modified Formula; ICN Biochemicals, England). After dilution, culture was prepared on agar medium, and incubated at 37ºC for 96 hours to count the primary number of CFUs [1].
Figure 1. SEM micrograph of the first sample confirming the formation of eight-week biofilm on root canal wall at different magnifications: (A) 50 µm, (B) 10 µm, (C) 5 µm and (D) 2 µm
Figure 2. SEM micrograph of the second sample confirming the formation of eight-week biofilm on root canal wall at different magnifications: (A) 50 µm, (B) 10 µm, (C) 5 µm and (D) 2 µm
Preparation and application of intracanal medicaments:
The samples were randomly divided into three groups:
Group 1 (CH + betamethasone) (n=30): one scoop (equal to 1.3 g) of CH powder (Pishro Dandan Co., Tehran, Iran) was mixed with 0.15 mL (3 drops) of 0.1% betamethasone eye drop (Abooreihan Co., Tehran, Iran). This mixture contained 0.00015 g betamethasone.
Group 2 (CH + ciprofloxacin) (n=30): one scoop (equal to 1.3 g) of CH powder (Pishro Dandan Co., Tehran, Iran) was mixed with 0.15 mL (3 drops) of 0.3% ciprofloxacin eye drop (Abooreihan Co., Tehran, Iran). This mixture contained 0.00045 g ciprofloxacin.
Group 3 (CH + saline) (n=30): one scoop (equal to 1.3 g) of CH powder (Pishro Dandan Co., Tehran, Iran) was mixed with 0.15 mL (3 drops) of saline.
The mixtures were delivered into the canals by means of a #30 lentulo spiral (Mani, Tochigi, Japan) [13].
Microbial analysis:
Microbial analysis and colony counting were performed at 1, 7 and 10 days. At each time point, 10 samples were selected from each group, and biofilm was disrupted by ultrasonication, and transferred to 0.9 mL of phosphate buffered saline (Dulbecco's Modified Formula; ICN Biochemicals, England). After dilution, the samples were spread on agar plate and incubated at 37ºC for 96 hours. After culture, the colony count was measured for the purpose of comparison with the primary colony count [13].
Statistical analysis:
The Kolmogorov-Smirnov test was conducted to assess the normality of data distribution. Accordingly, the comparison among the groups was performed by two-way ANOVA and a post-hoc test using SPSS version 20 (IBM SPSS Inc., Chicago, IL].
Results
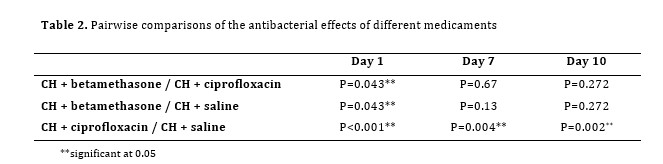
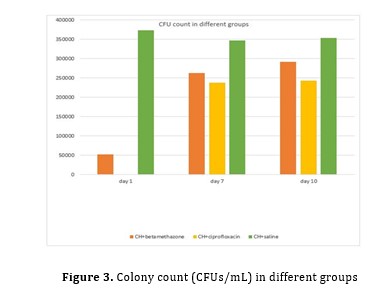
At 1 day, the highest colony count was observed in CH + betamethasone group followed by CH + saline, and the difference between them was highly significant (P<0.001). The difference between CH + betamethasone and CH + saline, and also the difference between CH + betamethasone and CH + ciprofloxacin was also significant in colony count (P=0.043).
At 7 and 10 days, the highest colony count was observed in CH + saline samples. While the difference between CH + ciprofloxacin and CH + betamethasone samples (P=0.67 at 7 days and P=0.272 at 10 days), and the difference between CH + betamethasone and CH + saline were not significant (P=0.13 at 7 days and P=0.272 at 10 days).
CH + ciprofloxacin group showed significantly lower colony count than CH + saline at 1 (P=0.001), 7 (P=0.004) and 10 (P=0.002) days (Tables 1 and 2; Figure 3).
Discussion
The present study evaluated the antibacterial effect of CH in combination with saline, betamethasone or ciprofloxacin on 8-week biofilm of E. faecalis in root canals of extracted human teeth. The results showed the lowest and the highest colony count in CH + ciprofloxacin and CH + saline groups, respectively. The combination of CH +betamethasone also showed some antibacterial activity. The alternative hypothesis behind the primary research question was confirmed: through colony counting, it was shown that combination of CH with ciprofloxacin or betamethasone improved the ex vivo antibacterial effects of CH paste on eight-week biofilm of E. faecalis.
When a carious lesion extends to the pulp chamber and the hard tissue barrier is breached, bacteria can invade the pulp tissue. In apical periodontitis, bacteria invade further and colonize the entire root canal system. Accordingly, to promote healing of apical periodontitis and cleaning of the root canal system, microorganisms within the root canal system must be eliminated.
Table 1. Mean colony count in the three groups at 1, 7 and 10 days
Table 2. Pairwise comparisons of the antibacterial effects of different medicaments
Figure 3. Colony count (CFUs/mL) in different groups
During root canal preparation, cleaning of the canals and dentinal tubules is achieved through both mechanical and chemical preparation. Use of intra-canal medicaments between sessions is a common approach to reduce bacterial and inflammatory contents of the canals and periapical regions with CH as the most-widely used medicament [20]. For antibacterial effect, CH must break down into calcium and hydroxyl ions which occurs when CH is mixed with an appropriate carrier [20]. CH is effective on most of the bacteria because of its high pH. However, E. faecalis does not respond to CH as it resides in deeper parts of dentinal tubules where pH is stable because of the buffering action of dentin. Moreover, by driving protons to the cytoplasm of bacteria through the action of proton pump [13], cocci can tolerate intracellular pH and show resistance [5]. Disinfection of teeth with tubular infection and long-lasting apical periodontitis can be a challenge that needs specific disinfection procedures in comparison with endodontic treatment of vital teeth [10].
In this context, use of TAP suggested for treatment of open-apex necrotic teeth [13] has come to attention. TAP is an antibiotic powder composed of equal portions of metronidazole, ciprofloxacin, and minocycline which is dissolved in 3 mL of carrier of choice (distilled water or propylene glycol) (33 mg of each antibiotic/mL) [21]. TAP can affect Gram-negative, Gram-positive, and anaerobic bacteria, which are involved in odontogenic infections [14]. In previous studies, TAP was reported to be more effective against E. faecalis than CH [22,23]. Ciprofloxacin, present in TAP, is a synthetic fluoroquinolone with fast bactericidal activity [24]. In the 1980s, fluorination of original quinolone antibiotics yielded fluoroquinolones, with enhanced antibacterial spectrum [25]. In the present ex vivo study, combined use of CH with ciprofloxacin showed the highest antibacterial activity against E. faecalis.
For some clinicians, the probable incidence of allergy may raise an issue of concern with common use of a combination of CH and ciprofloxacin. However, one must know that the incidence of quinolone allergy is lower than beta-lactam allergy and is most likely associated with the expanded use of systemic quinolones and/or introduction of moxifloxacin which appears to be more immunogenic than other quinolones [25]. In the present study, one scoop (1.3 g) of CH powder was mixed with 3 drops (0.15 mL) of 0.3% ciprofloxacin eye drop. This mixture contains 0.00045 g ciprofloxacin which is far beyond the level that could cause allergic reactions. Ciprofloxacin has appropriate tubular penetration, lengthy half-life, and wide-spectrum activity [26]. Ciprofloxacin eye drop is an easily accessible product which can be mixed with CH without diminishing its antimicrobial effect. It must be noted that association of antibiotic with CH did not interfere with the pH of CH paste and increased the antimicrobial action of CH against E. faecalis biofilm formation [5]. As a result, its safe use as a synergistic carrier for CH can be considered as a powerful option in chronic or persistent cases of root canal infection. However, development of resistant strains remains an issue to prohibit common use of this mixture [27,28].
In the present study, the reduction in colony count was significantly greater in CH and betamethasone combination compared with CH and saline although the difference was not significant at 7 and 10 days. This result was consistent with the study carried out by Tabrizizadeh et al. [17], which stated that when betamethasone was used as a carrier for CH, not only the antibacterial efficacy did not alter but it also conferred anti-inflammatory
property to the medicament. Betamethasone does not interfere with antibacterial efficacy of CH because it maintains the alkaline pH of CH [17]. Corticosteroids have anti-inflammatory properties which can reduce pain in apical pathosis followed by infected root canals [29]. Corticosteroids like betamethasone are valuable carriers for CH provided that they do not reduce its antibacterial effects [29]. Moreover, betamethasone has been generally proven as an inhibitor of the growth of many bacterial strains such as Pseudomonadaceae, Enterobacteriaceae, staphylococci, enterococci, streptococci and Staphylococcus aureus, which are susceptible to its action [30]. The most important indications of corticosteroids in endodontics include their topical use on the root surface, systemic administration, or their intracanal application as a medicament is case of root resorption, especially after trauma [31]. As a result, easy combination of one scoop (1.3 g) of CH powder with 3 drops (0.15 mL) of 0.1% betamethasone eye drop can be beneficial specifically in traumatic dental injuries because this mixture contains 0.00015 g betamethasone and showed bactericidal effect more than CH mixed with saline.
Last but not least, in spite of gross reduction in colony count in all experimental groups, no intra-canal medicament was able to eradicate all the bacteria from the root canals. This fact magnifies the role of mechanical instrumentation that can be complemented with different antibacterial chemical strategies.
Conclusion
Betamethasone and ciprofloxacin are appropriate carriers for CH when applied as intracanal medicament. Addition of betamethasone to CH did not interfere with its antimicrobial effectiveness while addition of ciprofloxacin provided stronger antimicrobial effects against E. faecalis biofilm.
Full-Text: (493 Views)
| Abstract
Background and Aim: This study aimed to assess the effect of calcium hydroxide (CH) in combination with betamethasone or ciprofloxacin on Enterococcus faecalis (E. faecalis) biofilm. Materials and Methods: This ex vivo experimental study was conducted on 95 single-rooted human teeth. The root canals were prepared and inoculated with E. faecalis. The samples were incubated for 8 weeks, and biofilm formation was confirmed by observation of 2 samples under a scanning electron microscope (SEM) and culture in 3 samples. The remaining samples were divided into three groups (n=30): CH + etamethasone eye drop, CH + ciprofloxacin eye drop, and CH + saline. Microbial analysis was performed at 1, 7 and 10 days. The colony count was measured. Comparisons were made by two-way ANOVA and a post-hoc test using SPSS. Results: On day 1, the highest colony count was observed in CH + saline group. The difference in colony count between CH + ciprofloxacin and CH + betamethasone, and the difference between CH + betamethasone and CH + saline were not significant at days 7 and 10. CH + ciprofloxacin showed significantly lower colony count than CH + saline at 1 (P=0.001), 7 (P=0.004) and 10 (P=0.002) days. Conclusion: The result of this study showed that betamethasone and ciprofloxacin were appropriate carriers for CH and resulted in suitable antibacterial effects against E. faecalis. Key Words: Betamethasone; Biofilms; Calcium Hydroxide; Ciprofloxacin; Enterococcus faecalis |
Introduction
Elimination of root canal bacteria is a perquisite for a successful root canal treatment. To achieve this goal, a combination of mechanical and chemical irrigation is necessary [1]. However, not all bacteria are eliminated through chemomechanical preparation, and some species can survive in inaccessible areas of the canal such as delta, isthmi and dentinal tubules [2]. Application of inter-appointment canal medicaments may help to decrease these persistent bacteria [3].
Evidence shows that bacterial elimination may be achieved by the application of calcium hydroxide (CH) as an intra-canal medicament [1]. First suggested by Hermann in 1920, CH is the most commonly used medicament due to its denaturizing effects on proteins as well as its antimicrobial qualities that are believed to be due to its very high pH resulting from the dissociation of hydroxyl ions. Water must be present for the antimicrobial effect of CH [4]. The dissociation of CH particles allows the diffusion of hydroxyl and calcium ions through the dentinal tubules [5]. The high pH promotes microbial inhibition through an irreversible enzymatic reaction [6]. Not only does calcium act by clearing the carbon dioxide used by bacteria for anaerobic respiration [7], but also it has the ability to promote inactivation of bacterial lipopolysaccharides found in the outer membrane of Gram-negative bacteria [8]. The mechanism of action for this phenomenon is the increase in pH, which might stimulate genetic cascades that modify the characteristics of the bacterial cells [5]. However, the effects of CH are limited in persistent infections [9].
Enterococcus faecalis (E. faecalis), is a facultative anaerobic Gram-positive coccus and is the most commonly isolated species from teeth with persistent periapical lesions (predominantly in endodontic failures) [10]. However, more recent studies believe that CH is unable to kill E. faecalis [11]. Evidence shows that E. faecalis may benefit from a CH challenge and grow in mixed biofilms [12]. It has been demonstrated that, when exposed to calcium hydroxide, E. faecalis uses a proton pump which can drive protons to the cytoplasm of the bacterium [13] to control intracellular pH and confer resistance [5].
For this reason, combination of CH with antibiotics has been proposed to improve the action against this microorganism [5]. The use of triple (TAP) and double antibiotic paste (DAP) (a combination of metronidazole and ciprofloxacin with/without minocycline) during endodontic regeneration is an accepted and essential step [14]. Ciprofloxacin is classified as a second-generation fluoroquinolone and is effective against enteric bacteria such as Enterococcus species with high tubular penetration [15]. According to de Freitas et al, [5] the highest pH values were found for CH paste containing ciprofloxacin.
Another goal in root canal treatment is to reduce inflammation and post-treatment pain. Local steroids, systemic steroids and non-steroidal anti-inflammatory drugs were introduced to achieve this purpose [16]. It has been stated that local steroids like betamethasone do not change antibacterial effectiveness of CH against planktonic E. faecalis but there is no information about E. faecalis biofilm [17]. Conversely, some have reported the combination of CH with hydrocortisone being non effective against E. faecalis [18]. Also, it has been shown that antibacterial effectiveness of CH on E. faecalis improves in combination with non-steroidal anti-inflammatory drugs [5]. Considering the conflicting data, this study was designed to assess the antibacterial efficacy of CH alone and in combination with betamethasone and ciprofloxacin on intracanal 8-week biofilm of E. faecalis.
Materials and Methods
After approval by the ethics committee of the Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran (IR.IAU.DENTAL.REC.1398.064), this ex vivo study was conducted on 95 single-rooted extracted human teeth with mature apices. The teeth included in this study were extracted due to periodontal attachment loss, orthodontic purposes, or unrestorable crown. After surface cleaning and disinfection, the teeth were examined under a laboratory microscope (Stemi DV4 Spot; Carl Zeiss, Oberkochen, Germany) at ×20 magnification to exclude teeth with cracks, caries, or restoration. Digital radiographs were obtained from buccal and proximal directions for detection of any anatomical complexity, internal resorption, and calcification. Selected teeth had root curvatures not greater than 20 degrees according to the Schneider’s method [19].
The whole procedure included root canal preparation and sterilization, bacterial inoculation, incubation for biofilm formation for 8 weeks, preparation and application of intra-canal medicaments, and culturing and microbial analysis by means of counting the number of colony-forming units (CFUs).
Canal preparation:
The crowns were cut to prepare root lengths of 12 mm from cervical to apical. Canals from orifice to apex were prepared with # 1 to #3 Gates Glidden drills (Dentsply-Maillefer, Ballaigues, Switzerland). Afterwards, for smear layer removal, the canals were irrigated with 5 mL of 17% EDTA solution (Darupakhsh, Tehran, Iran) followed by 5 mL of 0.9% saline (Darupakhsh, Tehran, Iran) and then 5 mL of 5.25% NaOCl (Darupakhsh, Tehran, Iran). Teeth were autoclaved for 30 minutes and were incubated at 37ºC for 48 hours. Sterilization was repeated if any opacity was detected in brain heart infusion broth [1,2].
Biofilm formation:
Fresh suspension of E. faecalis (ATCC 29212) was obtained from the Biological Resource Center (Tehran, Iran) and incubated in fresh brain heart infusion broth (Merck, Darmstadt, Germany) in aerobic atmosphere at 37°C for 4-5 hours, until the optical density of 600 nm was adjusted to a concentration of 1.0×106 CFUs per milliliter (CFUs/mL), and was verified spectrophotometric ally (OD600: 0.01–0.02). This suspension was inoculated into the canals by a 30-gauge needle. The samples were incubated at 37ºC for 8 weeks while placed on a shaker operating at 150 rpm [1].
Biofilm control:
By the end of 8 weeks, two samples were randomly removed from the incubator, fixed and observed under a scanning electron microscope (SEM; Jeol-JSM 5600LV, Noran Instruments, Tokyo, Japan) at 15 kW, to confirm biofilm formation (Figures 1 and 2). Also, three samples were randomly selected to determine the number of pre-intervention CFUs. In order to determine the colony count, the biofilm was ultrasonically disrupted and transferred to phosphate buffer saline (Dulbecco's Modified Formula; ICN Biochemicals, England). After dilution, culture was prepared on agar medium, and incubated at 37ºC for 96 hours to count the primary number of CFUs [1].
Figure 1. SEM micrograph of the first sample confirming the formation of eight-week biofilm on root canal wall at different magnifications: (A) 50 µm, (B) 10 µm, (C) 5 µm and (D) 2 µm
{kind=link}
Figure 2. SEM micrograph of the second sample confirming the formation of eight-week biofilm on root canal wall at different magnifications: (A) 50 µm, (B) 10 µm, (C) 5 µm and (D) 2 µm
{kind=link}
Preparation and application of intracanal medicaments:
The samples were randomly divided into three groups:
Group 1 (CH + betamethasone) (n=30): one scoop (equal to 1.3 g) of CH powder (Pishro Dandan Co., Tehran, Iran) was mixed with 0.15 mL (3 drops) of 0.1% betamethasone eye drop (Abooreihan Co., Tehran, Iran). This mixture contained 0.00015 g betamethasone.
Group 2 (CH + ciprofloxacin) (n=30): one scoop (equal to 1.3 g) of CH powder (Pishro Dandan Co., Tehran, Iran) was mixed with 0.15 mL (3 drops) of 0.3% ciprofloxacin eye drop (Abooreihan Co., Tehran, Iran). This mixture contained 0.00045 g ciprofloxacin.
Group 3 (CH + saline) (n=30): one scoop (equal to 1.3 g) of CH powder (Pishro Dandan Co., Tehran, Iran) was mixed with 0.15 mL (3 drops) of saline.
The mixtures were delivered into the canals by means of a #30 lentulo spiral (Mani, Tochigi, Japan) [13].
Microbial analysis:
Microbial analysis and colony counting were performed at 1, 7 and 10 days. At each time point, 10 samples were selected from each group, and biofilm was disrupted by ultrasonication, and transferred to 0.9 mL of phosphate buffered saline (Dulbecco's Modified Formula; ICN Biochemicals, England). After dilution, the samples were spread on agar plate and incubated at 37ºC for 96 hours. After culture, the colony count was measured for the purpose of comparison with the primary colony count [13].
Statistical analysis:
The Kolmogorov-Smirnov test was conducted to assess the normality of data distribution. Accordingly, the comparison among the groups was performed by two-way ANOVA and a post-hoc test using SPSS version 20 (IBM SPSS Inc., Chicago, IL].
Results
At 1 day, the highest colony count was observed in CH + betamethasone group followed by CH + saline, and the difference between them was highly significant (P<0.001). The difference between CH + betamethasone and CH + saline, and also the difference between CH + betamethasone and CH + ciprofloxacin was also significant in colony count (P=0.043).
At 7 and 10 days, the highest colony count was observed in CH + saline samples. While the difference between CH + ciprofloxacin and CH + betamethasone samples (P=0.67 at 7 days and P=0.272 at 10 days), and the difference between CH + betamethasone and CH + saline were not significant (P=0.13 at 7 days and P=0.272 at 10 days).
CH + ciprofloxacin group showed significantly lower colony count than CH + saline at 1 (P=0.001), 7 (P=0.004) and 10 (P=0.002) days (Tables 1 and 2; Figure 3).
Discussion
The present study evaluated the antibacterial effect of CH in combination with saline, betamethasone or ciprofloxacin on 8-week biofilm of E. faecalis in root canals of extracted human teeth. The results showed the lowest and the highest colony count in CH + ciprofloxacin and CH + saline groups, respectively. The combination of CH +betamethasone also showed some antibacterial activity. The alternative hypothesis behind the primary research question was confirmed: through colony counting, it was shown that combination of CH with ciprofloxacin or betamethasone improved the ex vivo antibacterial effects of CH paste on eight-week biofilm of E. faecalis.
When a carious lesion extends to the pulp chamber and the hard tissue barrier is breached, bacteria can invade the pulp tissue. In apical periodontitis, bacteria invade further and colonize the entire root canal system. Accordingly, to promote healing of apical periodontitis and cleaning of the root canal system, microorganisms within the root canal system must be eliminated.
Table 1. Mean colony count in the three groups at 1, 7 and 10 days
{kind=link}
Table 2. Pairwise comparisons of the antibacterial effects of different medicaments
{kind=link}
Figure 3. Colony count (CFUs/mL) in different groups
{kind=link}
During root canal preparation, cleaning of the canals and dentinal tubules is achieved through both mechanical and chemical preparation. Use of intra-canal medicaments between sessions is a common approach to reduce bacterial and inflammatory contents of the canals and periapical regions with CH as the most-widely used medicament [20]. For antibacterial effect, CH must break down into calcium and hydroxyl ions which occurs when CH is mixed with an appropriate carrier [20]. CH is effective on most of the bacteria because of its high pH. However, E. faecalis does not respond to CH as it resides in deeper parts of dentinal tubules where pH is stable because of the buffering action of dentin. Moreover, by driving protons to the cytoplasm of bacteria through the action of proton pump [13], cocci can tolerate intracellular pH and show resistance [5]. Disinfection of teeth with tubular infection and long-lasting apical periodontitis can be a challenge that needs specific disinfection procedures in comparison with endodontic treatment of vital teeth [10].
In this context, use of TAP suggested for treatment of open-apex necrotic teeth [13] has come to attention. TAP is an antibiotic powder composed of equal portions of metronidazole, ciprofloxacin, and minocycline which is dissolved in 3 mL of carrier of choice (distilled water or propylene glycol) (33 mg of each antibiotic/mL) [21]. TAP can affect Gram-negative, Gram-positive, and anaerobic bacteria, which are involved in odontogenic infections [14]. In previous studies, TAP was reported to be more effective against E. faecalis than CH [22,23]. Ciprofloxacin, present in TAP, is a synthetic fluoroquinolone with fast bactericidal activity [24]. In the 1980s, fluorination of original quinolone antibiotics yielded fluoroquinolones, with enhanced antibacterial spectrum [25]. In the present ex vivo study, combined use of CH with ciprofloxacin showed the highest antibacterial activity against E. faecalis.
For some clinicians, the probable incidence of allergy may raise an issue of concern with common use of a combination of CH and ciprofloxacin. However, one must know that the incidence of quinolone allergy is lower than beta-lactam allergy and is most likely associated with the expanded use of systemic quinolones and/or introduction of moxifloxacin which appears to be more immunogenic than other quinolones [25]. In the present study, one scoop (1.3 g) of CH powder was mixed with 3 drops (0.15 mL) of 0.3% ciprofloxacin eye drop. This mixture contains 0.00045 g ciprofloxacin which is far beyond the level that could cause allergic reactions. Ciprofloxacin has appropriate tubular penetration, lengthy half-life, and wide-spectrum activity [26]. Ciprofloxacin eye drop is an easily accessible product which can be mixed with CH without diminishing its antimicrobial effect. It must be noted that association of antibiotic with CH did not interfere with the pH of CH paste and increased the antimicrobial action of CH against E. faecalis biofilm formation [5]. As a result, its safe use as a synergistic carrier for CH can be considered as a powerful option in chronic or persistent cases of root canal infection. However, development of resistant strains remains an issue to prohibit common use of this mixture [27,28].
In the present study, the reduction in colony count was significantly greater in CH and betamethasone combination compared with CH and saline although the difference was not significant at 7 and 10 days. This result was consistent with the study carried out by Tabrizizadeh et al. [17], which stated that when betamethasone was used as a carrier for CH, not only the antibacterial efficacy did not alter but it also conferred anti-inflammatory
property to the medicament. Betamethasone does not interfere with antibacterial efficacy of CH because it maintains the alkaline pH of CH [17]. Corticosteroids have anti-inflammatory properties which can reduce pain in apical pathosis followed by infected root canals [29]. Corticosteroids like betamethasone are valuable carriers for CH provided that they do not reduce its antibacterial effects [29]. Moreover, betamethasone has been generally proven as an inhibitor of the growth of many bacterial strains such as Pseudomonadaceae, Enterobacteriaceae, staphylococci, enterococci, streptococci and Staphylococcus aureus, which are susceptible to its action [30]. The most important indications of corticosteroids in endodontics include their topical use on the root surface, systemic administration, or their intracanal application as a medicament is case of root resorption, especially after trauma [31]. As a result, easy combination of one scoop (1.3 g) of CH powder with 3 drops (0.15 mL) of 0.1% betamethasone eye drop can be beneficial specifically in traumatic dental injuries because this mixture contains 0.00015 g betamethasone and showed bactericidal effect more than CH mixed with saline.
Last but not least, in spite of gross reduction in colony count in all experimental groups, no intra-canal medicament was able to eradicate all the bacteria from the root canals. This fact magnifies the role of mechanical instrumentation that can be complemented with different antibacterial chemical strategies.
Conclusion
Betamethasone and ciprofloxacin are appropriate carriers for CH when applied as intracanal medicament. Addition of betamethasone to CH did not interfere with its antimicrobial effectiveness while addition of ciprofloxacin provided stronger antimicrobial effects against E. faecalis biofilm.
Type of Study: Original article |
Subject:
Endodontics
References
1. McGurkin-Smith R, Trope M, Caplan D, Sigurdsson A. Reduction of intracanal bacteria using GT rotary instrumentation, 5.25% NaOCl, EDTA, and Ca(OH)2. J Endod. 2005 May;31(5):359-63. [DOI:10.1097/01.don.0000145035.85272.7c] [PMID]
2. Peters LB, van Winkelhoff AJ, Buijs JF, Wesselink PR. Effects of instrumentation, irrigation and dressing with calcium hydroxide on infection in pulpless teeth with periapical bone lesions. Int Endod J. 2002 Jan;35(1):13-21. [DOI:10.1046/j.0143-2885.2001.00447.x] [PMID]
3. Ahangari Z, Mojtahed Bidabadi M, Asnaashari M, Rahmati A, Tabatabaei FS. Comparison of the Antimicrobial Efficacy of Cal-cium Hydroxide and Photodynamic Therapy Against Entero-coccus faecalis and Candida albicans in Teeth With Periapical Lesions; An In Vivo Study. J Lasers Med Sci. 2017 Spring;8(2):72-78. [DOI:10.15171/jlms.2017.13] [PMID] [PMCID]
4. Safavi K, Nakayama TA. Influence of mixing vehicle on dissoci-ation of calcium hydroxide in solution. J Endod. 2000 Nov;26(11):649-51. [DOI:10.1097/00004770-200011000-00004] [PMID]
5. de Freitas RP, Greatti VR, Alcalde MP, Cavenago BC, Vivan RR, Duarte MA, Weckwerth AC, Weckwerth PH. Effect of the Associ-ation of Nonsteroidal Anti-inflammatory and Antibiotic Drugs on Antibiofilm Activity and pH of Calcium Hy-droxide Pastes. J Endod. 2017 Jan;43(1):131-4. [DOI:10.1016/j.joen.2016.09.014] [PMID]
6. Siqueira JF Jr, Lopes HP. Mechanisms of antimicrobial activity of calcium hydroxide: a critical review. Int Endod J. 1999 Sep;32(5):361-9. [DOI:10.1046/j.1365-2591.1999.00275.x] [PMID]
7. Kontakiotis E, Nakou M, Georgopoulou M. In vitro study of the indirect action of calcium hydroxide on the anaerobic flora of the root canal. Int Endod J. 1995 Nov;28(6):285-9. [DOI:10.1111/j.1365-2591.1995.tb00317.x] [PMID]
8. Tanomaru JM, Leonardo MR, Tanomaru Filho M, Bonetti Filho I, Silva LA. Effect of different irrigation solutions and calcium hydroxide on bacterial LPS. Int Endod J. 2003 Nov; 36(11):733-9. [DOI:10.1046/j.1365-2591.2003.00717.x] [PMID]
9. Sathorn C, Parashos P, Messer H. Antibacterial efficacy of cal-cium hydroxide intracanal dressing: a systematic review and meta-analysis. Int Endod J. 2007 Jan;40(1):2-10. [DOI:10.1111/j.1365-2591.2006.01197.x] [PMID]
10. Orstavik D. Root canal disinfection: a review of concepts and recent developments. Aust Endod J. 2003 Aug;29(2):70-4. [DOI:10.1111/j.1747-4477.2003.tb00515.x] [PMID]
11. Javidi M, Afkhami F, Zarei M, Ghazvini K, Rajabi O. Efficacy of a combined nanoparticulate/calcium hydroxide root canal medication on elimination of Enterococcus faecalis. Aust Endod J. 2014 Aug;40(2):61-5. [DOI:10.1111/aej.12028] [PMID]
12. van der Waal SV, Connert T, Crielaard W, de Soet JJ. In mixed biofilms Enterococcus faecalis benefits from a calcium hydrox-ide challenge and culturing. Int Endod J. 2016 Sep; 49 (9):865-73. [DOI:10.1111/iej.12542] [PMID]
13. Mehta S, Verma P, Tikku AP, Chandra A, Bains R, Banerjee G. Comparative evaluation of antimicrobial efficacy of triple anti-biotic paste, calcium hydroxide, and a proton pump inhibitor against resistant root canal pathogens. Eur J Dent. 2017 Jan-Mar;11(1):53-7. [DOI:10.4103/ejd.ejd_159_16] [PMID] [PMCID]
14. Nosrat A, Seifi A, Asgary S. Regenerative endodontic treat-ment (revascularization) for necrotic immature permanent molars: a review and report of two cases with a new biomaterial. J Endod. 2011 Apr;37(4):562-7. [DOI:10.1016/j.joen.2011.01.011] [PMID]
15. Sisto F, Bonomi A, Cavicchini L, Coccè V, Scaltrito MM, Bondiolotti G, Alessandri G, Parati E, Pes-sina A. Human mesenchymal stromal cells can uptake and release ciprofloxacin, acquiring in vitro anti-bacterial activity. Cytotherapy. 2014 Feb;16(2):181-90. [DOI:10.1016/j.jcyt.2013.11.009] [PMID]
16. Davoudi A, Razavi SA, Mosaddeghmehrjardi MH, Tabrizizadeh M. The Effect of Fragaria vesca Extract on Smear Layer Removal: A Scanning Electron Microscopic Evaluation. Iran Endod J. 2015 Summer;10(3):204-7.
17. Tabrizizadeh M, Rasti M, Ayatollahi F, Mossadegh MH, Zandi H, Dehghan F, Mousavi Z. Antimicrobial Activity of Calcium Hy-droxide and Betamethasone on Enterococcus faecalis; An in vitro Assessment. Iran Endod J. 2015 Summer;10(3):184-7.
18. SENA IADA, ARAÚJO IJDS, SANTOS MMD, LIMA IPC. Antibacterial effectiveness in vitro of different formulations of calcium hydroxide paste. RGO-Revista Gaúcha de Odontologia. 2017;65(4):293-8. [DOI:10.1590/1981-863720170002000013127]
19. Schneider SW. A comparison of canal preparations instraight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32:271-5. [DOI:10.1016/0030-4220(71)90230-1] [PMID]
20. Mohammadi Z, Dummer PM. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J. 2011 Aug;44(8):697-730. [DOI:10.1111/j.1365-2591.2011.01886.x] [PMID]
21. Sabrah AH, Yassen GH, Gregory RL. Effectiveness of antibiotic medicaments against biofilm formation of Enterococcus faecalis and Porphyromonas gingivalis. J Endod. 2013;39(11):1385-9. [DOI:10.1016/j.joen.2013.05.003] [PMID]
22. Adl A, Shojaee NS, Motamedifar M. A Comparison between the Antimicrobial Effects of Triple Antibiotic Paste and Calcium Hydroxide Against Entrococcus Faecalis. Iran Endod J. 2012 Summer;7(3):149-55.
23. Karataş E, Baltacı MÖ, Uluköylü E, Adıgüzel A. Antibacterial effectiveness of calcium hydroxide alone or in combination with Ibuprofen and Ciprofloxacin in teeth with asymptomatic apical periodontitis: a randomized controlled clinical study. Int Endod J. 2020 Jun;53(6):742-53. [DOI:10.1111/iej.13277] [PMID]
24. Diwan A, Bhagavaldas MC, Bagga V, Shetty A. Multidisciplinary Approach in Management of a Large Cystic Lesion in Anterior Maxilla - A Case Report. J Clin Diagn Res. 2015 May;9(5):ZD41-3. [DOI:10.7860/JCDR/2015/13540.5992] [PMID] [PMCID]
25. McGee EU, Samuel E, Boronea B, Dillard N, Milby MN, Lewis SJ. Quinolone Allergy. Pharmacy (Basel). 2019 Jul 19; 7(3):97. [DOI:10.3390/pharmacy7030097] [PMID] [PMCID]
26. Somasundaram S, Manivannan K. An Overview of Fluoroquinolones. ARRB [Internet]. 10May2013 ;3(3):296-313.
27. Kim YB, Seo KW, Shim JB, Son SH, Noh EB, Lee YJ. Molecular characterization of antimicrobial-resistant Enterococcus faecalis and Enterococcus faecium isolated from layer parent stock. Poult Sci. 2019 Nov 1;98(11):5892-9. [DOI:10.3382/ps/pez288] [PMID]
28. Sun Y, Lu H, Zhang X, Wu Q, Bi W, Liu H, Cao J, Zhou T. Pheno-type and genotype alteration during adaptive evolution of Enterococcus faecalis to antimicrobials. Infect Genet Evol. 2018 Aug;62:80-5. [DOI:10.1016/j.meegid.2018.03.029] [PMID]
29. Mohammadi Z. Systemic and local applications of steroids in endodontics: an update review. Int Dent J. 2009 Oct; 59(5):297-304.
30. Artini M, Papa R, Cellini A, Tilotta M, Barbato G, Koverech A, Selan L. Effect of betamethasone in combination with antibiotics on gram positive and gram negative bacteria. Int J Immunopathol Pharmacol. 2014 Oct-Dec;27(4):675-82. [DOI:10.1177/039463201402700426] [PMID]
31. Abbott PV. Prevention and management of external inflammatory resorption following trauma to teeth. Aust Dent J. 2016 Mar;61 Suppl 1:82-94. [DOI:10.1111/adj.12400] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
