Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 236-242 |
Back to browse issues page


Ethics code: IR.IAU.KHUISF.REC.1398.121
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Golestaneh G, Rafiei M, Golestaneh A. Maximum Bite Force of Skeletal Class II Pa-tients Between 18-30 Years Before and After
Orthognathic Surgery. J Res Dent Maxillofac Sci 2023; 8 (4) :236-242
URL: http://jrdms.dentaliau.ac.ir/article-1-462-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-462-en.html



1- Department of Endodontics, School of Dentistry, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
2- Department of Orthodontics, Faculty of Dentistry, Islamic Azad University, Isfahan (Khorasgan) Branch, Isfahan, Iran ,mehdi.rafiei@khuisf.ac.ir
3- Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Islamic Azad University, Isfahan (Khorasgan) Branch, Isfahan, Iran
2- Department of Orthodontics, Faculty of Dentistry, Islamic Azad University, Isfahan (Khorasgan) Branch, Isfahan, Iran ,
3- Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Islamic Azad University, Isfahan (Khorasgan) Branch, Isfahan, Iran
Full-Text [PDF 640 kb]
(1042 Downloads)
| Abstract (HTML) (2914 Views)
Introduction
Mastication is a complex function that involves a number of factors such as the position of the posterior teeth and the bite force [1]. After completion of permanent dentition and hormonal stability, the maximum bite force decreases and is stabilized. The masticatory forces indicate the function of the muscles of mastication and their interactions. Thus, measurement of the bite force can provide beneficial information regarding the activity and function of the muscles and dentition. The maximum bite force depends on anthropometric characteristics such as age and gender of patients [2]. The bite force is a reflection of the lever system of the mandible. In long-face individuals, the maxilla has a downward rotation. Thus, the mechanical properties of the elevator muscles decrease and; therefore, the bite force in long-face patients is lower than that in normal-face individuals. Periodontal status also influences the bite force [3].
In case of presence of compensatory movement of the teeth due to skeletal deformity, the position of the teeth should be orthodontically corrected prior to surgery, and irrespective of the relationship with the opposing arch. This procedure worsens the deformity prior to surgery; however, it is necessary in order to correct positioning of the osteotomized segments by surgery. The type of presurgical orthodontic treatment varies in different individuals.
Patients with skeletal Class II malocclusion may have mandibular deficiency, maxillary excess or a combination of both. Bilateral sagittal split osteotomy (BSSO) is the most commonly performed procedure for mandibular advancement, which is easily performed through an intraoral incision [4].
It appears that the mandible serves as a lever based on two assumptions: (I) The interaction of force vectors generated by the muscles of mastication passes through the bite point. (II) Also, the condylar neck and/or the temporomandibular joint (TMJ) are not suitable to tolerate the reaction force during mastication. Assessment of the electromyographic data and the properties of the TMJ support the mandibular lever theory. Moreover, analysis of the strength of the condylar neck indicates that this structure is strong enough to tolerate the expected reaction force during the lever function [5]. According to Proffit [6], the masticatory system is a classic lever, and the muscles are located between the support, which is the TMJ, and the point of load application i.e., between the teeth.
Considering all the above, orthognathic surgery, and particularly BSSO in Class II patients with mandibular deficiency and normal facial vertical height is expected to change their bite force; however, the efficacy of orthognathic surgery in improvement of the masticatory function is a matter of discussion.
The maximum bite force is measured to assess the effect of different dental procedures on the masticatory system such as orthodontic and prosthodontic treatments. Also, the effects of facial deformities such as malocclusion and TMJ disorders on the bite force have been previously studied [7]. However, to the best of the authors’ knowledge, no study has precisely addressed the changes in bite force after orthognathic surgery in skeletal Class II patients. Thus, considering the significance of the masticatory function and its effects on health, and the bite force as an objective and quantitative parameter for assessment of the efficiency of mastication [2], this study aimed to assess the changes in maximum bite force in skeletal Class II patients between 18-30 years after orthognathic surgery compared with the preoperative state.
The main objective of this study was to assess the maximum bite force in skeletal Class II patients with mandibular deficiency between 18-30 years before and after mandibular advancement surgery. The maximum bite force was the primary outcome. Correlations of the maximum bite force of patients before surgery with their overbite and overjet, and side of the jaw were considered as the secondary outcomes of the study.
Materials and Methods
This inception cohort study (ethical code: IR.IAU.KHUISF.REC.1398.121) was conducted on 17 skeletal Class II malocclusion patients who required mandibular advancement and presented to the Oral and Maxillofacial Surgery Department of Islamic Azad University, School of Dentistry, Khorasgan Branch.
The participants had skeletal Class II malocclusion with mandibular deficiency and no problem in vertical dimension of the face (normal face). They were between 18 to 30 years, required mandibular advancement by BSSO, and had no developmental syndromes, no cleft lip and palate, no history of jaw trauma, no TMJ problem, good general health, and optimal cooperation. All patients had received a course of orthodontic treatment for decompensation. Orthodontic treatment of patients had been scheduled to continue for at least 6 months after surgery.
The patients had no neuromuscular or neurological disorders, sensitive or mobile first molars, first molars with extensive restorations, prosthetic crowns, or bruxism or clenching.
After obtaining written informed consent from the patients, their bite force was measured preoperatively and at 6 weeks, and 3 and 6 months, postoperatively. The device used for this purpose had a load cell with a maximum capacity of 100 kg, and a digital display. This device was designed by Mahsa Rismanchian, an engineer with a Master's degree in computer science from the Islamic Azad University, Khorasgan branch) (Figure 1).
Figure 1. Bite force measuring device
The sensor covered in disposable pads was first placed on the mandibular right first molar and then on the mandibular left first molar. The patients were then requested to bite on the sensor with maximum power for 5 seconds. This was repeated for each side of the jaw four times, with 5-minute resting intervals. At each time of measurement, the maximum force displayed on the monitor was recorded.
Eventually, the maximum value among all four measurements was recorded for the respective side of the jaw. The patients’ head was in natural head position for measurement of the bite force. For this purpose, the patients were in the upright position and asked to look straight ahead such that the Frankfurt plane was almost parallel to the ground. The overbite and overjet were also measured on diagnostic casts and recorded.
Sample size calculation:
The sample size was calculated to be 17 by repeated measures ANOVA using G*Power software assuming α=0.05, β=0.2, study power of 80%, mean effect size (d) of 0.3, and 4 repetitions. Considering 10% possibility of loss to follow-up, 20 patients were enrolled.
Statistical analysis:
Data were analyzed using descriptive and inferential statistics. Repeated measures ANOVA with the two repeated measures of time of measurement and side of the jaw was applied for data analysis. The normality of data distribution was evaluated by the Shapiro-Wilk test, and the Mauchly’s test was applied to test the assumption of sphericity. Data were found to be normally distributed. However, the Mauchly’s test showed that the effects of time and the interaction effect of time and side of the jaw were significant on bite force. Thus, the Greenhouse-Geisser test was applied for data analysis. The Spearman and the Pearson’s correlation coefficients were used to analyze the correlation of maximum bite force with overbite and overjet of patients. All statistical analyses were carried out by SPSS version 22 at 0.05 level of significance.
Results
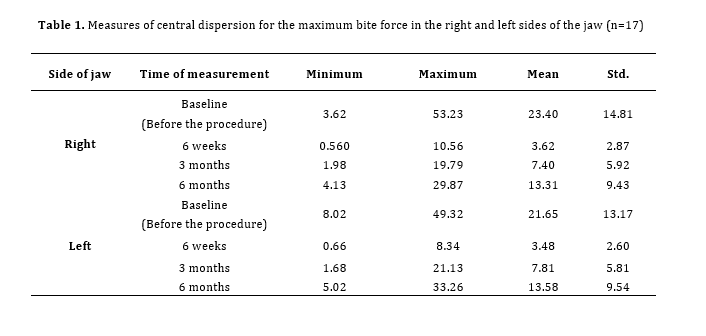
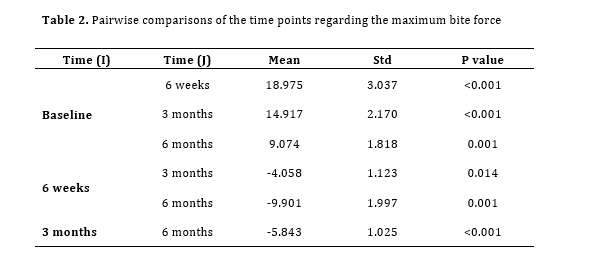
Seventeen patients were evaluated including 13 women and 4 men between 18-30 years. Table 1 presents the measures of central dispersion for the maximum bite force in the right and left sides of the jaw. Repeated measures ANOVA showed that the effect of time of measurement on maximum bite force was significant (P<0.001). In other words, the mean maximum bite force of patients was significantly different at different time points. The effect of side of the jaw on maximum bite force was not significant (P=0.589). In other words, the maximum bite force was not significantly different in the right and left sides of the jaw. The interaction effect of time and laterality on bite force was not significant either (P=0.294). The Bonferroni adjustment was then applied for pairwise comparisons of the time points regarding the maximum bite force (Table 2). As shown, the mean maximum bite force at baseline was significantly higher than that at 6 weeks (P<0.001), 3 months (P<0.001) and 6 months (P<0.001). The mean maximum bite force at 6 weeks was also significantly lower than that at 3 months (P=0.014) and 6 months (P=0.001). The mean maximum bite force at 3 months was significantly lower than that at 6 months (P<0.001).
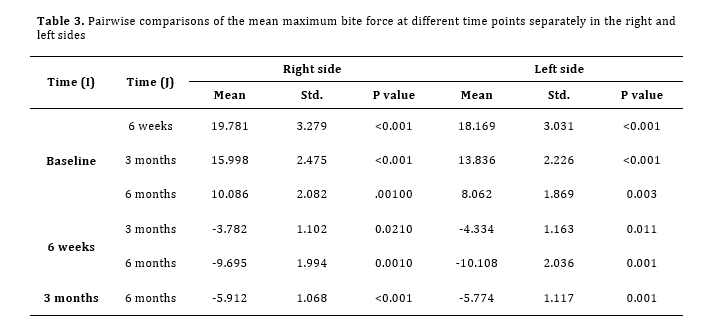
Pairwise comparisons of the mean maximum bite force at different time points separately in the right and left sides (Table 3) indicated that in the right side, the mean maximum bite force of patients preoperatively was significantly higher than that at 6 weeks (P<0.001), 3 months (P<0.001) and 6 months (P<0.001), postoperatively. The value at 6 weeks was significantly lower than that at 3 months (P=0.021) and 6 months (P<0.001). The value at 3 months was also significantly lower than that at 6 months (P<0.001). The same results were obtained in the left side.
Before the procedure, the mean overbite was 2.26±0.40 mm (range 2-3 mm), and the mean overjet was 9.52±1.03 mm (range 8-12 mm). The Spearman’s correlation test revealed no significant correlation between overbite and the maximum bite force in the right (P=0.181) or left (P=0.134) side. The Pearson’s correlation test found no significant correlation between the overjet and the maximum bite force in the right (P=0.881)
or left (P=0.677) side of the jaw. After surgery, the patients reached the normal range of overbite (1-2 mm) and the normal range of overjet (2-3 mm).
Table 1. Measures of central dispersion for the maximum bite force in the right and left sides of the jaw (n=17)
Table 2. Pairwise comparisons of the time points regarding the maximum bite force
Table 3. Pairwise comparisons of the mean maximum bite force at different time points separately in the right and left sides
Discussion
This study assessed the changes in maximum bite force of skeletal Class II patients between 18-30 years after orthognathic surgery compared with the preoperative state. The results indicated that the mean maximum bite force at 6 weeks after the procedure was significantly lower than that before the procedure. The maximum bite force significantly increased at 3 and 6 months but was still lower than the baseline preoperative value. This trend suggests that the bite force may eventually return to the baseline value in longer eriods of time, which calls for studies with longer follow-ups. Reduction in bite force after orthognathic surgery in the present study can be attributed to postoperative edema, inflammation and pain. Also, patients have a soft diet for at least 1 month after orthognathic surgery, which also weakens the muscles of mastication. This explains the lowest bite force at 6 weeks, postoperatively. Physiotherapy and exercise improved the muscle function and increased the bite force at 3 and then at 6 months.
Also, the patients may have fear of biting hard on the sensor after surgery, which may also explain the reduction in bite force. Furthermore, after mandibular advancement, the distance between the teeth (site of load application) and muscles increases; thus, the maximum bite force is also expected to decrease. However, since the magnitude of mandibular advancement is small (relative to the jaw length), the change in bite force is also small. Increased maximum bite force after orthognathic surgery in some studies may be due to the use of screw and plate for jaw fixation and its psychological effect on patients, which would give them the courage to bite harder on the sensor. Also, correction of Class II relationship improves the contact of tooth surfaces in centric occlusion, and subsequently increases the efficiency of mastication and the maximum bite force [8].
Celakil et al. [6] evaluated the effect of orthognathic surgery on muscle function of skeletal Class III patients. They evaluated electromyographic activity before and after splinting and at 1 and 6-8 months after orthognathic surgery. The present study was conducted on Class II patients who needed mandibular advancement. Despite the different methods, their results were consistent with ours and showed a decrease in bite force after orthognathic surgery. Firoozeie et al. [9] evaluated the changes in bite force and electromyographic activity of the muscles of mastication in patients with mandibular prognathism following orthognathic surgery. They reported that at 3 months postoperatively, the bite force and the electromyographic activity of the masticatory muscles of patients were lower than the corresponding values before surgery. All parameters improved at 6 months after surgery but the maximum bite force at the molar site did not reach the preoperative state. The same results were obtained in the present study regarding the reduction in bite force by up to 6 months. Islam et al. [10] systematically evaluated the changes in bite force after orthognathic surgery for correction of mandibular prognathism. They reviewed 17 articles and a total of 697 patients between 15-44 years. A total of 532 patients underwent BSSO, 108 underwent intraoral vertical ramus osteotomy and 24 underwent extraoral vertical ramus osteotomy. They concluded that the efficiency of mastication at 3 months after surgery was higher than that before surgery, and this improvement was significant after 6 months. Also, the occlusal contact points and surfaces increased after 3 months; this increase was significant after 12 months. The occlusal forces improved as well. However, the values in corrected prognathic patients were still lower than the corresponding values in normognathic patients 2 years after surgery. Similarly, the present study showed that the maximum bite force at 6 months after surgery was still lower than the baseline value. In the present study, in contrast to the findings of Islam et al. [10], the efficacy of mastication at 3 and 6 months after surgery was lower than that before the procedure. The occlusal contact points and surfaces improved at 3 and 6 months postoperatively in the present study, due to the conversion of Class II to Class I occlusion, which was in agreement with the results of Islam et al, [10].
However, it should be noted that Islam et al. [10] evaluated Class III patients while the present study was conducted on Class II patients.
Yari et al. [8], conducted a study that compared the maximum bite force in skeletal Class III patients before and after orthognathic surgery. They examined the maximum bite force before surgery and 3 months after surgery. Their results were consistent with ours, and the patients showed a decrease in bite force 3 months after surgery. Naguib et al. [11] investigated the changes in masticatory muscles following orthognathic surgery (BSSO for correction of skeletal Class III deformity). In contrast to our study, no changes in temporalis and masseter muscle contraction strength were observed after BSSO as determined by EMG examination. Hu et al. [12] evaluated the bite force after orthognathic surgery and reported that bite force was positively correlated with occlusal contact and recovered fully 6 months after surgery. While in the present study, after 6 months, a decrease in bite force was observed compared to the preoperative values.
Small sample size and short duration of follow-up were among the limitations of this study. Also, we could not persuade the patients to bite on the sensor as hard as they could.
Future studies with larger sample size are recommended to measure the bite force in skeletal Class II patients over a longer period of time. The function of the muscles of mastication in Class II patients and the efficacy of physiotherapy in improvement of the bite force should also be evaluated in further studies.
Conclusion
Mandibular advancement surgery in skeletal Class II patients with mandibular deficiency decreases the maximum bite force in the first 6 months, postoperatively.
Full-Text: (1283 Views)
|
Abstract
Background and Aim: The bite force changes due to alterations in the lever system of the jaw following orthognathic surgery. This study aimed to assess the changes in the maximum bite force of skeletal Class II patients between 18-30 years after orthognathic surgery compared with the preoperative state.
Materials and Methods: This inception cohort study evaluated 17 patients with skeletal Class II malocclusion (mandibular deficiency) and normal vertical dimension between 18-30 years who underwent mandibular advancement surgery. The maximum bite force on the mandibular first molars was measured preoperatively and at 6 weeks, and 3 and 6 months, postoperatively. The overjet and overbite were also measured on diagnostic casts. Data were analyzed by the Shapiro-Wilk test, Mauchly’s test, the Greenhouse–Geisser correction, and the Spearman and Pearson’s correlation coefficients. Results: The mean maximum bite force preoperatively was significantly higher than that at 6 weeks (P<0.001), 3 months (P<0.001), and 6 months (P<0.001), postoperatively. No significant difference was noted in the mean bite force in the right and left sides of the jaw (P=0.589). The overbite and maximum bite force were not significantly correlated in the right (P=0.181) or the left (P=0.134) side, preoperatively. The overjet had no significant correlation with the maximum bite force in the right (P=0.881) or the left (P=0.677) side, preoperatively. Conclusion: Mandibular advancement surgery in skeletal Class II patients with mandibular deficiency decreases the maximum bite force in the first 6 months, postoperatively. |
| Key Words: Malocclusion, Angle Class II; Bite Force; Mandibular Osteotomy; Micrognathism |
Introduction
Mastication is a complex function that involves a number of factors such as the position of the posterior teeth and the bite force [1]. After completion of permanent dentition and hormonal stability, the maximum bite force decreases and is stabilized. The masticatory forces indicate the function of the muscles of mastication and their interactions. Thus, measurement of the bite force can provide beneficial information regarding the activity and function of the muscles and dentition. The maximum bite force depends on anthropometric characteristics such as age and gender of patients [2]. The bite force is a reflection of the lever system of the mandible. In long-face individuals, the maxilla has a downward rotation. Thus, the mechanical properties of the elevator muscles decrease and; therefore, the bite force in long-face patients is lower than that in normal-face individuals. Periodontal status also influences the bite force [3].
In case of presence of compensatory movement of the teeth due to skeletal deformity, the position of the teeth should be orthodontically corrected prior to surgery, and irrespective of the relationship with the opposing arch. This procedure worsens the deformity prior to surgery; however, it is necessary in order to correct positioning of the osteotomized segments by surgery. The type of presurgical orthodontic treatment varies in different individuals.
Patients with skeletal Class II malocclusion may have mandibular deficiency, maxillary excess or a combination of both. Bilateral sagittal split osteotomy (BSSO) is the most commonly performed procedure for mandibular advancement, which is easily performed through an intraoral incision [4].
It appears that the mandible serves as a lever based on two assumptions: (I) The interaction of force vectors generated by the muscles of mastication passes through the bite point. (II) Also, the condylar neck and/or the temporomandibular joint (TMJ) are not suitable to tolerate the reaction force during mastication. Assessment of the electromyographic data and the properties of the TMJ support the mandibular lever theory. Moreover, analysis of the strength of the condylar neck indicates that this structure is strong enough to tolerate the expected reaction force during the lever function [5]. According to Proffit [6], the masticatory system is a classic lever, and the muscles are located between the support, which is the TMJ, and the point of load application i.e., between the teeth.
Considering all the above, orthognathic surgery, and particularly BSSO in Class II patients with mandibular deficiency and normal facial vertical height is expected to change their bite force; however, the efficacy of orthognathic surgery in improvement of the masticatory function is a matter of discussion.
The maximum bite force is measured to assess the effect of different dental procedures on the masticatory system such as orthodontic and prosthodontic treatments. Also, the effects of facial deformities such as malocclusion and TMJ disorders on the bite force have been previously studied [7]. However, to the best of the authors’ knowledge, no study has precisely addressed the changes in bite force after orthognathic surgery in skeletal Class II patients. Thus, considering the significance of the masticatory function and its effects on health, and the bite force as an objective and quantitative parameter for assessment of the efficiency of mastication [2], this study aimed to assess the changes in maximum bite force in skeletal Class II patients between 18-30 years after orthognathic surgery compared with the preoperative state.
The main objective of this study was to assess the maximum bite force in skeletal Class II patients with mandibular deficiency between 18-30 years before and after mandibular advancement surgery. The maximum bite force was the primary outcome. Correlations of the maximum bite force of patients before surgery with their overbite and overjet, and side of the jaw were considered as the secondary outcomes of the study.
Materials and Methods
This inception cohort study (ethical code: IR.IAU.KHUISF.REC.1398.121) was conducted on 17 skeletal Class II malocclusion patients who required mandibular advancement and presented to the Oral and Maxillofacial Surgery Department of Islamic Azad University, School of Dentistry, Khorasgan Branch.
The participants had skeletal Class II malocclusion with mandibular deficiency and no problem in vertical dimension of the face (normal face). They were between 18 to 30 years, required mandibular advancement by BSSO, and had no developmental syndromes, no cleft lip and palate, no history of jaw trauma, no TMJ problem, good general health, and optimal cooperation. All patients had received a course of orthodontic treatment for decompensation. Orthodontic treatment of patients had been scheduled to continue for at least 6 months after surgery.
The patients had no neuromuscular or neurological disorders, sensitive or mobile first molars, first molars with extensive restorations, prosthetic crowns, or bruxism or clenching.
After obtaining written informed consent from the patients, their bite force was measured preoperatively and at 6 weeks, and 3 and 6 months, postoperatively. The device used for this purpose had a load cell with a maximum capacity of 100 kg, and a digital display. This device was designed by Mahsa Rismanchian, an engineer with a Master's degree in computer science from the Islamic Azad University, Khorasgan branch) (Figure 1).
Figure 1. Bite force measuring device
{kind=link}
The sensor covered in disposable pads was first placed on the mandibular right first molar and then on the mandibular left first molar. The patients were then requested to bite on the sensor with maximum power for 5 seconds. This was repeated for each side of the jaw four times, with 5-minute resting intervals. At each time of measurement, the maximum force displayed on the monitor was recorded.
Eventually, the maximum value among all four measurements was recorded for the respective side of the jaw. The patients’ head was in natural head position for measurement of the bite force. For this purpose, the patients were in the upright position and asked to look straight ahead such that the Frankfurt plane was almost parallel to the ground. The overbite and overjet were also measured on diagnostic casts and recorded.
Sample size calculation:
The sample size was calculated to be 17 by repeated measures ANOVA using G*Power software assuming α=0.05, β=0.2, study power of 80%, mean effect size (d) of 0.3, and 4 repetitions. Considering 10% possibility of loss to follow-up, 20 patients were enrolled.
Statistical analysis:
Data were analyzed using descriptive and inferential statistics. Repeated measures ANOVA with the two repeated measures of time of measurement and side of the jaw was applied for data analysis. The normality of data distribution was evaluated by the Shapiro-Wilk test, and the Mauchly’s test was applied to test the assumption of sphericity. Data were found to be normally distributed. However, the Mauchly’s test showed that the effects of time and the interaction effect of time and side of the jaw were significant on bite force. Thus, the Greenhouse-Geisser test was applied for data analysis. The Spearman and the Pearson’s correlation coefficients were used to analyze the correlation of maximum bite force with overbite and overjet of patients. All statistical analyses were carried out by SPSS version 22 at 0.05 level of significance.
Results
Seventeen patients were evaluated including 13 women and 4 men between 18-30 years. Table 1 presents the measures of central dispersion for the maximum bite force in the right and left sides of the jaw. Repeated measures ANOVA showed that the effect of time of measurement on maximum bite force was significant (P<0.001). In other words, the mean maximum bite force of patients was significantly different at different time points. The effect of side of the jaw on maximum bite force was not significant (P=0.589). In other words, the maximum bite force was not significantly different in the right and left sides of the jaw. The interaction effect of time and laterality on bite force was not significant either (P=0.294). The Bonferroni adjustment was then applied for pairwise comparisons of the time points regarding the maximum bite force (Table 2). As shown, the mean maximum bite force at baseline was significantly higher than that at 6 weeks (P<0.001), 3 months (P<0.001) and 6 months (P<0.001). The mean maximum bite force at 6 weeks was also significantly lower than that at 3 months (P=0.014) and 6 months (P=0.001). The mean maximum bite force at 3 months was significantly lower than that at 6 months (P<0.001).
Pairwise comparisons of the mean maximum bite force at different time points separately in the right and left sides (Table 3) indicated that in the right side, the mean maximum bite force of patients preoperatively was significantly higher than that at 6 weeks (P<0.001), 3 months (P<0.001) and 6 months (P<0.001), postoperatively. The value at 6 weeks was significantly lower than that at 3 months (P=0.021) and 6 months (P<0.001). The value at 3 months was also significantly lower than that at 6 months (P<0.001). The same results were obtained in the left side.
Before the procedure, the mean overbite was 2.26±0.40 mm (range 2-3 mm), and the mean overjet was 9.52±1.03 mm (range 8-12 mm). The Spearman’s correlation test revealed no significant correlation between overbite and the maximum bite force in the right (P=0.181) or left (P=0.134) side. The Pearson’s correlation test found no significant correlation between the overjet and the maximum bite force in the right (P=0.881)
or left (P=0.677) side of the jaw. After surgery, the patients reached the normal range of overbite (1-2 mm) and the normal range of overjet (2-3 mm).
Table 1. Measures of central dispersion for the maximum bite force in the right and left sides of the jaw (n=17)
{kind=link}
Table 2. Pairwise comparisons of the time points regarding the maximum bite force
{kind=link}
Table 3. Pairwise comparisons of the mean maximum bite force at different time points separately in the right and left sides
{kind=link}
Discussion
This study assessed the changes in maximum bite force of skeletal Class II patients between 18-30 years after orthognathic surgery compared with the preoperative state. The results indicated that the mean maximum bite force at 6 weeks after the procedure was significantly lower than that before the procedure. The maximum bite force significantly increased at 3 and 6 months but was still lower than the baseline preoperative value. This trend suggests that the bite force may eventually return to the baseline value in longer eriods of time, which calls for studies with longer follow-ups. Reduction in bite force after orthognathic surgery in the present study can be attributed to postoperative edema, inflammation and pain. Also, patients have a soft diet for at least 1 month after orthognathic surgery, which also weakens the muscles of mastication. This explains the lowest bite force at 6 weeks, postoperatively. Physiotherapy and exercise improved the muscle function and increased the bite force at 3 and then at 6 months.
Also, the patients may have fear of biting hard on the sensor after surgery, which may also explain the reduction in bite force. Furthermore, after mandibular advancement, the distance between the teeth (site of load application) and muscles increases; thus, the maximum bite force is also expected to decrease. However, since the magnitude of mandibular advancement is small (relative to the jaw length), the change in bite force is also small. Increased maximum bite force after orthognathic surgery in some studies may be due to the use of screw and plate for jaw fixation and its psychological effect on patients, which would give them the courage to bite harder on the sensor. Also, correction of Class II relationship improves the contact of tooth surfaces in centric occlusion, and subsequently increases the efficiency of mastication and the maximum bite force [8].
Celakil et al. [6] evaluated the effect of orthognathic surgery on muscle function of skeletal Class III patients. They evaluated electromyographic activity before and after splinting and at 1 and 6-8 months after orthognathic surgery. The present study was conducted on Class II patients who needed mandibular advancement. Despite the different methods, their results were consistent with ours and showed a decrease in bite force after orthognathic surgery. Firoozeie et al. [9] evaluated the changes in bite force and electromyographic activity of the muscles of mastication in patients with mandibular prognathism following orthognathic surgery. They reported that at 3 months postoperatively, the bite force and the electromyographic activity of the masticatory muscles of patients were lower than the corresponding values before surgery. All parameters improved at 6 months after surgery but the maximum bite force at the molar site did not reach the preoperative state. The same results were obtained in the present study regarding the reduction in bite force by up to 6 months. Islam et al. [10] systematically evaluated the changes in bite force after orthognathic surgery for correction of mandibular prognathism. They reviewed 17 articles and a total of 697 patients between 15-44 years. A total of 532 patients underwent BSSO, 108 underwent intraoral vertical ramus osteotomy and 24 underwent extraoral vertical ramus osteotomy. They concluded that the efficiency of mastication at 3 months after surgery was higher than that before surgery, and this improvement was significant after 6 months. Also, the occlusal contact points and surfaces increased after 3 months; this increase was significant after 12 months. The occlusal forces improved as well. However, the values in corrected prognathic patients were still lower than the corresponding values in normognathic patients 2 years after surgery. Similarly, the present study showed that the maximum bite force at 6 months after surgery was still lower than the baseline value. In the present study, in contrast to the findings of Islam et al. [10], the efficacy of mastication at 3 and 6 months after surgery was lower than that before the procedure. The occlusal contact points and surfaces improved at 3 and 6 months postoperatively in the present study, due to the conversion of Class II to Class I occlusion, which was in agreement with the results of Islam et al, [10].
However, it should be noted that Islam et al. [10] evaluated Class III patients while the present study was conducted on Class II patients.
Yari et al. [8], conducted a study that compared the maximum bite force in skeletal Class III patients before and after orthognathic surgery. They examined the maximum bite force before surgery and 3 months after surgery. Their results were consistent with ours, and the patients showed a decrease in bite force 3 months after surgery. Naguib et al. [11] investigated the changes in masticatory muscles following orthognathic surgery (BSSO for correction of skeletal Class III deformity). In contrast to our study, no changes in temporalis and masseter muscle contraction strength were observed after BSSO as determined by EMG examination. Hu et al. [12] evaluated the bite force after orthognathic surgery and reported that bite force was positively correlated with occlusal contact and recovered fully 6 months after surgery. While in the present study, after 6 months, a decrease in bite force was observed compared to the preoperative values.
Small sample size and short duration of follow-up were among the limitations of this study. Also, we could not persuade the patients to bite on the sensor as hard as they could.
Future studies with larger sample size are recommended to measure the bite force in skeletal Class II patients over a longer period of time. The function of the muscles of mastication in Class II patients and the efficacy of physiotherapy in improvement of the bite force should also be evaluated in further studies.
Conclusion
Mandibular advancement surgery in skeletal Class II patients with mandibular deficiency decreases the maximum bite force in the first 6 months, postoperatively.
Type of Study: Original article |
Subject:
orthodontic
References
1. Hatch JP, Shinkai RS, Sakai S, Rugh JD, Paunovich ED. Determinants of masticatory performance in dentate adults. Arch Oral Biol. 2001 Jul;46(7):641-8. [DOI:10.1016/S0003-9969(01)00023-1] [PMID]
2. Takaki P, Vieira M, Bommarito S. Maximum bite force analysis in different age groups. Int Arch Otorhinolaryngol. 2014 Jul;18(3):272-6. [DOI:10.1055/s-0034-1374647] [PMID] []
3. Koc D, Dogan A, Bek B. Bite force and influential factors on bite force measurements: a literature review. Eur J Dent. 2010 Apr;4(2):223-32. [DOI:10.1055/s-0039-1697833] [PMID] []
4. Hupp JR, Tucker MR, Ellis E. Contemporary oral and maxillofacial surgery. 7th ed. St. Louis: Elsevier; 2019. p. 269-72.
5. Hylander WL. The human mandible: lever or link? Am J Phys Anthropol. 1975 Sep;43(2):227-42. [DOI:10.1002/ajpa.1330430209] [PMID]
6. Celakil D, Ozdemir F, Eraydin F, Celakil T. Effect of orthognath-ic surgery on masticatory performance and muscle activity in skeletal Class III patients. Cranio. 2018 May; 36 (3):174-80. [DOI:10.1080/08869634.2017.1311395] [PMID]
7. Al-Gunaid TH. Bite force -What we should know: A literature review. Int J Orthod Rehabil. 2019;10(4):168-74. [DOI:10.4103/ijor.ijor_33_19]
8. Yari F, Rafiei M, Golestaneh A, Ehrami E. Comparison of Maxi-mum Bite Force in Class Ш Skeletal Patients Before and After Orthognathic Surgery. J Isfahan Dent Sch. 2022; 18(1): 18-24. [DOI:10.18502/ijds.v18i1.10068]
9. Firoozeie G, Golestaneh A, Shirvani A. Changes in bite force and electromyographic activities of masticatory muscles in prognathic patients after orthognathic surgery. J Iran Dent Assoc. 2009; 21(3) :202-8.
10. Islam I, Lim AAT, Wong RCW. Changes in bite force after orthognathic surgical correction of mandibular prognathism: a systematic review. Int J Oral Maxillofac Surg. 2017 Jun; 46 (6):746-55. [DOI:10.1016/j.ijom.2017.01.012] [PMID]
11. Naguib A, Abdelmabood A, Naguib R. Changes in Masticatory Muscles Following Orthognathic Surgery After Mandibular Prognathism Correction. Egyptian Dental Journal. 2021;67(3):1915-23. [DOI:10.21608/edj.2021.66311.1540]
12. Hu HL, Lin ShC, Wu YY, Tun YY, Cheng MC, Yao CCJ, et al. Bite Force and Maximum Mouth Opening after Orthognathic Surgery. Taiwanese Journal of Orthodontics. 2013 Jan;25 (4):204-10.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |