Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 102-109 |
Back to browse issues page


Ethics code: IR.KMU.REC.1396.1944
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Habib Agahi R, Navabi N, Sarabi M. Oral Health-Related Quality of Life in Patients with Denture Stomatitis and Recovery after Antifungal Treatment. J Res Dent Maxillofac Sci 2023; 8 (2) :102-109
URL: http://jrdms.dentaliau.ac.ir/article-1-436-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-436-en.html



1- Orthodontic Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
2- Department of Oral Medicine, Kerman University of Medical Sciences, Kerman, Iran ,nader_nawabi@yahoo.com
3- Private Dental Practice, Kerman, Iran
2- Department of Oral Medicine, Kerman University of Medical Sciences, Kerman, Iran ,
3- Private Dental Practice, Kerman, Iran
Full-Text [PDF 710 kb]
(1113 Downloads)
| Abstract (HTML) (2892 Views)
Introduction
Some oral mucosal lesions occur due to acute or chronic irritation by denture-related factors. These lesions are referred to as denture-related mucosal lesions. Denture stomatitis (DS) is among the most common denture-related mucosal lesions [1]. DS is the inflammatory response of tissues in the palatal mucosa of the maxilla covered by a removable denture [2-4]. Other terms are also used to refer to this condition, including denture-induced stomatitis or denture-related stomatitis [5]. The prevalence of DS ranges from 15% to 75% in denture wearers, and it has been reported that this condition affects around 60% of denture wearers to some degrees [2,3]. A higher prevalence of DS has been reported in individuals > 60 years of age [3,6,7]. In an epidemiological study, DS was reported as one of the 10 most common oral mucosal lesions [8]. The clinical manifestations of DS mainly include inflammation, shiny erythema, and edema. Candida fungal species are isolated from 65-84.1% of the elderly denture wearers. The most plausible hypothesis about the pathogenesis of DS is chronic atrophic Candida infection [9,10].
Candida albicans (C. albicans) is the chief etiologic factor for DS, and in most studies, this fungal species, which is the most prevalent fungus in the oral microflora, has been reported to be associated with the occurrence of DS [11-14]. Therefore, DS has been classified under the category of candida-associated lesions of the oral cavity. Accordingly, anti-fungal treatment is the most effective approach to treat this condition. Proper and timely anti-fungal treatment can eliminate contamination with C. albicans and help resolve DS symptoms. Azole derivatives are among the most commonly used anti-fungal agents to treat DS [15-17].
DS remains almost undiagnosed in almost all patients due to its asymptomatic nature [6]. C. albicans in the oral cavity of patients with DS increases the risk of cytotoxic effects on the adjacent tissue cells, dysplasia, and precancerous changes. Therefore, DS should be treated even in the absence of any symptom [2,11]. In addition, high prevalence rate of edentulism in developing countries (including Iran) leading to a high percentage of denture wearers in these countries, high percentage of C. albicans colonization as an important component of the oral microflora of denture wearers, and high prevalence of DS after long-term denture use are of great significance. Oral health-related quality of life (OHRQoL) is defined as an individual evaluation of how the physical, psychological, and social aspects affect the well-being and discomfort experienced in relation to orofacial conditions [18]. The present study was undertaken to assess the OHRQoL of patients with DS and its improvement after anti-fungal treatment of DS as the first study investigating this topic.
Materials and Methods
The present quasi-experimental study was done in Kerman, Iran. The participants were assigned to three groups: participants with at least 20 natural teeth without a removable denture (the control group), those wearing a maxillary complete denture without DS, and patients wearing a maxillary complete denture with DS. A convenience sampling technique was used for selection of participants by referring to the retired employee section of state organizations (the education system, banks, military centers, etc.). The inclusion criteria consisted of wearing a maxillary complete denture for at least 6 months (in groups 2 and 3) and a minimum age of 50 years.
The exclusion criteria included positive history of a chronic systemic condition such as diabetes mellitus, affliction with other related oral lesions such as epulis fissuratum and other forms of oral conditions such as median rhomboid glossitis, continuous use of medications such as antibiotics, oral rinses, or oral steroids in the past 1-month, continuous use of tobacco and alcohol, and history of long-term xerostomia [6,17].
DS is characterized by chronic inflammation, erythema and edema of the palatal mucosa beneath the base of the maxillary removable acrylic denture. A diagnosis of DS was made through a clinical examination using a sterile disposable examination set under sufficient light, based on the Newton’s classification:
Type I: Local inflammation and pin-point petechia
Type II: Widespread erythema in areas covered by denture
Type III: Erythematous areas in the form of inflamed, red papules, referred to as inflammatory papillary hyperplasia [9,15].
The participants were examined by a senior dental student trained for this purpose. The suspected DS cases were referred to an oral medicine specialist for a definitive diagnosis. Patients with types I and II were enrolled.
The standardized Persian version of the oral health impact profile (OHIP-14) questionnaire was used to determine the OHRQoL. This questionnaire is the most commonly used questionnaire for this purpose. It consists of 14 questions. The respondents answer the questions, with each question dealing with one of the problems related to the oral and dental status or denture in the past 12 months. These problems are, in fact, experiences about the physical, psychological, and social problems that are manifested as pain, discomfort, or inability. The Likert scale was used to analyze the responses, with a score of 4 for ‘always’, a score of 3 for ‘in most occasions,’ a score of 2 for ‘sometimes,’ a score of 1 for ‘seldom’, and a score of 0 for ‘never’. Therefore, the total score range for OHIP-14 is 0-56, with lower scores indicating higher OHRQoL. In addition, the questionnaire examines seven domains as follows: questions 1 and 2: the performance domain, questions 3 and 4: physical discomfort, questions 5 and 6: psychological discomfort, questions 7 and 8: physical inability, questions 9 and 10: psychological inability, questions 11 and 12: social inability, and questions 13 and 14: total inability [18,19].
After determining the OHRQoL in the three study groups, oral administration of fluconazole capsules (100 mg once daily; Rouz Darou, Iran) was initiated in group 3 for 2 weeks, in association with recommendations for daily washing of the inner surface of the denture and not wearing the denture at night [15]. The OHIP-14 questionnaire was completed again after 2 weeks. In case of any adverse drug reaction to fluconazole, the treatment was stopped and the patient was excluded from the study. The sample size was estimated at 75 (n=25 in each group) based on a previous study with α=0.05 and power=80% (19). The data were analyzed by SPSS 26, using the Pearson’s correlation coefficient, Fisher’s exact test, and one-way ANOVA to analyze the inter-group differences, followed by the Tukey’s post-hoc test. The participants participated in the study voluntarily. The patients’ demographic data were kept confidential throughout the study and after it.
The Ethics Committee of Kerman University of Medical Sciences, Kerman, Iran approved the protocol of the study (code: IR.KMU.REC.1396.1944.). Informed consent was obtained from all participants before participating in the study. All personal and identifying information was kept confidential.
Results
A total of 85 participants participated in the present study (n=30 in the control group with natural teeth, n=30 in denture wearer group without DS, and n=25 in denture wearer group with DS) including 51 males (60%) and 34 females (40%). There were no significant differences among the three study groups in gender distribution (Pearson’s chi-squared, P=0.36). In addition, there was no significant difference in educational level of the study groups (Fisher’s exact test, P=0.41). ANOVA showed a significantly higher mean age in the DS group than the other two groups (P=0.001). Comparison of the OHIP-14 questionnaire scores among the three groups showed the lowest score in the control and denture wearer without DS groups, and the highest score in the denture wearer with DS group. ANOVA showed a higher mean score for the OHIP-14 questionnaire in this group than the other two groups (P=0.0001); in other words, the OHRQoL of this group was lower than the other two groups (Table 1). The analysis of the OHIP-14 questionnaire scores in the seven domains with ANOVA showed significant differences in the mean OHRQoL scores between the DS group and the other two groups in all seven domains (P=0.003 for the psychological discomfort, and P=0.000 for the other six domains). The OHRQoL of the patients with DS in all the domains was lower than the other two groups.
Full-Text: (1346 Views)
| Abstract
Background and Aim: Denture stomatitis (DS) is a common oral condition which usually occurs under the maxillary removable complete dentures. Infection by Candida albicans (C. albicans) is considered as the main etiology of this lesion. The aim of the present study was to assess the oral health-related quality of life (OHRQoL) of patients with DS and its improvement after antifungal treatment. Materials and Methods: In the present quasi-experimental study, the patients were classified into three groups with natural teeth, complete denture wearers without DS, and DS group. The Oral Health Impact Profile (OHIP-14) questionnaire was completed once by the first two groups and twice by the DS group (before and after prescription of 100 mg fluconazole daily for 14 days). Data analysis was performed by one-way ANOVA, Fisher’s exact test, and Pearson’s correlation coefficient at a confidence interval of 95%. Results: A total of 85 patients were included with a mean age of 69.74±7.95 years. The mean OHIP score was significantly lower in the DS group in comparison with the other two groups (P=0.0001). OHRQoL significantly improved after prescription of fluconazole for DS patients (P=0.0001). Conclusion: It appears that DS disrupts the OHRQoL of the affected patients, and systemic antifungal therapy has the potential to improve it. Key Words: Quality of Life; Stomatitis; Dentures; Antifungal Agents |
Introduction
Some oral mucosal lesions occur due to acute or chronic irritation by denture-related factors. These lesions are referred to as denture-related mucosal lesions. Denture stomatitis (DS) is among the most common denture-related mucosal lesions [1]. DS is the inflammatory response of tissues in the palatal mucosa of the maxilla covered by a removable denture [2-4]. Other terms are also used to refer to this condition, including denture-induced stomatitis or denture-related stomatitis [5]. The prevalence of DS ranges from 15% to 75% in denture wearers, and it has been reported that this condition affects around 60% of denture wearers to some degrees [2,3]. A higher prevalence of DS has been reported in individuals > 60 years of age [3,6,7]. In an epidemiological study, DS was reported as one of the 10 most common oral mucosal lesions [8]. The clinical manifestations of DS mainly include inflammation, shiny erythema, and edema. Candida fungal species are isolated from 65-84.1% of the elderly denture wearers. The most plausible hypothesis about the pathogenesis of DS is chronic atrophic Candida infection [9,10].
Candida albicans (C. albicans) is the chief etiologic factor for DS, and in most studies, this fungal species, which is the most prevalent fungus in the oral microflora, has been reported to be associated with the occurrence of DS [11-14]. Therefore, DS has been classified under the category of candida-associated lesions of the oral cavity. Accordingly, anti-fungal treatment is the most effective approach to treat this condition. Proper and timely anti-fungal treatment can eliminate contamination with C. albicans and help resolve DS symptoms. Azole derivatives are among the most commonly used anti-fungal agents to treat DS [15-17].
DS remains almost undiagnosed in almost all patients due to its asymptomatic nature [6]. C. albicans in the oral cavity of patients with DS increases the risk of cytotoxic effects on the adjacent tissue cells, dysplasia, and precancerous changes. Therefore, DS should be treated even in the absence of any symptom [2,11]. In addition, high prevalence rate of edentulism in developing countries (including Iran) leading to a high percentage of denture wearers in these countries, high percentage of C. albicans colonization as an important component of the oral microflora of denture wearers, and high prevalence of DS after long-term denture use are of great significance. Oral health-related quality of life (OHRQoL) is defined as an individual evaluation of how the physical, psychological, and social aspects affect the well-being and discomfort experienced in relation to orofacial conditions [18]. The present study was undertaken to assess the OHRQoL of patients with DS and its improvement after anti-fungal treatment of DS as the first study investigating this topic.
Materials and Methods
The present quasi-experimental study was done in Kerman, Iran. The participants were assigned to three groups: participants with at least 20 natural teeth without a removable denture (the control group), those wearing a maxillary complete denture without DS, and patients wearing a maxillary complete denture with DS. A convenience sampling technique was used for selection of participants by referring to the retired employee section of state organizations (the education system, banks, military centers, etc.). The inclusion criteria consisted of wearing a maxillary complete denture for at least 6 months (in groups 2 and 3) and a minimum age of 50 years.
The exclusion criteria included positive history of a chronic systemic condition such as diabetes mellitus, affliction with other related oral lesions such as epulis fissuratum and other forms of oral conditions such as median rhomboid glossitis, continuous use of medications such as antibiotics, oral rinses, or oral steroids in the past 1-month, continuous use of tobacco and alcohol, and history of long-term xerostomia [6,17].
DS is characterized by chronic inflammation, erythema and edema of the palatal mucosa beneath the base of the maxillary removable acrylic denture. A diagnosis of DS was made through a clinical examination using a sterile disposable examination set under sufficient light, based on the Newton’s classification:
Type I: Local inflammation and pin-point petechia
Type II: Widespread erythema in areas covered by denture
Type III: Erythematous areas in the form of inflamed, red papules, referred to as inflammatory papillary hyperplasia [9,15].
The participants were examined by a senior dental student trained for this purpose. The suspected DS cases were referred to an oral medicine specialist for a definitive diagnosis. Patients with types I and II were enrolled.
The standardized Persian version of the oral health impact profile (OHIP-14) questionnaire was used to determine the OHRQoL. This questionnaire is the most commonly used questionnaire for this purpose. It consists of 14 questions. The respondents answer the questions, with each question dealing with one of the problems related to the oral and dental status or denture in the past 12 months. These problems are, in fact, experiences about the physical, psychological, and social problems that are manifested as pain, discomfort, or inability. The Likert scale was used to analyze the responses, with a score of 4 for ‘always’, a score of 3 for ‘in most occasions,’ a score of 2 for ‘sometimes,’ a score of 1 for ‘seldom’, and a score of 0 for ‘never’. Therefore, the total score range for OHIP-14 is 0-56, with lower scores indicating higher OHRQoL. In addition, the questionnaire examines seven domains as follows: questions 1 and 2: the performance domain, questions 3 and 4: physical discomfort, questions 5 and 6: psychological discomfort, questions 7 and 8: physical inability, questions 9 and 10: psychological inability, questions 11 and 12: social inability, and questions 13 and 14: total inability [18,19].
After determining the OHRQoL in the three study groups, oral administration of fluconazole capsules (100 mg once daily; Rouz Darou, Iran) was initiated in group 3 for 2 weeks, in association with recommendations for daily washing of the inner surface of the denture and not wearing the denture at night [15]. The OHIP-14 questionnaire was completed again after 2 weeks. In case of any adverse drug reaction to fluconazole, the treatment was stopped and the patient was excluded from the study. The sample size was estimated at 75 (n=25 in each group) based on a previous study with α=0.05 and power=80% (19). The data were analyzed by SPSS 26, using the Pearson’s correlation coefficient, Fisher’s exact test, and one-way ANOVA to analyze the inter-group differences, followed by the Tukey’s post-hoc test. The participants participated in the study voluntarily. The patients’ demographic data were kept confidential throughout the study and after it.
The Ethics Committee of Kerman University of Medical Sciences, Kerman, Iran approved the protocol of the study (code: IR.KMU.REC.1396.1944.). Informed consent was obtained from all participants before participating in the study. All personal and identifying information was kept confidential.
Results
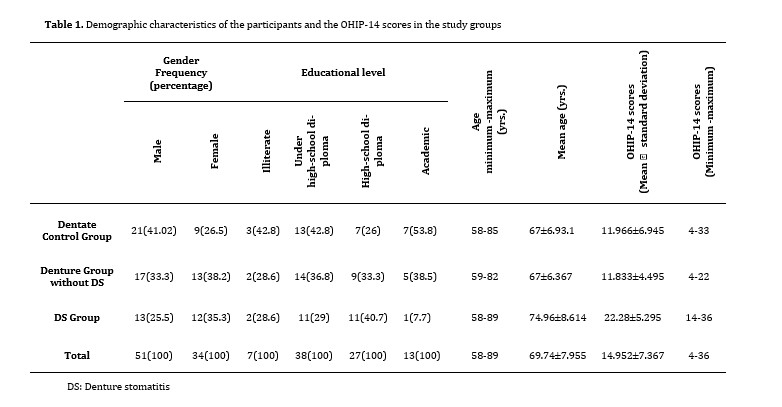
A total of 85 participants participated in the present study (n=30 in the control group with natural teeth, n=30 in denture wearer group without DS, and n=25 in denture wearer group with DS) including 51 males (60%) and 34 females (40%). There were no significant differences among the three study groups in gender distribution (Pearson’s chi-squared, P=0.36). In addition, there was no significant difference in educational level of the study groups (Fisher’s exact test, P=0.41). ANOVA showed a significantly higher mean age in the DS group than the other two groups (P=0.001). Comparison of the OHIP-14 questionnaire scores among the three groups showed the lowest score in the control and denture wearer without DS groups, and the highest score in the denture wearer with DS group. ANOVA showed a higher mean score for the OHIP-14 questionnaire in this group than the other two groups (P=0.0001); in other words, the OHRQoL of this group was lower than the other two groups (Table 1). The analysis of the OHIP-14 questionnaire scores in the seven domains with ANOVA showed significant differences in the mean OHRQoL scores between the DS group and the other two groups in all seven domains (P=0.003 for the psychological discomfort, and P=0.000 for the other six domains). The OHRQoL of the patients with DS in all the domains was lower than the other two groups.
Table 1. Demographic characteristics of the participants and the OHIP-14 scores in the study groups
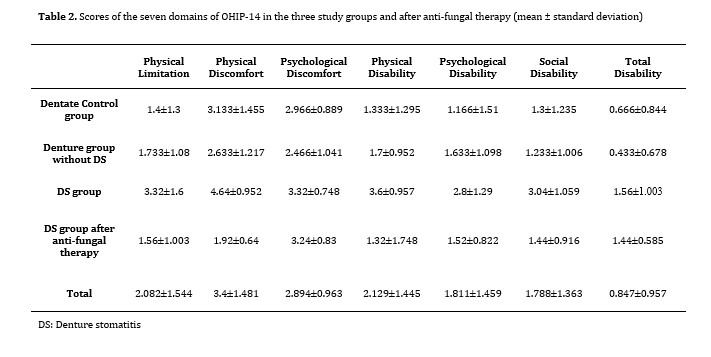
The mean OHRQoL score in the DS group was 11.56±2.599 after anti-fungal treatment, which was significantly different from that before treatment (P=0.0001). Oral anti-fungal treatment resulted in a significant improvement in OHRQoL of patients with DS. In addition, the mean scores in the seven domains of the OHIP-14 questionnaire in patients with DS showed significant differences in all the domains (P=0.0001),
except for the third domain (psychological discomfort) (P=0.6147,Table 2). No adverse drug reaction to fluconazole was seen.
Table 2. Scores of the seven domains of OHIP-14 in the three study groups and after anti-fungal therapy (mean ± standard deviation)
Discussion
The present study was the first investigation into the OHRQoL of patients with DS. The two main findings of the present study indicated a lower quality of life in patients with DS than the dentate patients and patients wearing complete dentures without DS. Anti-fungal oral treatment in these patients improved their quality of life.
Some other researchers have evaluated changes in the quality of life of patients with other prevalent oral lesions. Nassab et al. evaluated the quality of life of 39 patients with lichen planus, pemphigus vulgaris, recurrent aphthous stomatitis, and leukoplakia, reporting that the clinicians in charge of treating these conditions should pay attention to symptomatic treatment and resolution of these lesions [20]. Farhang et al. [21] studied 101 patients and reported that chronic oral lesions affected the patients’ quality of life. They also evaluated exophytic oral lesions in addition to the four lesions evaluated by Nassab et al [20]. Concerning efforts to improve the quality of life in patients with prevalent oral mucosal lesions, several studies evaluated recurrent aphthous stomatitis. Kurklu-Gurleyen et al. used the OHIP-14 questionnaire, similar to the present study, to evaluate the efficacy of a mucosal paste containing citrus extract for improvement of OHRQoL in patients with recurrent oral aphthous stomatitis. The results showed improvements in the general score of the tool in different domains of oral functions, consistent with the present study [22]. In addition, some others evaluated the quality of life of patients with oral lichen planus. Nagao and Sata [23] evaluated the efficacy of an oral protective gel (a type of therapeutic toothpaste) on the quality of life of patients with oral lichen planus and chronic hepatitis C at the same time. The results showed an improvement in the quality of life of patients. Similar to the present study, lower OHRQoL in patients with DS was also reported by Anadioti et al. [24]; however, their study was carried out on patients with implant-supported overdentures. They used the OHIP tool, and it can be claimed that this tool is the gold standard for evaluation of OHRQoL [24].
However, in a study by Mendes et al. [25], elderly patients were evaluated using the Geriatric Oral Health Assessment Index. The question is why DS leads to a reduction in OHRQoL. If the multifunctional etiology of DS is taken into account, it becomes evident that poor denture hygiene is among the factors exacerbating Candida contamination on the tissue surface of dentures [26,27]. In addition, research has shown that delayed visits to the clinician fabricating the denture, poor financial status (forcing the patients to refer to a laboratory technician rather than a dentist to fabricate a denture), and improper use of denture (round the clock use) affect the incidence of DS [9,28]. Therefore, it is clear that sociocultural factors have a role in the incidence of such lesions. However, since DS is not visible as it develops under the maxillary denture in many patients, and since it does not have severe symptoms, it is not expected to disrupt oral functions. This characteristic complicates the relationship between DS and the functional and psychological domains to some extent. However, in contrast, if the patients’ attention is directed towards the lesion and scattered or prominent redness of the hard palate, they may become concerned about the lesion and its possible malignant nature.
The second finding of the present study was the optimal efficacy of oral fluconazole for improvement of OHRQoL in patients with DS. Nystatin drop is routinely prescribed to treat oral candidiasis, which requires preparation of suspension by the patient; in addition, it has a bitter taste, which is a drawback. Oral fluconazole is the most commonly used systemic medication to treat oral candidiasis, with minimal side effects due to its systemic use. It has been introduced as a safe and well-tolerated medication for treatment of infections such as DS [15]. However, a meta-analysis by Hilgert et al. did not report an effective treatment option for DS; in other words, there is no standard therapeutic protocol for it [4], as confirmed by a systematic review by Yarborough et al. [29]. Therefore, similar to the present study, the best available option should be used. Sutula et al. used the OHIP tool and reported that using a topical treatment to decrease the pathogenic oral microflora did not significantly affect the quality of life of patients [30]. However, Mahdavi Omran et al. concluded that azole derivatives (including fluconazole) were effective in preventing the growth and proliferation of Candida species isolated from the oral cavity of Iranian patients with DS [31], which was almost consistent with the present findings.
Psychological discomfort is the only aspect of OHRQoL, which was not significantly affected by prescribing oral fluconazole for patients with DS. As discussed above, studies have reported that these psychological aspects are predominantly related to facial esthetics, and other than changes in the psychological status of patients and concerns about the nature of the lesion and the possibility of malignancy, no other changes are expected. It is a little complicated why in the present study, there was no significant difference in the OHRQoL of patients wearing a denture without DS and those with natural teeth. It might be attributed to individuals’ expectations and satisfaction with their dental status. Batisse et al. reported that masticatory efficiency is an influential factor to improve OHRQoL over time [32], and it is probable that individuals wearing a denture are adequately satisfied with their mastication.
It is highly difficult to standardize the participants in terms of factors such as the type and efficacy of denture hygiene measures taken by patients, denture fabrication quality, the clinician in charge of denture fabrication, and the time passed since the fabrication of denture [21]. Therefore, it can be considered as a limitation of this study. Another limitation of this study was impossible standardization of the two groups (affected by DS) in terms of severity of lesions because of small number of cases. Future studies with a larger sample size are required in order to standardize the patients in this regard.
Conclusion
The present study showed that the OHRQoL of patients with DS was lower than that of dentate patients and those wearing a denture without DS. Also, oral anti-fungal treatment helped resolve DS.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The study protocol was approved by the Ethics Committee of Kerman University of Medical Sciences (IR.KMUREC.1396.1944).
Funding
This study was funded by Kerman University of Medical Sciences.
Acknowledgement
This study was financially supported by Social Determinants on Oral Health Research Center, Kerman University of Medical Sciences, Kerman, Iran (Research No: 96/697). The authors appreciate the sincere cooperation of this center.
{kind=link}
The mean OHRQoL score in the DS group was 11.56±2.599 after anti-fungal treatment, which was significantly different from that before treatment (P=0.0001). Oral anti-fungal treatment resulted in a significant improvement in OHRQoL of patients with DS. In addition, the mean scores in the seven domains of the OHIP-14 questionnaire in patients with DS showed significant differences in all the domains (P=0.0001),
except for the third domain (psychological discomfort) (P=0.6147,Table 2). No adverse drug reaction to fluconazole was seen.
Table 2. Scores of the seven domains of OHIP-14 in the three study groups and after anti-fungal therapy (mean ± standard deviation)
{kind=link}
Discussion
The present study was the first investigation into the OHRQoL of patients with DS. The two main findings of the present study indicated a lower quality of life in patients with DS than the dentate patients and patients wearing complete dentures without DS. Anti-fungal oral treatment in these patients improved their quality of life.
Some other researchers have evaluated changes in the quality of life of patients with other prevalent oral lesions. Nassab et al. evaluated the quality of life of 39 patients with lichen planus, pemphigus vulgaris, recurrent aphthous stomatitis, and leukoplakia, reporting that the clinicians in charge of treating these conditions should pay attention to symptomatic treatment and resolution of these lesions [20]. Farhang et al. [21] studied 101 patients and reported that chronic oral lesions affected the patients’ quality of life. They also evaluated exophytic oral lesions in addition to the four lesions evaluated by Nassab et al [20]. Concerning efforts to improve the quality of life in patients with prevalent oral mucosal lesions, several studies evaluated recurrent aphthous stomatitis. Kurklu-Gurleyen et al. used the OHIP-14 questionnaire, similar to the present study, to evaluate the efficacy of a mucosal paste containing citrus extract for improvement of OHRQoL in patients with recurrent oral aphthous stomatitis. The results showed improvements in the general score of the tool in different domains of oral functions, consistent with the present study [22]. In addition, some others evaluated the quality of life of patients with oral lichen planus. Nagao and Sata [23] evaluated the efficacy of an oral protective gel (a type of therapeutic toothpaste) on the quality of life of patients with oral lichen planus and chronic hepatitis C at the same time. The results showed an improvement in the quality of life of patients. Similar to the present study, lower OHRQoL in patients with DS was also reported by Anadioti et al. [24]; however, their study was carried out on patients with implant-supported overdentures. They used the OHIP tool, and it can be claimed that this tool is the gold standard for evaluation of OHRQoL [24].
However, in a study by Mendes et al. [25], elderly patients were evaluated using the Geriatric Oral Health Assessment Index. The question is why DS leads to a reduction in OHRQoL. If the multifunctional etiology of DS is taken into account, it becomes evident that poor denture hygiene is among the factors exacerbating Candida contamination on the tissue surface of dentures [26,27]. In addition, research has shown that delayed visits to the clinician fabricating the denture, poor financial status (forcing the patients to refer to a laboratory technician rather than a dentist to fabricate a denture), and improper use of denture (round the clock use) affect the incidence of DS [9,28]. Therefore, it is clear that sociocultural factors have a role in the incidence of such lesions. However, since DS is not visible as it develops under the maxillary denture in many patients, and since it does not have severe symptoms, it is not expected to disrupt oral functions. This characteristic complicates the relationship between DS and the functional and psychological domains to some extent. However, in contrast, if the patients’ attention is directed towards the lesion and scattered or prominent redness of the hard palate, they may become concerned about the lesion and its possible malignant nature.
The second finding of the present study was the optimal efficacy of oral fluconazole for improvement of OHRQoL in patients with DS. Nystatin drop is routinely prescribed to treat oral candidiasis, which requires preparation of suspension by the patient; in addition, it has a bitter taste, which is a drawback. Oral fluconazole is the most commonly used systemic medication to treat oral candidiasis, with minimal side effects due to its systemic use. It has been introduced as a safe and well-tolerated medication for treatment of infections such as DS [15]. However, a meta-analysis by Hilgert et al. did not report an effective treatment option for DS; in other words, there is no standard therapeutic protocol for it [4], as confirmed by a systematic review by Yarborough et al. [29]. Therefore, similar to the present study, the best available option should be used. Sutula et al. used the OHIP tool and reported that using a topical treatment to decrease the pathogenic oral microflora did not significantly affect the quality of life of patients [30]. However, Mahdavi Omran et al. concluded that azole derivatives (including fluconazole) were effective in preventing the growth and proliferation of Candida species isolated from the oral cavity of Iranian patients with DS [31], which was almost consistent with the present findings.
Psychological discomfort is the only aspect of OHRQoL, which was not significantly affected by prescribing oral fluconazole for patients with DS. As discussed above, studies have reported that these psychological aspects are predominantly related to facial esthetics, and other than changes in the psychological status of patients and concerns about the nature of the lesion and the possibility of malignancy, no other changes are expected. It is a little complicated why in the present study, there was no significant difference in the OHRQoL of patients wearing a denture without DS and those with natural teeth. It might be attributed to individuals’ expectations and satisfaction with their dental status. Batisse et al. reported that masticatory efficiency is an influential factor to improve OHRQoL over time [32], and it is probable that individuals wearing a denture are adequately satisfied with their mastication.
It is highly difficult to standardize the participants in terms of factors such as the type and efficacy of denture hygiene measures taken by patients, denture fabrication quality, the clinician in charge of denture fabrication, and the time passed since the fabrication of denture [21]. Therefore, it can be considered as a limitation of this study. Another limitation of this study was impossible standardization of the two groups (affected by DS) in terms of severity of lesions because of small number of cases. Future studies with a larger sample size are required in order to standardize the patients in this regard.
Conclusion
The present study showed that the OHRQoL of patients with DS was lower than that of dentate patients and those wearing a denture without DS. Also, oral anti-fungal treatment helped resolve DS.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The study protocol was approved by the Ethics Committee of Kerman University of Medical Sciences (IR.KMUREC.1396.1944).
Funding
This study was funded by Kerman University of Medical Sciences.
Acknowledgement
This study was financially supported by Social Determinants on Oral Health Research Center, Kerman University of Medical Sciences, Kerman, Iran (Research No: 96/697). The authors appreciate the sincere cooperation of this center.
Type of Study: Original article |
Subject:
Oral medicin
References
1. Sugio CYC, Garcia AAMN, Albach T, Moraes GS, Bonfante EA, Urban VM, Neppelenbroek KH. Candida-Associated Denture Stomatitis and Murine Models: What Is the Importance and Scientific Evidence? J Fungi (Basel). 2020 May 23;6(2):70. [DOI:10.3390/jof6020070] [PMID] [PMCID]
2. Salerno C, Pascale M, Contaldo M, Esposito V, Busciolano M, Milillo L, Guida A, Petruzzi M, Serpico R. Candida-associated denture stomatitis. Med Oral Patol Oral Cir Bucal. 2011 Mar 1;16(2):e139-43. [DOI:10.4317/medoral.16.e139] [PMID]
3. Gendreau L, Loewy ZG. Epidemiology and etiology of denture stomatitis. J Prosthodont. 2011 Jun;20(4):251-60. [DOI:10.1111/j.1532-849X.2011.00698.x] [PMID]
4. Hilgert JB, Giordani JM, de Souza RF, Wendland EM, D'Avila OP, Hugo FN. Interventions for the Management of Den-ture Stomatitis: A Systematic Review and Meta-Analysis. J Am Geriatr Soc. 2016 Dec;64(12):2539-45. [DOI:10.1111/jgs.14399] [PMID]
5. Sánchez-Vargas LO, Estrada-Barraza D, Pozos-Guillen AJ, Ri-vas-Caceres R. Biofilm formation by oral clinical isolates of Can-dida species. Arch Oral Biol. 2013 Oct;58(10):1318-26. [DOI:10.1016/j.archoralbio.2013.06.006] [PMID]
6. Contaldo M, Romano A, Mascitti M, Fiori F, Della Vella F, Ser-pico R, Santarelli A. Association between denture stomatitis, candida species and diabetic status. J Biol Regul Ho-meost Agents. 2019 May-Jun;33(3 Suppl. 1):35-41.
7. Emami E, Taraf H, de Grandmont P, Gauthier G, de Koninck L, Lamarche C, de Souza RF. The association of denture stomatitis and partial removable dental prostheses: a systematic review. Int J Prosthodont. 2012 Mar-Apr; 25(2): 113-9.
8. Kansky AA, Didanovic V, Dovsak T, Brzak BL, Pelivan I, Terle-vic D. Epidemiology of oral mucosal lesions in Slovenia. Radiol Oncol. 2018 Sep 11;52(3):263-6. [DOI:10.2478/raon-2018-0031] [PMID] [PMCID]
9. Navabi N, Gholamhoseinian A, Baghaei B, Hashemipour MA. Risk factors associated with denture stomatitis in healthy sub-jects attending a dental school in southeast iran. Sultan Qaboos Univ Med J. 2013 Nov;13(4):574-80. [DOI:10.12816/0003318] [PMID] [PMCID]
10. Aoun G, Cassia A. Evaluation of Denture-related Factors Predisposing to Denture Stomatitis in a Lebanese Population. Mater Sociomed. 2016 Oct;28(5):392-6. [DOI:10.5455/msm.2016.28.392-396] [PMID] [PMCID]
11. Matsumoto MA, Castanho J, Kawakami RY, Ribeiro DA. Cyto-genetical damage in exfoliated oral mucosa cells in elderly people suffering denture stomatitis. Gerodontology. 2010 Sep;27(3):183-8. [DOI:10.1111/j.1741-2358.2009.00315.x] [PMID]
12. Casaroto AR, Lara VS. Phytomedicines for Candida-associated denture stomatitis. Fitoterapia. 2010 Jul; 81(5): 323-8. [DOI:10.1016/j.fitote.2009.12.003] [PMID]
13. Emami E, Kabawat M, Rompre PH, Feine JS. Linking evidence to treatment for denture stomatitis: a meta-analysis of randomized controlled trials. J Dent. 2014 Feb; 42 (2):99-106. [DOI:10.1016/j.jdent.2013.11.021] [PMID]
14. Jose A, Coco BJ, Milligan S, Young B, Lappin DF, Bagg J, Murray C, Ramage G. Reducing the incidence of denture stomatitis: are denture cleansers sufficient? J Prosthodont. 2010 Jun;19(4):252-7. [DOI:10.1111/j.1532-849X.2009.00561.x] [PMID]
15. Alajbeg I, Challacombe SJ, Holmstrup P, Jontell M. Red and White Lesions of the Oral Mucosa. Burket's Oral Medicine. 13th ed. Hoboken, NJ, USA: Wiley-Blackwell; 2021: 92-3. [DOI:10.1002/9781119597797.ch4]
16. Yano J, Yu A, Fidel PL Jr, Noverr MC. Candida glabrata Has No Enhancing Role in the Pathogenesis of Candida-Associated Den-ture Stomatitis in a Rat Model. mSphere. 2019 Apr 3;4(2):e00191-19. [DOI:10.1128/mSphere.00191-19] [PMID] [PMCID]
17. Altarawneh S, Bencharit S, Mendoza L, Curran A, Barrow D, Barros S, Preisser J, Loewy ZG, Gendreau L, Offenbacher S. Clini-cal and histological findings of denture stomatitis as related to intraoral colonization patterns of Candida albicans, salivary flow, and dry mouth. J Prosthodont. 2013 Jan;22(1):13-22. [DOI:10.1111/j.1532-849X.2012.00906.x] [PMID] [PMCID]
18. Navabi N, Nakhaee N, Mirzadeh A. Validation of a Persian Version of the Oral Health Impact Profile (OHIP-14). Iran J Pub-lic Health. 2010;39(4):135-9.
19. Habibagahi R, Navabi N, Alsadat Hashemipour M, Hashemzehi A. Does Smoking Cessation Improve Oral Health-related Quality of Life? A Pilot Study. Addict Health 2020; 12(3): 167-74.
20. Nassab ARG, Navabi N, Pour MM, Charrosta N, Hashemipour MA. Quality of life in patients with chronic oral mucosal conditions: a qualitative research. Pesqui Bras Odon-topediatria Clín Integr. 2021; 21:e0092. [DOI:10.1590/pboci.2021.018]
21. Farhang M, Navabi N, Kakoie S, Hashemipour MA. Evaluating the life quality of patients with diseases of oral mu-cosa referred to Kerman Dental School, Kerman, Iran, in 2014-2015. J Oral Health Oral Epidemiol. 2017; 6(3): 151-8.
22. Kürklü-Gürleyen E, Öğüt-Erişen M, Çakır O, Uysal Ö, Ak G. Quality of life in patients with recurrent aphthous stomatitis treated with a mucoadhesive patch containing citrus essential oil. Patient Prefer Adherence. 2016 May 27;10:967-73. [DOI:10.2147/PPA.S106530] [PMID] [PMCID]
23. Nagao Y, Sata M. Effect of oral care gel on the quality of life for oral lichen planus in patients with chronic HCV infection. Virol J. 2011 Jul 12;8:348. [DOI:10.1186/1743-422X-8-348] [PMID] [PMCID]
24. Anadioti E, Gates WD 3rd, Elpers J, De Kok IJ, Cooper LF. Retrospective cohort analysis of maxillary overdentures re-tained by unsplinted implants. J Prosthet Dent. 2019 Sep; 122(3):301-8.e1. [DOI:10.1016/j.prosdent.2018.10.014] [PMID]
25. Mendes MSS, Chester LN, Fernandes Dos Santos JF, Chen X, Caplan DJ, Marchini L. Self-perceived oral health among institu-tionalized older adults in Taubate, Brazil. Spec Care Dentist. 2020 Jan;40(1):49-54. [DOI:10.1111/scd.12430] [PMID]
26. Gauch LMR, Pedrosa SS, Silveira-Gomes F, Esteves RA, Marques-da-Silva SH. Isolation of Candida spp. from denture-related stomatitis in Pará, Brazil. Braz J Microbiol. 2018 Jan-Mar;49(1):148-51. [DOI:10.1016/j.bjm.2017.07.001] [PMID] [PMCID]
27. Uludamar A, Evren BA, Işeri U, Özkan YK. Oral health status and treatment requirements of different residential homes in Istanbul: a comparative study. Arch Gerontol Geriatr. 2011 Jul-Aug;53(1):e67-74. [DOI:10.1016/j.archger.2010.10.029] [PMID]
28. Mandali G, Sener ID, Turker SB, Ulgen H. Factors affecting the distribution and prevalence of oral mucosal lesions in complete denture wearers. Gerodontology. 2011 Jun;28(2):97-103. [DOI:10.1111/j.1741-2358.2009.00351.x] [PMID]
29. Yarborough A, Cooper L, Duqum I, Mendonça G, McGraw K, Stoner L. Evidence Regarding the Treatment of Denture Stomati-tis. J Prosthodont. 2016 Jun;25(4):288-301. [DOI:10.1111/jopr.12454] [PMID]
30. Sutula J, Coulthwaite L, Thomas L, Verran J. The effect of a commercial probiotic drink on oral microbiota in healthy complete denture wearers. Microb Ecol Health Dis. 2012 Oct 3;23. [DOI:10.3402/mehd.v23i0.18404] [PMID] [PMCID]
31. Mahdavi Omran S, Rezaei Dastjerdi M, Zuashkiani M, Moqarabzadeh V, Taghizadeh-Armaki M. In Vitro Antifungal Susceptibility of Candida Species Isolated from Iranian Patients with Denture Stomatitis. Biomed Res Int. 2018 May 16;2018:3086586. [DOI:10.1155/2018/3086586] [PMID] [PMCID]
32. Batisse C, Bonnet G, Veyrune JL, Nicolas E, Bessadet M. Pre-dictive Parameters of Oral Health Quality of Life in Complete Mandibular Denture Wearers Stabilized by Mini-Implants: A Two-Year Follow-Up Study. Materials (Basel). 2017 Oct 19;10(10):1197. [DOI:10.3390/ma10101197] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |