Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 79-87 |
Back to browse issues page


Ethics code: IR.KMU.REC.1395.529
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hosseini B, Malekmohammadi T, Naderi T, Bakhtiary M, Hosseini Dastnaei P, Mafi S. Oral and Dental Health Status of Pregnant Women Referred to Perinatal Clinics in Southeastern Iran. J Res Dent Maxillofac Sci 2023; 8 (2) :79-87
URL: http://jrdms.dentaliau.ac.ir/article-1-413-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-413-en.html
Bahareh Hosseini1 

 , Tayebeh Malekmohammadi2 , Tayebeh Naderi3 , Maryam Bakhtiary4 , Peimaneh Hosseini Dastnaei5 , Sahar Mafi *6
, Tayebeh Malekmohammadi2 , Tayebeh Naderi3 , Maryam Bakhtiary4 , Peimaneh Hosseini Dastnaei5 , Sahar Mafi *6
, Tayebeh Malekmohammadi2 , Tayebeh Naderi3 , Maryam Bakhtiary4 , Peimaneh Hosseini Dastnaei5 , Sahar Mafi *6
1- Endodontology Research Center, Ker-man University of Medical Sciences, Kerman, Iran
2- Social Determinants of Health Research Center, Department of Dental Public Health, School of Dentistry, Kerman University of Medical Sciences, Kerman, Iran
3- Department of Obstetrics and Gynecology, Kerman University of Medical Sciences, Kerman, Iran
4- Private Dentistry Practice, Kerman, Iran
5- Private Dentistry Practice, Isfahan, Iran
6- Department of Oral Medicine, School of Dentistry, Kermanshah, Iran ,Sahar.mafi86@gmail.com
2- Social Determinants of Health Research Center, Department of Dental Public Health, School of Dentistry, Kerman University of Medical Sciences, Kerman, Iran
3- Department of Obstetrics and Gynecology, Kerman University of Medical Sciences, Kerman, Iran
4- Private Dentistry Practice, Kerman, Iran
5- Private Dentistry Practice, Isfahan, Iran
6- Department of Oral Medicine, School of Dentistry, Kermanshah, Iran ,
Full-Text [PDF 737 kb]
(1155 Downloads)
| Abstract (HTML) (2974 Views)
Background and Aim: As maternal periodontal disease can increase the risk of preterm birth and low birth weight, this study aimed to investigate the oral health status of pregnant women considering the circumstances during pregnancy and the necessity to keep the mother and baby healthy.
Materials and Methods: This cross-sectional study was conducted on 200 pregnant women referred to perinatal clinics in Kerman city. The participants’ oral health behavior, decayed, missing, and filled teeth (DMFT) score, plaque index (PI) and community periodontal index (CPI) were assessed. Data were analyzed by the Chi-square test and multivariate linear regression model.
Results: Of all, 39.5% had dental problems during pregnancy. Only 5.4% of them presented to a dentist. The participants’ concerns regarding the risks of dental procedures during pregnancy was the most common reason for not seeking dental treatment. The mean PI and DMFT were 0.75±0.48 and 11.29±3.88, respectively. Multivariate analysis showed that the DMFT index score had a significant correlation with age (P=0.001) and educational level (P=0.03). The CPI and gestational age (in weeks) were also significantly correlated (P=0.005).
Conclusion: Due to poor oral health of pregnant women, healthcare planners should provide inter-professional, community-based, and preventive oral health interventions before and during pregnancy.
Key Words: Oral Health; Pregnancy; Pregnant Women
Introduction
Currently, achieving and maintaining excellent oral and dental health during pregnancy is an essential factor with immediate and long-term effects on maternal and child’s health [1]. High levels of estrogen and progesterone increase the levels of inflammatory mediators and immune responses [2]. Along with these hormonal changes, possible changes in oral and dental hygiene habits, lifestyle, and mothers' nutrition during pregnancy predispose them to a higher risk of periodontal disease [3, 4]. A relationship has been shown between periodontal disease and premature birth and low birth weight [5]. On the other hand, recent studies declared that reducing the mothers’ oral Streptococcus count decreased the risk of contamination and early childhood caries in babies [6-8]. A direct relationship has been found between the mothers' oral health status and their quality of life during and after pregnancy [2, 9, 10].
Therefore, special conditions during pregnancy necessitate better oral healthcare during this period, and failure to pay attention to this matter may cause oral and dental problems and compromise the mother's general health and subsequently the baby’s health. One reason for this negligence is that dental practitioners, physicians, gynecologists, and mothers either do not have sufficient knowledge or do not pay enough attention to dental treatments during pregnancy. Another reason may be social or financial problems of the parents [4,7,8,11-14]. Studies in
developed and developing countries show that less than half of pregnant women are examined by a dentist during pregnancy [15, 16].
Researchers in different parts of the world have conducted epidemiological studies to assess the oral and dental health status of pregnant women so that the results can be used for large-scale planning in the field of prevention and treatment [11, 17-19].
To the best of the authors’ knowledge, there is no recent study conducted on oral and dental health status of pregnant women in southeast Iran conducted in the past 15 years. The population of pregnant women and their economic situation have drastically changed since then, which highlights the need for further investigations in this regard. This study aimed to investigate the oral health status of pregnant women referred to perinatal clinics in Kerman city in the southeast Iran.
Materials and Methods
In this descriptive cross-sectional study, 200 pregnant women referred to perinatal clinics (Afzalipour Obstetrics and Gynecology Hospital and several private clinics) in Kerman, Iran in 2017 were selected by simple random sampling. The sample size was calculated based on previous studies [3,4] using the sample size calculation formula (Z=1.96, P=0.25, Q=0.75, D=0.06, N=P*Q*Z*Z/D*D). The Research Ethics Committee of Kerman University of Medical Sciences approved this study (IR.KMU.REC.1395.529).
The inclusion criteria were signing informed consent forms, voluntary participation in the study, and not wearing a denture. Uncontrolled systemic diseases, history of periodontal disease, and severe gag reflex were the exclusion criteria.
A researcher-made questionnaire was used to collect the data. Seven oral medicine specialists verified the validity of the questionnaire, and its content validity index was found to be favorable (>0.78). The intraclass correlation coefficient was high (0.84) as confirmed by the test-retest reliability assessment.
The questionnaire had 19 questions and three charts. The first part of the questionnaire asked for the participants’ name, age, educational level, order of pregnancy, gestational age in weeks, and stage of pregnancy. The following questions were also asked: previous pregnancies (such as history of miscarriage, C-section or preterm delivery), history of diseases (cardiac, pulmonary, digestive system, renal, mental or other types of diseases) and the medications used by the participants. Pregnant women were asked to self-evaluate their oral health status. The remaining questions were about the women’s oral health behaviors, history of having dental problems and visiting a dentist, receipt of dental treatments, and referral to a dentist by a midwife or obstetrician before or during pregnancy. They were also asked about the prescribed medications during pregnancy for dental problems, the women’s concerns about receiving dental treatments during pregnancy, and whether their pregnancy was planned or not. Three charts at the end of the questionnaire were used to assess the community periodontal index (CPI), plaque index (PI) and decayed, missing, and filled teeth (DMFT) index of the participants.
All indices were recorded by a trained dental student after obtaining the required calibration score with a trainee (dental public health specialist). Dental examinations were performed on a chair under a headlight using a flat dental mirror and a CPI-probe (or WHO-probe that has a black band from 3.5 to 5.5 mm, and two black rings at 8.5 and 11.5 mm form its round ball shape tip) [20]. To calculate the CPI, periodontal conditions including gingival bleeding, subgingival calculus, and depth of periodontal pockets were evaluated in teeth #16-17, 11, 26-27, 36-37, 31 and 46-47. According to the CPI criteria, each patient received a code from 0 to 4 (code 0: healthy periodontium; code 1: gingival bleeding on probing; code 2: calculus and bleeding; code 3: periodontal pocket by 4-5 mm; and code 4: periodontal pocket ≥ 6 mm) [20]. For each tooth, the biggest number was considered and the frequency of each code in all participants was reported.
According to the World Health Organization, for DMFT Index, dental examinations were performed visually for carious, filled, and missing teeth [20]. If a filled tooth had caries, it was classified as a decayed tooth. The DMFT score for each tooth ranged from 0 to 6 (code 0: sound tooth 1, code 1: decayed tooth, code 2: filled tooth with recurrent caries, code 3: filled tooth with no caries, code 4: missed tooth due to caries, code 5: missed tooth due to other reasons, code 6: unerupted tooth). For DMFT index score, all codes for each participant were summed and divided by the number of teeth. The Silness and Loe standard index and visual examination were used to evaluate the presence of dental plaque [20]. PI was calculated for teeth #12, 16, 24, 32, 36, and 44. The PI for each tooth ranged from 0 to 3 (code 0: no observable plaque, code 1: a thin film of plaque is detected at the gingival margin by running a probe or explorer across the tooth surfaces, code 2: a moderate amount of plaque is detected along the gingival margin and plaque is visible clinically, code 3: heavy plaque accumulation is detected at the gingival margin and in interdental spaces. All codes for each participant were summed and divided by the number of assessed teeth. If the overall score was zero, oral hygiene was excellent. If it was 0.1- 0.9, 1-1.9, and 2-3 it was considered as good, moderate, and poor oral hygiene, respectively.
In addition to descriptive statistics (frequency, percentage, mean, and standard deviation), the Pearson's correlation coefficient was applied to analyze the relationship of DMFT and dental PI with gestational age in weeks. The Spearman’s correlation coefficient was used to assess the relationship of CPI and gestational age in weeks. The Chi-square test was applied to analyze the correlation of CPI with current pregnancy order, educational level, and underlying diseases. The multivariate linear regression was used to analyze the cumulative effect of the variables. The level of significance was set at 0.05.
Results
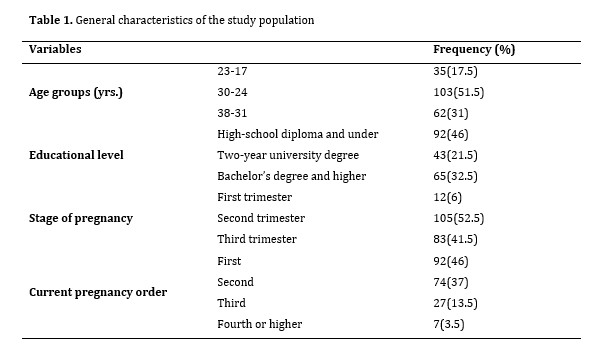
A total of 200 pregnant women participated in this study with an age range of 17-38 years (mean age of 27.93±4.64 years), and gestational age of 9–41 weeks (mean of 26.85±6.89 weeks). Table 1 shows the demographic characteristics of the participants.
Thirty-five participants (17.5%) had a history of systemic conditions. Twenty-eight (14%) pregnant women took medications during pregnancy, and the most commonly used medication was levothyroxine, followed by insulin.
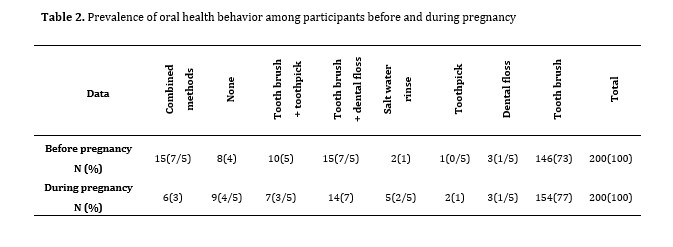
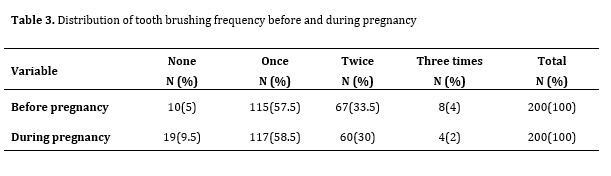
Nineteen participants (9.5%) had a history of abortion, and 4 (2%) of them had experienced premature delivery (childbirth before the 37th week of gestational age). Oral health self-assessment showed that 43.5% of pregnant women believed that their oral health status was moderate. Pregnant women's oral health behaviors before and during pregnancy including toothbrushing, and using dental floss, toothpicks, mouthwashes, and saline solution are shown in Tables 2 and 3. Figure 1 shows all dental treatments that participants received during pregnancy.
Discussion
Higher risk for gingival and periodontal disease and dental caries due to hormonal changes and nutritional and hygienic habits during pregnancy can cause premature birth and low birthweight as short-term effects [5]. The long-term effects like transmission of Streptococcus mutans from mother to baby can lead to a higher rate of dental caries in children [6-8, 21]. On the other hand, oral health in pregnant women has an established relationship with the mothers' quality of life [2, 9, 10]. Mothers also have a unique role in hygienic habits of other family members, especially children, indicating their significant role in promoting the community's oral health [21].
Nevertheless, worldwide studies have shown unfavorable oral health status of pregnant women [4, 18, 19, 22-26].
Investigating the oral health status of pregnant women in this study showed that the mean of DMFT index was high. The most frequent component of the DMFT index was the D component, and it exhibited a significant relationship with age and educational level of mothers. The pregnant women with lower educational levels had the highest mean DMFT. The results also indicated that only a little more than one-fourth of pregnant women were periodontally healthy.
The mean DMFT score and the PI of 340 pregnant women in Arak, Iran, in 2011 were reported to be 5.4±2.83 and 76%, respectively, in a study by Shamsi et al. which was in agreement with the present findings [22].
The present results indicated that oral health behaviors of pregnant women in Kerman were not favorable; in this context, most of them only brushed their teeth once daily during this period, although they needed to brush their teeth more frequently. Comparing these results with similar studies in developing countries showed that insufficient attention to oral hygiene during pregnancy is a common problem [18]. The situation seems to be more favorable in developed countries; according to some studies, most pregnant women brush their teeth two or three times a day, and the oral health indices are better in these countries [11, 19].
In the present study, 76.5% of the women had a history of dental procedures before pregnancy. The obstetrician or midwives had referred only 1.5% of 63.5% of the participants with pre-planned pregnancy to a dentist for dental examinations and dental treatments.
A study by Odermatt et al. on pregnant and non-pregnant women (control group) in Switzerland in 2017 indicated that the target group had a significantly higher knowledge level about the importance of oral and dental health during pregnancy than the control group. This study also found that an obstetrician informed only one out of four pregnant women (25%) about the importance of periodic dental examinations during pregnancy. Odermatt et al. reported that providing pregnant women with inadequate information by obstetricians is due to insufficient knowledge of obstetricians about periodontal disease [17]. A national survey by Byrd et al. in the United States in 2018 declared that two-thirds of the primary care physicians instructed pregnant women about the importance of oral health during pregnancy and encouraged them to have periodic dental examinations [14].
Another study on 3,455 pregnant women in 2018 showed that 17.6% of them were referred to a dentist by an obstetrician.
Follow-ups and dental procedures in these pregnant women were significantly more common than in those presenting to the dentist without a referral by an obstetrician. This study emphasized on the importance of oral and dental healthcare in this period and the necessity of increasing the obstetricians' involvement in the referral process [27].
In the current study, 79 participants (39.5%) developed oral and dental problems during pregnancy. They did not have a positive attitude towards dental visits, and only 12 women (15.2%) had visited a dentist while only 9 out of 12 had been referred to a dentist by their obstetrician or midwife.
The results of the present study indicated lack of attention of healthcare providers such as midwives and obstetricians to oral health during pregnancy and referral of pregnant women for dental examinations and treatments before and during pregnancy. Therefore, it is necessary to educate obstetricians, midwives, and family physicians about the importance of oral health and the problems that pregnant women may face during pregnancy. On the other hand, attention should be paid to cooperation between theses healthcare providers and dentists.
In the present study, obstetricians and midwives referred only 9 participants (4.5%) to dentists for dental examinations and dental treatments. Considering the small number of referrals, it appears that along with other barriers in referring pregnant women to dentists during pregnancy, healthcare providers did not place sufficient emphasis on this matter because of concerns about the consequences of dental procedures during pregnancy [13].
In line with these findings, Al-Habashneh et al. showed that 88% of physicians recommended pregnant women to postpone oral and dental treatments to the postpartum period. In their study, only 54% of participates believed that dental problems could affect pregnancy outcomes [28].
Other recent studies declared misunderstandings about the safety of dental procedures during pregnancy among healthcare providers and dentists. While, even radiography and extraction can be carried out during this period without any specific problems [24, 26, 27, 29].
As mentioned earlier, 79 participants suffered from oral and dental problems during pregnancy, and 61 of them (77.2%) did not visit a dentist to address their oral and dental issues because they were worried about the consequences of dental treatments. They believed that these procedures might be harmful for the baby. In some studies, poor maternal health awareness was addressed as one of the reasons for this belief. They suggested that healthcare providers should enhance the mothers' knowledge to change their attitude [1, 11, 17, 29]. In addition, due to multiple barriers to deliver dental services to pregnant women, researchers suggest some solutions such as reformed insurance policy, equality in distributing health resources and services, and cost-effective population-level interventions [30].
Conclusion
The results of this study showed that oral health status in pregnant women in Kerman was not favorable. It seems necessary to inform women of childbearing age and expectant mothers about the importance of oral health, how to maintain oral health, and treatments that can be done during pregnancy. Therefore, the national health policymakers should develop programs to educate women and refer them to dentists through health service providers, midwives and obstetricians and monitor their effective implementation.
Acknowledgments
This study was supported by the Oral and Dental Diseases Research Center, Kerman University of Medical Sciences, Kerman, Iran. We would like to appreciate our colleagues in the Oral Medicine Department of Dental School of Kerman University of Medical Sciences for their cooperation. The patients who participated in this study are also appreciated.
Full-Text: (1378 Views)
Abstract
Background and Aim: As maternal periodontal disease can increase the risk of preterm birth and low birth weight, this study aimed to investigate the oral health status of pregnant women considering the circumstances during pregnancy and the necessity to keep the mother and baby healthy.
Materials and Methods: This cross-sectional study was conducted on 200 pregnant women referred to perinatal clinics in Kerman city. The participants’ oral health behavior, decayed, missing, and filled teeth (DMFT) score, plaque index (PI) and community periodontal index (CPI) were assessed. Data were analyzed by the Chi-square test and multivariate linear regression model.
Results: Of all, 39.5% had dental problems during pregnancy. Only 5.4% of them presented to a dentist. The participants’ concerns regarding the risks of dental procedures during pregnancy was the most common reason for not seeking dental treatment. The mean PI and DMFT were 0.75±0.48 and 11.29±3.88, respectively. Multivariate analysis showed that the DMFT index score had a significant correlation with age (P=0.001) and educational level (P=0.03). The CPI and gestational age (in weeks) were also significantly correlated (P=0.005).
Conclusion: Due to poor oral health of pregnant women, healthcare planners should provide inter-professional, community-based, and preventive oral health interventions before and during pregnancy.
Key Words: Oral Health; Pregnancy; Pregnant Women
Introduction
Currently, achieving and maintaining excellent oral and dental health during pregnancy is an essential factor with immediate and long-term effects on maternal and child’s health [1]. High levels of estrogen and progesterone increase the levels of inflammatory mediators and immune responses [2]. Along with these hormonal changes, possible changes in oral and dental hygiene habits, lifestyle, and mothers' nutrition during pregnancy predispose them to a higher risk of periodontal disease [3, 4]. A relationship has been shown between periodontal disease and premature birth and low birth weight [5]. On the other hand, recent studies declared that reducing the mothers’ oral Streptococcus count decreased the risk of contamination and early childhood caries in babies [6-8]. A direct relationship has been found between the mothers' oral health status and their quality of life during and after pregnancy [2, 9, 10].
Therefore, special conditions during pregnancy necessitate better oral healthcare during this period, and failure to pay attention to this matter may cause oral and dental problems and compromise the mother's general health and subsequently the baby’s health. One reason for this negligence is that dental practitioners, physicians, gynecologists, and mothers either do not have sufficient knowledge or do not pay enough attention to dental treatments during pregnancy. Another reason may be social or financial problems of the parents [4,7,8,11-14]. Studies in
developed and developing countries show that less than half of pregnant women are examined by a dentist during pregnancy [15, 16].
Researchers in different parts of the world have conducted epidemiological studies to assess the oral and dental health status of pregnant women so that the results can be used for large-scale planning in the field of prevention and treatment [11, 17-19].
To the best of the authors’ knowledge, there is no recent study conducted on oral and dental health status of pregnant women in southeast Iran conducted in the past 15 years. The population of pregnant women and their economic situation have drastically changed since then, which highlights the need for further investigations in this regard. This study aimed to investigate the oral health status of pregnant women referred to perinatal clinics in Kerman city in the southeast Iran.
Materials and Methods
In this descriptive cross-sectional study, 200 pregnant women referred to perinatal clinics (Afzalipour Obstetrics and Gynecology Hospital and several private clinics) in Kerman, Iran in 2017 were selected by simple random sampling. The sample size was calculated based on previous studies [3,4] using the sample size calculation formula (Z=1.96, P=0.25, Q=0.75, D=0.06, N=P*Q*Z*Z/D*D). The Research Ethics Committee of Kerman University of Medical Sciences approved this study (IR.KMU.REC.1395.529).
The inclusion criteria were signing informed consent forms, voluntary participation in the study, and not wearing a denture. Uncontrolled systemic diseases, history of periodontal disease, and severe gag reflex were the exclusion criteria.
A researcher-made questionnaire was used to collect the data. Seven oral medicine specialists verified the validity of the questionnaire, and its content validity index was found to be favorable (>0.78). The intraclass correlation coefficient was high (0.84) as confirmed by the test-retest reliability assessment.
The questionnaire had 19 questions and three charts. The first part of the questionnaire asked for the participants’ name, age, educational level, order of pregnancy, gestational age in weeks, and stage of pregnancy. The following questions were also asked: previous pregnancies (such as history of miscarriage, C-section or preterm delivery), history of diseases (cardiac, pulmonary, digestive system, renal, mental or other types of diseases) and the medications used by the participants. Pregnant women were asked to self-evaluate their oral health status. The remaining questions were about the women’s oral health behaviors, history of having dental problems and visiting a dentist, receipt of dental treatments, and referral to a dentist by a midwife or obstetrician before or during pregnancy. They were also asked about the prescribed medications during pregnancy for dental problems, the women’s concerns about receiving dental treatments during pregnancy, and whether their pregnancy was planned or not. Three charts at the end of the questionnaire were used to assess the community periodontal index (CPI), plaque index (PI) and decayed, missing, and filled teeth (DMFT) index of the participants.
All indices were recorded by a trained dental student after obtaining the required calibration score with a trainee (dental public health specialist). Dental examinations were performed on a chair under a headlight using a flat dental mirror and a CPI-probe (or WHO-probe that has a black band from 3.5 to 5.5 mm, and two black rings at 8.5 and 11.5 mm form its round ball shape tip) [20]. To calculate the CPI, periodontal conditions including gingival bleeding, subgingival calculus, and depth of periodontal pockets were evaluated in teeth #16-17, 11, 26-27, 36-37, 31 and 46-47. According to the CPI criteria, each patient received a code from 0 to 4 (code 0: healthy periodontium; code 1: gingival bleeding on probing; code 2: calculus and bleeding; code 3: periodontal pocket by 4-5 mm; and code 4: periodontal pocket ≥ 6 mm) [20]. For each tooth, the biggest number was considered and the frequency of each code in all participants was reported.
According to the World Health Organization, for DMFT Index, dental examinations were performed visually for carious, filled, and missing teeth [20]. If a filled tooth had caries, it was classified as a decayed tooth. The DMFT score for each tooth ranged from 0 to 6 (code 0: sound tooth 1, code 1: decayed tooth, code 2: filled tooth with recurrent caries, code 3: filled tooth with no caries, code 4: missed tooth due to caries, code 5: missed tooth due to other reasons, code 6: unerupted tooth). For DMFT index score, all codes for each participant were summed and divided by the number of teeth. The Silness and Loe standard index and visual examination were used to evaluate the presence of dental plaque [20]. PI was calculated for teeth #12, 16, 24, 32, 36, and 44. The PI for each tooth ranged from 0 to 3 (code 0: no observable plaque, code 1: a thin film of plaque is detected at the gingival margin by running a probe or explorer across the tooth surfaces, code 2: a moderate amount of plaque is detected along the gingival margin and plaque is visible clinically, code 3: heavy plaque accumulation is detected at the gingival margin and in interdental spaces. All codes for each participant were summed and divided by the number of assessed teeth. If the overall score was zero, oral hygiene was excellent. If it was 0.1- 0.9, 1-1.9, and 2-3 it was considered as good, moderate, and poor oral hygiene, respectively.
In addition to descriptive statistics (frequency, percentage, mean, and standard deviation), the Pearson's correlation coefficient was applied to analyze the relationship of DMFT and dental PI with gestational age in weeks. The Spearman’s correlation coefficient was used to assess the relationship of CPI and gestational age in weeks. The Chi-square test was applied to analyze the correlation of CPI with current pregnancy order, educational level, and underlying diseases. The multivariate linear regression was used to analyze the cumulative effect of the variables. The level of significance was set at 0.05.
Results
A total of 200 pregnant women participated in this study with an age range of 17-38 years (mean age of 27.93±4.64 years), and gestational age of 9–41 weeks (mean of 26.85±6.89 weeks). Table 1 shows the demographic characteristics of the participants.
Thirty-five participants (17.5%) had a history of systemic conditions. Twenty-eight (14%) pregnant women took medications during pregnancy, and the most commonly used medication was levothyroxine, followed by insulin.
Nineteen participants (9.5%) had a history of abortion, and 4 (2%) of them had experienced premature delivery (childbirth before the 37th week of gestational age). Oral health self-assessment showed that 43.5% of pregnant women believed that their oral health status was moderate. Pregnant women's oral health behaviors before and during pregnancy including toothbrushing, and using dental floss, toothpicks, mouthwashes, and saline solution are shown in Tables 2 and 3. Figure 1 shows all dental treatments that participants received during pregnancy.
Table 1. General characteristics of the study population
About 153 (76.5%) pregnant mothers had a history of dental procedures such as restorative treatments, periodontal treatment, root canal therapy, tooth extraction, and dental surgery, before pregnancy.
A total of 127 participants (63.5%) had planned their pregnancy. Only three pregnant women (1.5%) confirmed that they had been referred for dental examination before pregnancy by their gynecologist. During pregnancy, 79 women (39.5%) suffered from oral and dental problems and pain, and the rest had no problems. Twelve (15/2%) women with oral and dental problems had visited a dentist, but only 9 (5.4%) of them had been referred to a dentist by their obstetrician or midwife.
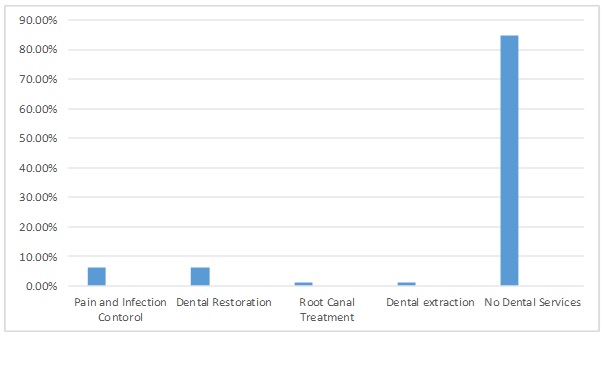
Of those visiting a dentist, 5 (6.3%) received medications for pain and infection control (three received analgesics, one received antibiotics, and one received both); 5 (6.3%) underwent restorative procedures, 1 (1.2%) had root canal therapy, and 1 (1.2%) underwent tooth extraction (Figure 1).
In participants with oral and dental problems during pregnancy, 61 (77.2%) pregnant women did not seek dental treatment due to their concerns about dental procedures during pregnancy.
The PI ranged from 0 to 2.5 (0.75±0.48). PI was not significantly correlated with any of the variables such as age, education level, gestational age in weeks, current pregnancy order, and underlying conditions (P>0.05).
The CPI index ranged from 0–4, and the highest frequency belonged to bleeding on probing (42.5%). CPI showed a significant correlation with gestational age in weeks (P=0.005).
The DMFT index ranged from 0–21 (11.29±3.88). The highest value was related to decayed teeth (D) (9.46±3.41), while the mean and standard error for the teeth lost due to caries (M) and filled teeth (F) were 1.8±0.18 and 3.18±2.35, respectively.
Multivariate analysis showed that the DMFT index had a significant correlation with age (P=0.001) and educational level (P=0.03). The highest mean DMFT was recorded in participants with older age and lower educational level.
{kind=link}
About 153 (76.5%) pregnant mothers had a history of dental procedures such as restorative treatments, periodontal treatment, root canal therapy, tooth extraction, and dental surgery, before pregnancy.
A total of 127 participants (63.5%) had planned their pregnancy. Only three pregnant women (1.5%) confirmed that they had been referred for dental examination before pregnancy by their gynecologist. During pregnancy, 79 women (39.5%) suffered from oral and dental problems and pain, and the rest had no problems. Twelve (15/2%) women with oral and dental problems had visited a dentist, but only 9 (5.4%) of them had been referred to a dentist by their obstetrician or midwife.
Of those visiting a dentist, 5 (6.3%) received medications for pain and infection control (three received analgesics, one received antibiotics, and one received both); 5 (6.3%) underwent restorative procedures, 1 (1.2%) had root canal therapy, and 1 (1.2%) underwent tooth extraction (Figure 1).
In participants with oral and dental problems during pregnancy, 61 (77.2%) pregnant women did not seek dental treatment due to their concerns about dental procedures during pregnancy.
The PI ranged from 0 to 2.5 (0.75±0.48). PI was not significantly correlated with any of the variables such as age, education level, gestational age in weeks, current pregnancy order, and underlying conditions (P>0.05).
The CPI index ranged from 0–4, and the highest frequency belonged to bleeding on probing (42.5%). CPI showed a significant correlation with gestational age in weeks (P=0.005).
The DMFT index ranged from 0–21 (11.29±3.88). The highest value was related to decayed teeth (D) (9.46±3.41), while the mean and standard error for the teeth lost due to caries (M) and filled teeth (F) were 1.8±0.18 and 3.18±2.35, respectively.
Multivariate analysis showed that the DMFT index had a significant correlation with age (P=0.001) and educational level (P=0.03). The highest mean DMFT was recorded in participants with older age and lower educational level.
{kind=link}
{kind=link}
{kind=link}
Discussion
Higher risk for gingival and periodontal disease and dental caries due to hormonal changes and nutritional and hygienic habits during pregnancy can cause premature birth and low birthweight as short-term effects [5]. The long-term effects like transmission of Streptococcus mutans from mother to baby can lead to a higher rate of dental caries in children [6-8, 21]. On the other hand, oral health in pregnant women has an established relationship with the mothers' quality of life [2, 9, 10]. Mothers also have a unique role in hygienic habits of other family members, especially children, indicating their significant role in promoting the community's oral health [21].
Nevertheless, worldwide studies have shown unfavorable oral health status of pregnant women [4, 18, 19, 22-26].
Investigating the oral health status of pregnant women in this study showed that the mean of DMFT index was high. The most frequent component of the DMFT index was the D component, and it exhibited a significant relationship with age and educational level of mothers. The pregnant women with lower educational levels had the highest mean DMFT. The results also indicated that only a little more than one-fourth of pregnant women were periodontally healthy.
The mean DMFT score and the PI of 340 pregnant women in Arak, Iran, in 2011 were reported to be 5.4±2.83 and 76%, respectively, in a study by Shamsi et al. which was in agreement with the present findings [22].
The present results indicated that oral health behaviors of pregnant women in Kerman were not favorable; in this context, most of them only brushed their teeth once daily during this period, although they needed to brush their teeth more frequently. Comparing these results with similar studies in developing countries showed that insufficient attention to oral hygiene during pregnancy is a common problem [18]. The situation seems to be more favorable in developed countries; according to some studies, most pregnant women brush their teeth two or three times a day, and the oral health indices are better in these countries [11, 19].
In the present study, 76.5% of the women had a history of dental procedures before pregnancy. The obstetrician or midwives had referred only 1.5% of 63.5% of the participants with pre-planned pregnancy to a dentist for dental examinations and dental treatments.
A study by Odermatt et al. on pregnant and non-pregnant women (control group) in Switzerland in 2017 indicated that the target group had a significantly higher knowledge level about the importance of oral and dental health during pregnancy than the control group. This study also found that an obstetrician informed only one out of four pregnant women (25%) about the importance of periodic dental examinations during pregnancy. Odermatt et al. reported that providing pregnant women with inadequate information by obstetricians is due to insufficient knowledge of obstetricians about periodontal disease [17]. A national survey by Byrd et al. in the United States in 2018 declared that two-thirds of the primary care physicians instructed pregnant women about the importance of oral health during pregnancy and encouraged them to have periodic dental examinations [14].
Another study on 3,455 pregnant women in 2018 showed that 17.6% of them were referred to a dentist by an obstetrician.
Follow-ups and dental procedures in these pregnant women were significantly more common than in those presenting to the dentist without a referral by an obstetrician. This study emphasized on the importance of oral and dental healthcare in this period and the necessity of increasing the obstetricians' involvement in the referral process [27].
In the current study, 79 participants (39.5%) developed oral and dental problems during pregnancy. They did not have a positive attitude towards dental visits, and only 12 women (15.2%) had visited a dentist while only 9 out of 12 had been referred to a dentist by their obstetrician or midwife.
The results of the present study indicated lack of attention of healthcare providers such as midwives and obstetricians to oral health during pregnancy and referral of pregnant women for dental examinations and treatments before and during pregnancy. Therefore, it is necessary to educate obstetricians, midwives, and family physicians about the importance of oral health and the problems that pregnant women may face during pregnancy. On the other hand, attention should be paid to cooperation between theses healthcare providers and dentists.
In the present study, obstetricians and midwives referred only 9 participants (4.5%) to dentists for dental examinations and dental treatments. Considering the small number of referrals, it appears that along with other barriers in referring pregnant women to dentists during pregnancy, healthcare providers did not place sufficient emphasis on this matter because of concerns about the consequences of dental procedures during pregnancy [13].
In line with these findings, Al-Habashneh et al. showed that 88% of physicians recommended pregnant women to postpone oral and dental treatments to the postpartum period. In their study, only 54% of participates believed that dental problems could affect pregnancy outcomes [28].
Other recent studies declared misunderstandings about the safety of dental procedures during pregnancy among healthcare providers and dentists. While, even radiography and extraction can be carried out during this period without any specific problems [24, 26, 27, 29].
As mentioned earlier, 79 participants suffered from oral and dental problems during pregnancy, and 61 of them (77.2%) did not visit a dentist to address their oral and dental issues because they were worried about the consequences of dental treatments. They believed that these procedures might be harmful for the baby. In some studies, poor maternal health awareness was addressed as one of the reasons for this belief. They suggested that healthcare providers should enhance the mothers' knowledge to change their attitude [1, 11, 17, 29]. In addition, due to multiple barriers to deliver dental services to pregnant women, researchers suggest some solutions such as reformed insurance policy, equality in distributing health resources and services, and cost-effective population-level interventions [30].
Conclusion
The results of this study showed that oral health status in pregnant women in Kerman was not favorable. It seems necessary to inform women of childbearing age and expectant mothers about the importance of oral health, how to maintain oral health, and treatments that can be done during pregnancy. Therefore, the national health policymakers should develop programs to educate women and refer them to dentists through health service providers, midwives and obstetricians and monitor their effective implementation.
Acknowledgments
This study was supported by the Oral and Dental Diseases Research Center, Kerman University of Medical Sciences, Kerman, Iran. We would like to appreciate our colleagues in the Oral Medicine Department of Dental School of Kerman University of Medical Sciences for their cooperation. The patients who participated in this study are also appreciated.
Type of Study: Original article |
Subject:
Oral medicine
References
1. Johnson M, George A, Dahlen H, Ajwani S, Bhole S, Blinkhorn A, Ellis S, Yeo A. The midwifery initiated oral health-dental service protocol: an intervention to improve oral health outcomes for pregnant women. BMC Oral Health. 2015 Jan 15;15:2. [DOI:10.1186/1472-6831-15-2] [PMID] [PMCID]
2. Musskopf ML, Milanesi FC, Rocha JMD, Fiorini T, Moreira CHC, Susin C, Rösing CK, Weidlich P, Oppermann RV. Oral health relat-ed quality of life among pregnant women: arandomized controlled trial. Braz Oral Res. 2018;32:e002. [DOI:10.1590/1807-3107bor-2018.vol32.0002]
3. Karem Hassan B, Jabbar Ali B, Mahmood Alwan A, Badeia RA. Self-Reported Oral Health Attitudes and Behaviors, and Gingival Status of Dental Students. Clin Cosmet Investig Dent. 2020 Jun 25;12:225-32. [DOI:10.2147/CCIDE.S249708] [PMID] [PMCID]
4. Suwargiani AA, Arief EM, Aripin D, Widyaputra S, Susilawati S. Oral health care practice of women with pregnancy experience. Padjadjaran Journal of Dentistry. 2020;32(3):197-206. [DOI:10.24198/pjd.vol32no3.30312]
5. Chambrone L, Pannuti CM, Guglielmetti MR, Chambrone LA. Evidence grade associating periodontitis with preterm birth and/or low birth weight: II: a systematic review of randomized trials evaluating the effects of periodontal treatment. J Clin Peri-odontol. 2011 Oct;38(10):902-14. [DOI:10.1111/j.1600-051X.2011.01761.x] [PMID]
6. Leong PM, Gussy MG, Barrow SY, de Silva-Sanigorski A, Wa-ters E. A systematic review of risk factors during first year of life for early childhood caries. Int J Paediatr Dent. 2013 Jul;23(4):235-50. [DOI:10.1111/j.1365-263X.2012.01260.x] [PMID]
7. Togoo RA, Al-Almai B, Al-Hamdi F, Huaylah SH, Althobati M, Alqarni S. Knowledge of Pregnant Women about Pregnancy Gingivitis and Children Oral Health. Eur J Dent. 2019 May;13(2):261-70. [DOI:10.1055/s-0039-1693236] [PMID] [PMCID]
8. Abdat M, Ramayana I. Relationship between mother's knowledge and behaviour with oral health status of early child-hood. Padjadjaran Journal of Dentistry. 2020;32(3): 166-73. [DOI:10.24198/pjd.vol32no2.24734]
9. Aguilar-Cordero MJ, Leon-Rios XA, Rivero-Blanco T, Rodriguez-Blanque R, Expósito-Ruiz M & Gil-Montoya JA. Quali-ty of life during pregnancy and its influence on oral health: a systematic review. J Oral Res 2019; 8(1):74-81. [DOI:10.17126/joralres.2019.011]
10. Gharehghani MAM, Bayani A, Bayat AH, Hemmat M, Karimy M, Ahounbar E, Armoon B, Fakhri Y, Schroth RJ. Poor oral health-related quality of life among pregnant women: A systematic review and meta-analysis. Int J Dent Hyg. 2021 Feb;19(1):39-49. [DOI:10.1111/idh.12465] [PMID]
11. Gaszyńska E, Klepacz-Szewczyk J, Trafalska E, Garus-Pakowska A, Szatko F. Dental awareness and oral health of pregnant women in Poland. Int J Occup Med Environ Health. 2015;28(3):603-11. [DOI:10.13075/ijomeh.1896.00183] [PMID]
12. Jackson JT, Quinonez RB, Kerns AK, Chuang A, Eidson RS, Boggess KA, Weintraub JA. Implementing a prenatal oral health program through interprofessional collaboration. J Dent Educ. 2015 Mar;79(3):241-8. [DOI:10.1002/j.0022-0337.2015.79.3.tb05878.x] [PMID]
13. Malek Mohammadi T, Malek Mohammadi M. Knowledge, attitude and practice of gynecologists and midwifes toward oral health in pregnant women in Kerman (2016).The Iranian Journal of Obstetrics, Gynecology and Infertility. 2017;20(4):9-18.
14. Byrd MG, Quinonez RB, Rozier RG, Phillips C, Mehegan M, Martinez L, Divaris K. Prenatal Oral Health Counseling by Prima-ry Care Physicians: Results of a National Survey. Matern Child Health J. 2018 Jul;22(7):1033-41. [DOI:10.1007/s10995-018-2483-4] [PMID]
15. Lydon-Rochelle MT, Krakowiak P, Hujoel PP, Peters RM. Dental care use and self-reported dental problems in relation to pregnancy. Am J Public Health. 2004 May;94(5):765-71. [DOI:10.2105/AJPH.94.5.765] [PMID] [PMCID]
16. George A, Dahlen HG, Blinkhorn A, Ajwani S, Bhole S, Ellis S, Yeo A, Elcombe E, Sadozai A, Johnson M. Measuring oral health during pregnancy: sensitivity and specificity of a maternal oral screening (MOS) tool. BMC Pregnancy Childbirth. 2016 Nov 9;16(1):347. [DOI:10.1186/s12884-016-1140-4] [PMID] [PMCID]
17. Odermatt T, Schötzau A, Hoesli I. Orale Gesundheit und Schwangerschaft - Patientinnenbefragung anhand eines Fragebogens [Oral Health and Pregnancy - Patient Survey using a Questionnaire]. Z Geburtshilfe Neonatol. 2017 Aug;221(4):180-6. [DOI:10.1055/s-0043-108762] [PMID]
18. Kateeb E. Palestinian women's oral health status, knowledge, practices, and access to dental care during pregnancy: a cross-sectional study. Lancet. 2018;391:S10. [DOI:10.1016/S0140-6736(18)30335-0]
19. Práger N, Kiss G, Orvos H, Novák T, Virág K, Gorzó I, Radnai M. Change in the Caries Status of Pregnant Women in Southeast Hungary and Its Background. Oral Health Prev Dent. 2018;16(2):137-43.
20. World Health Organization. Oral health surveys: basic methods. Available from: https://apps.who.int/iris/bitstream/handle/10665/97035/9789241548649_eng.pdf?sequence=1.
21. Bozorgmehr E, Hajizamani A, Malek Mohammadi T. Oral health behavior of parents as a predictor of oral health status of their children. ISRN Dent. 2013 May 8;2013: 741783. [DOI:10.1155/2013/741783] [PMID] [PMCID]
22. Shamsi M, Hidarnia A, Niknami S, Rafiee M, Karimi M. Oral health during pregnancy: A study from women with pregnancy. Dent Res J (Isfahan). 2013 May;10(3):409-10.
23. Elangovan GP, Muthu J, Periyasamy IK, Balu P, Kumar RS. Self-reported prenatal oral health-care practices of preterm low birth weight-delivered women belonging to different socioeco-nomic status: A postnatal survey. J Indian Soc Periodontol. 2017 Nov-Dec;21(6):489-93.
24. George A, Ajwani S, Bhole S, Dahlen HG, Reath J, Korda A, Ng Chok H, Miranda C, Villarosa A, Johnson M. Knowledge, attitude and practises of dentists towards oral health care during preg-nancy: A cross sectional survey in New South Wales, Australia. Aust Dent J. 2017 Sep;62(3):301-10. [DOI:10.1111/adj.12505] [PMID]
25. Deghatipour M, Ghorbani Z, Ghanbari S, Arshi S, Ehdayivand F, Namdari M, et al. Oral health status in relation to socioeconomic and behavioral factors among pregnant women: a community-based cross-sectional study. BMC Oral Health. 2019;19(1):1-10. [DOI:10.1186/s12903-019-0801-x] [PMID] [PMCID]
26. Thakur DV, Thakur DR, Kaur DM, Kaur DJ, Kumar DA, Virdi DD, Jassal DS. Pregnancy & Oral Health and Dental Management in Pregnant Patient. J Current Med Res Opinion . 2020;3(11):724-31. [DOI:10.15520/jcmro.v3i11.360]
27. Kobylińska A, Sochacki-Wójcicka N, Dacyna N, Trzaska M, Zawadzka A, Gozdowski D, Wielgoś M, Olczak-Kowalczyk D. The role of the gynaecologist in the promotion and maintenance of oral health during pregnancy. Ginekol Pol. 2018;89(3):120-4. [DOI:10.5603/GP.a2018.0021] [PMID]
28. Al-Habashneh R, Aljundi SH, Alwaeli HA. Survey of medical doctors' attitudes and knowledge of the association between oral health and pregnancy outcomes. Int J Dent Hyg. 2008 Aug;6(3):214-20. [DOI:10.1111/j.1601-5037.2008.00320.x] [PMID]
29. George A, Dahlen HG, Blinkhorn A, Ajwani S, Bhole S, Ellis S, Yeo A, Elcombe E, Johnson M. Evaluation of a midwifery initiated oral health-dental service program to im-prove oral health and birth outcomes for pregnant women: A multi-centre randomised controlled trial. Int J Nurs Stud. 2018 Jun;82:49-57. [DOI:10.1016/j.ijnurstu.2018.03.006] [PMID]
30. Mehrolhassani MH, Dehnavieh R, Haghdoost AA, Khosravi S. Evaluation of the primary healthcare program in Iran: a systematic review. Aust J Prim Health. 2018 Nov;24 (5):359-67. [DOI:10.1071/PY18008] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |