

Volume 8, Issue 1 (1-2023)
J Res Dent Maxillofac Sci 2023, 8(1): 1-10 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sedaghati G, Asnaashari E, Khalilak Z. In Vitro Comparison of the Push-Out Bond Strength of RetroMTA, OrthoMTA, and ProRoot MTA. J Res Dent Maxillofac Sci 2023; 8 (1) :1-10
URL: http://jrdms.dentaliau.ac.ir/article-1-408-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-408-en.html



1- Department of Orthodontics, School of Dentistry, Isfahan (Khorasgan) Branch, Islamic Azad University, Isfahan, Iran
2- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,Ehsan_dmd@yahoo.com
3- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
2- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran ,
3- Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
Full-Text [PDF 883 kb]
(746 Downloads)
| Abstract (HTML) (1797 Views)
Introduction
Creating a hermetic seal to prevent microleakage from the oral environment and periradicular tissue is a common concern following the use of biomaterials for procedures such as perforation repair, apical plug formation, and vital pulp therapy [1,2]. Biomaterials should ideally have adequate resistance against the dislodging forces such as mechanical loads, occlusal loads, and compressive loads. Not paying attention to adhesion of biomaterials to dentin and their resistance against the dislodging forces would result in their dislodgement, breached seal, microleakage, and eventual failure of endodontic treatment [2-5].
To date, several materials have been proposed for repair of perforations such as amalgam, temporary restorative materials, glass ionomer, and calcium hydroxide. However, mineral trioxide aggregate (MTA) is often the material of choice for perforation repair and vital pulp therapy due to its favorable properties such as optimal surface hardness and push-out bond strength (PBS) to dentin and other suitable physical and biological characteristics [6-11]. MTA was first introduced in 1993. Aside from the abovementioned favorable properties, MTA has shortcomings e.g., long setting time and difficult handling [12,13]. The PBS refers to resistance of a material against the dislodging forces [14].
Different MTA brands have different PBS values. To date, ProRoot MTA has shown the highest PBS [15]. Recently, OrthoMTA (BioMTA, Seoul, South Korea) was introduced to the market, which is supplied in the form of a biocompatible pure white powder composing of acetylene sulfide, tricalcium silicate, etc. This hydrophilic material forms hydroxyapatite in dentinal tubules and induces cementum formation at the root apex as soon as it is mixed with water [16]. The manufacturer of OrthoMTA claims that it has a composition similar to that of ProRoot MTA, with the difference that OrthoMTA has lower heavy metal content than ProRoot MTA [17]. OrthoMTA provides physical, chemical and biological seal, and has clinical antibacterial properties as well [15].
RetroMTA (BioMTA, Seoul, South Korea) is a recently introduced hydraulic bioceramic used for vital pulp therapy and perforation repair. Its powder is composed of small hydrophilic particles that set in presence of water. It has been claimed that RetroMTA has a shorter setting time, optimal handling properties, no cytotoxicity, and higher wash-out resistance than ProRoot MTA. Also, its setting reactions start in presence of moisture and it does not contain heavy metals. Since no previous study has assessed the PBS of RetroMTA, this study aimed to compare the PBS of RetroMTA (BioMTA, South Korea), ProRoot MTA (Dentsply Sirona, USA), and OrthoMTA (BioMTA, South Korea.
Materials and Methods
This in vitro, experimental study assessed recently extracted single-rooted human canine teeth. The teeth were decoronated, and their root canals were enlarged with #2 to #5 Gates-Glidden drills by 1.3 mm. They were mounted in acrylic resin, and were then transversely sectioned at the center by a low-speed diamond saw (Fanavarane Pars, Iran) under water coolant to obtain discs with 2 mm thickness (Figure 1).
Figure 1. The teeth were transversely sectioned to obtain discs with 2 mm thickness
The sample size was calculated to be 54 discs. The specimens were then randomly assigned to 6 groups (n=9). At a neutral pH, OrthoMTA, ProRoot MTA, and RetroMTA were applied in the lumen of dentin discs in the form of a thin layer, each in 2 groups. Excess material was removed by a scalpel. The specimens were then wrapped in a moist gauze and incubated at 37°C and 100% humidity. The PBS was measured by a universal testing machine after 10 minutes in one OrthoMTA, one ProRoot MTA, and one RetroMTA group, and after 4 hours (primary setting time of MTA) in the remaining three groups. The specimens were then placed on a metal slab that had a central hole for free movement of the piston of the universal testing machine (TTM, Germany) (Figure 2). Compressive load was applied on the surface of each specimen by the movement of the tester probe at a constant crosshead speed of 1 mm/minute (Figure 3).
Figure 2. Measuring the PBS in a universal testing machine
Figure 3. Discs placed in universal testing machine
The maximum load causing dislodgement of the material from the lumen was recorded in Newtons (N). The PBS was calculated in megapascals (MPs) by dividing the load at dislodgement by the cross-sectional area of the material using the formula N/2 πrh, where π is a constant value of 3.14, r is the radius of the lumen, and h is the thickness of root dentin cross-section in millimeters (mm).
The mode of failure was determined under a stereomicroscope (Optika, Italy) at x10 magnification. The mode of failure was categorized as adhesive failure at the MTA-dentin interface, cohesive failure within the MTA, or mixed (Figure 4).
This study was approved by the Dental Research Committee and Dental Ethics Committee of Faculty of Dentistry, Islamic
Azad Tehran Medical University (IR.IAU.DENTAL.REC.1399.235).
The PBS data of the groups were compared by two-way ANOVA. The mode of failure was statistically analyzed by the Chi-square test using SPSS version 22.
Figure 4. (A) Adhesive failure; (B) Cohesive failure; (C) Mixed failure
Results
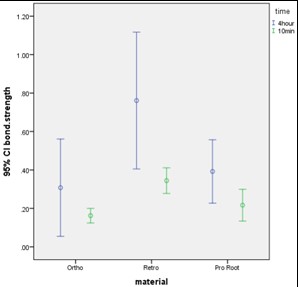
the PBS of the groups based on the type of material and time of measurement are presented in Table 1. The PBS was 0.16±0.04 MPa and 0.31±0.32 MPa for OrthoMTA, 0.34±0.08 MPa and 0.76±0.46 MPa for RetroMTA, and 0.2167±0.1 MPa and 0.39±0.21 MPa for ProRoot MTA after 10 minutes and 4 hours, respectively. RetroMTA showed maximum PBS at both 10 minutes and 4 hours.
The interaction effect of time and material on PBS was not significant (P=0.227). In other words, the materials had a significant difference in PBS at both time points (P=0.001), such that the mean PBS of RetroMTA was significantly higher than that of ProRoot MTA and OrthoMTA (P<0.014).
The PBS of all materials was significantly higher at 4 hours compared with 10 minutes (P=0.001). The mean PBS of OrthoMTA, RetroMTA and ProRoot MTA at 10 minutes and 4 hours is reported in Figure 5.
Table 1. PBS of the groups based on the type of material and time of measurement using two-way ANOVA(n=9)
Full-Text: (812 Views)
| Abstract
Background and Aim: Different MTA brands may have different push-out bond strength (PBS) values in 10 minutes and 4 hours. Thus, this study aimed to compare the PBS of RetroMTA, OrthoMTA, and ProRoot MTA. Materials and Methods: In this in vitro, experimental study, 54 dentin discs with 2 mm diameter and a central lumen with 1.3 mm radius were used in each of the RetroMTA, OrthoMTA, and ProRoot MTA groups (18 discs for each group). The samples were wrapped in a moist gauze and incubated at 37°C and 100% humidity. The PBS was measured by a universal testing machine at a crosshead speed of 1 mm/minute after 10 minutes and 4 hours. The mode of failure was also categorized by using a stereomicroscope. The mean PBS of the three groups was compared using two-way ANOVA. The mode of failure was analyzed by the Chi-square test. Results: The interaction effect of time and material on PBS was not significant (P=0.227). At both time points, the PBS of the three groups was significantly different (P=0.001), and RetroMTA showed significantly higher PBS (P<0.014). However, the PBS of OrthoMTA and ProRoot MTA was not significantly different (P=0.695). The PBS of all materials at 4 hours was significantly higher than that at 10 minutes (P=0.001). Conclusion: RetroMTA was superior to ProRoot MTA and OrthoMTA regarding the PBS after 4 hours. Key Words: Biocompatible Materials; Mineral Trioxide Aggregate; Dental Bonding; Root Canal Therapy |
Introduction
Creating a hermetic seal to prevent microleakage from the oral environment and periradicular tissue is a common concern following the use of biomaterials for procedures such as perforation repair, apical plug formation, and vital pulp therapy [1,2]. Biomaterials should ideally have adequate resistance against the dislodging forces such as mechanical loads, occlusal loads, and compressive loads. Not paying attention to adhesion of biomaterials to dentin and their resistance against the dislodging forces would result in their dislodgement, breached seal, microleakage, and eventual failure of endodontic treatment [2-5].
To date, several materials have been proposed for repair of perforations such as amalgam, temporary restorative materials, glass ionomer, and calcium hydroxide. However, mineral trioxide aggregate (MTA) is often the material of choice for perforation repair and vital pulp therapy due to its favorable properties such as optimal surface hardness and push-out bond strength (PBS) to dentin and other suitable physical and biological characteristics [6-11]. MTA was first introduced in 1993. Aside from the abovementioned favorable properties, MTA has shortcomings e.g., long setting time and difficult handling [12,13]. The PBS refers to resistance of a material against the dislodging forces [14].
Different MTA brands have different PBS values. To date, ProRoot MTA has shown the highest PBS [15]. Recently, OrthoMTA (BioMTA, Seoul, South Korea) was introduced to the market, which is supplied in the form of a biocompatible pure white powder composing of acetylene sulfide, tricalcium silicate, etc. This hydrophilic material forms hydroxyapatite in dentinal tubules and induces cementum formation at the root apex as soon as it is mixed with water [16]. The manufacturer of OrthoMTA claims that it has a composition similar to that of ProRoot MTA, with the difference that OrthoMTA has lower heavy metal content than ProRoot MTA [17]. OrthoMTA provides physical, chemical and biological seal, and has clinical antibacterial properties as well [15].
RetroMTA (BioMTA, Seoul, South Korea) is a recently introduced hydraulic bioceramic used for vital pulp therapy and perforation repair. Its powder is composed of small hydrophilic particles that set in presence of water. It has been claimed that RetroMTA has a shorter setting time, optimal handling properties, no cytotoxicity, and higher wash-out resistance than ProRoot MTA. Also, its setting reactions start in presence of moisture and it does not contain heavy metals. Since no previous study has assessed the PBS of RetroMTA, this study aimed to compare the PBS of RetroMTA (BioMTA, South Korea), ProRoot MTA (Dentsply Sirona, USA), and OrthoMTA (BioMTA, South Korea.
Materials and Methods
This in vitro, experimental study assessed recently extracted single-rooted human canine teeth. The teeth were decoronated, and their root canals were enlarged with #2 to #5 Gates-Glidden drills by 1.3 mm. They were mounted in acrylic resin, and were then transversely sectioned at the center by a low-speed diamond saw (Fanavarane Pars, Iran) under water coolant to obtain discs with 2 mm thickness (Figure 1).
Figure 1. The teeth were transversely sectioned to obtain discs with 2 mm thickness
{kind=link}
The sample size was calculated to be 54 discs. The specimens were then randomly assigned to 6 groups (n=9). At a neutral pH, OrthoMTA, ProRoot MTA, and RetroMTA were applied in the lumen of dentin discs in the form of a thin layer, each in 2 groups. Excess material was removed by a scalpel. The specimens were then wrapped in a moist gauze and incubated at 37°C and 100% humidity. The PBS was measured by a universal testing machine after 10 minutes in one OrthoMTA, one ProRoot MTA, and one RetroMTA group, and after 4 hours (primary setting time of MTA) in the remaining three groups. The specimens were then placed on a metal slab that had a central hole for free movement of the piston of the universal testing machine (TTM, Germany) (Figure 2). Compressive load was applied on the surface of each specimen by the movement of the tester probe at a constant crosshead speed of 1 mm/minute (Figure 3).
Figure 2. Measuring the PBS in a universal testing machine
{kind=link}
Figure 3. Discs placed in universal testing machine
{kind=link}
The maximum load causing dislodgement of the material from the lumen was recorded in Newtons (N). The PBS was calculated in megapascals (MPs) by dividing the load at dislodgement by the cross-sectional area of the material using the formula N/2 πrh, where π is a constant value of 3.14, r is the radius of the lumen, and h is the thickness of root dentin cross-section in millimeters (mm).
The mode of failure was determined under a stereomicroscope (Optika, Italy) at x10 magnification. The mode of failure was categorized as adhesive failure at the MTA-dentin interface, cohesive failure within the MTA, or mixed (Figure 4).
This study was approved by the Dental Research Committee and Dental Ethics Committee of Faculty of Dentistry, Islamic
Azad Tehran Medical University (IR.IAU.DENTAL.REC.1399.235).
The PBS data of the groups were compared by two-way ANOVA. The mode of failure was statistically analyzed by the Chi-square test using SPSS version 22.
Figure 4. (A) Adhesive failure; (B) Cohesive failure; (C) Mixed failure
{kind=link}
Results
the PBS of the groups based on the type of material and time of measurement are presented in Table 1. The PBS was 0.16±0.04 MPa and 0.31±0.32 MPa for OrthoMTA, 0.34±0.08 MPa and 0.76±0.46 MPa for RetroMTA, and 0.2167±0.1 MPa and 0.39±0.21 MPa for ProRoot MTA after 10 minutes and 4 hours, respectively. RetroMTA showed maximum PBS at both 10 minutes and 4 hours.
The interaction effect of time and material on PBS was not significant (P=0.227). In other words, the materials had a significant difference in PBS at both time points (P=0.001), such that the mean PBS of RetroMTA was significantly higher than that of ProRoot MTA and OrthoMTA (P<0.014).
The PBS of all materials was significantly higher at 4 hours compared with 10 minutes (P=0.001). The mean PBS of OrthoMTA, RetroMTA and ProRoot MTA at 10 minutes and 4 hours is reported in Figure 5.
Table 1. PBS of the groups based on the type of material and time of measurement using two-way ANOVA(n=9)
{kind=link}
Table 2. Mode of failure of materials at different time points
Figure 5. PBS of the groups
Regarding the mode of failure of the materials at different time points (Table 2), adhesive failure had the highest frequency (60%) at 4 hours; while, cohesive failure had the highest frequency (50%) at 10 minutes in OrthoMTA group. Cohesive failure had the highest frequency at both 4 hours (60%) and 10 minutes (80%) in ProRoot MTA group. Cohesive failure had the highest frequency at both 4 hours (50%) and 10 minutes (60%) in RetroMTA group.
Discussion
In this study, the PBS of ProRoot MTA, OrthoMTA, and RetroMTA was measured after 10 minutes and 4 hours. An ideal material should be able to seal the root canal, root end cavity, and the surrounding tissues, prevent bacterial leakage from the peri-radicular areas, and resist the dislodging forces. MTA has the majority of these properties, and is the gold-standard root-end filling material [18] and vital pulp therapy material due to its high sealing ability [19]. The success of endodontic treatment after vital pulp therapy depends on optimal application of filling material to well resist the dislodging forces applied during the condensation of permanent restorative material. The compressive force applied for condensation of amalgam can be as high as 9.4±8.2 MPa and 5.8±5.1 MPa by using a condenser [20]. Such a high pressure can lead to dislodgement of the biomaterial used for vital pulp therapy [4,5,21,22]. Thus, the PBS of such materials is an important factor in the clinical setting. In the present study, the PBS of all types of MTA at both 10 minutes and 4 hours was lower than the amalgam condensing forces, which can result in dislodgement of MTA. Thus, a strong base or liner such as resin modified glass ionomer is needed to cover the MTA before amalgam condensation.
This study evaluated 40 single-rooted human canine teeth, which was close to the sample size of a study by Chen et al. [23] Canine teeth were used in this study since they have longer roots, and higher number of dentin discs can be obtained from them. The root canals were enlarged by 1.3 mm using Gates-Glidden drills to simulate a perforation in the clinical setting, and were mounted in acrylic resin. They were then sectioned into 2 mm thick slices to obtain cavities with similar depth and diameter for standardized application of materials. The obtained discs were wrapped in a moist gauze and stored at 37°C and 100% humidity to simulate the oral clinical setting. The PBS was measured after 10 minutes; because in the clinical setting, the time interval between the application of MTA and final restoration of the tooth is approximately 10 minutes. The 4-hour assessment time point was according to the brochure of the materials, stating that the primary setting time of the materials is 4 hours. The results showed that the PBS was 0.16±0.04 MPa and 0.31±0.32 MPa for OrthoMTA, 0.34±0.08 MPa and 0.76±0.46 MPa for RetroMTA, and 0.2167±0.1 MPa and 0.39±0.21 MPa for ProRoot MTA after 10 minutes and 4 hours, respectively. The materials showed significantly different PBS values at 10 minutes and 4 hours (P=0.048).
It has been discussed that optimal biocompatibility and sealability of MTA are attributed to the physicochemical reactions between the MTA and dentin. The PBS of MTA to dentin indicates the rate of adhesion between them. Several tests are used to assess the adhesion of dental materials to dentin such as the tensile, shear and PBS tests [24]. Despite the availability of several techniques for assessment of the bond strength of MTA, the PBS test provides reliable and efficient results [25]. Thus, the PBS test was used in the present study to assess the bond strength of different types of MTA to dentin.
Presence of moisture is important for the MTA setting. The curing conditions are also important in MTA retention because the PBS of dry-cured MTA is significantly lower than that of wet-cured MTA. Thus, in order to achieve an optimal PBS, wet environment is required during MTA setting. Moreover, the retention and PBS of MTA improve proportionally to the duration of storage in a wet environment. Thus, in the clinical setting, at least the first 3 days of MTA curing should be in presence of water to achieve optimally high retention. Also, presence of moisture for at least the first 3 days is imperative to achieve adequate resistance of MTA against the dislodging forces [2]. It has been reported that MTA stored in a humid environment for 2-7 days has higher strength compared with MTA stored for 4 hours in a wet environment [26]. In the current study, the specimens were stored in a humid environment for 10 minutes and 4 hours.
The sealability of MTA may increase by its apatite-forming potential and bioactivity [27]. ProRoot MTA contains dicalcium silicate, tricalcium silicate, tricalcium aluminoferrite, tricalcium aluminate, calcium sulfate dihydrate, bismuth oxide, tricalcium oxide, and other oxides that can set in presence of water [28,29]. ProRoot MTA has a relatively slow setting reaction. Although this property may minimize leakage, ProRoot MTA may be washed off in case of bleeding when used for vital pulp therapy, and lead to treatment failure [3]. Difficult handling and high cost are among the main reasons reported by endodontists for not using ProRoot MTA [12].
OrthoMTA contains dicalcium silicate, tricalcium silicate, tetracalcium aluminoferrite, tricalcium aluminate, calcium sulfate, free calcium oxides, and bismuth oxide [28]. It is bioactive and results in release of calcium ions through the apical foramen, leading to formation of a hydroxyapatite layer. Moreover, the manufacturer claims that OrthoMTA has lower content of heavy metals than ProRoot MTA [30]. Shahi et al. [31] simulated the in vivo environment by wrapping the root segments in a gauze dipped in simulated tissue fluid. Formation of hydroxyapatite layer and intratubular mineralization may affect the PBS. In the current study, the samples were wrapped in a moist gauze to provide sufficient humidity for MTA setting and were then incubated.
Water sorption is a complex process, which can affect the chemical, biological, and physical characteristics of the materials [32]. Presence of excess water during mixing can complicate the handling and application of materials. The amount of water should be proportionate to the amount of powder in order not to affect the bioactivity, handling, or physical properties of the material. Nekoufar et al [33]. reported variations in the amount of water supplied in ProRoot MTA packages, which may result in unpredictable consequences in the clinical and in vitro settings such as incomplete setting (which might affect the PBS) and poor handling properties. Encapsulation of predetermined amounts of MTA powder and water would be beneficial because it would standardize the powder to water ratio and the mixing technique. Moreover, it would lower the risk of common manipulations and errors during weighing and mixing. Nonetheless, they showed that use of encapsulated MTA did not improve the PBS in comparison with other mixing methods namely ultrasonic and conventional mixing. In our study, conventional mixing was performed, and the correct ratio of powder to water was observed.
Kim et al. compared the biological characteristics of ProRoot MTA, OrthoMTA, and EndocemMTA [28]. They compared the setting time of the three materials and reported that the setting time was 318.56±0.0 minutes for ProRoot MTA and 324.2±3.1 minutes for OrthoMTA. In their study, OrthoMTA had a longer setting time, which was in agreement with our findings regarding lower PBS of OrthoMTA than ProRoot MTA. Alsubait et al, in 2014 compared the PBS of ProRoot MTA, BioAggregate, and Biodentine [34]. They incubated the specimens for 3 days and reported that the mean PBS of ProRoot MTA was 26.49±23.5 MPa, which was different from the value in our study (0.39±0.21 MPa); this difference may be attributed to different incubation times of specimens. Aggarwal et al, in 2013 compared the PBS of three biomaterials for furcal perforation repair [35]. They used ProRoot MTA and measured its PBS after 24 hours, which was found to be 5.0±2.4 MPa; this value was different from that in our study. In the present study, the maximum PBS of ProRoot MTA after 4 hours was 96.27±0.0 MPa. Difference in the results of the two studies in this respect may be due to different incubation times. Ertas et al. compared the PBS of different MTA types [15]. They used ProRoot MTA and incubated the specimens for 3 days. They reported that the mean PBS of ProRoot MTA was 12.5±2.7 MPa, which was different from the reported value in our study (96.27±0.0 MPa after 4 hours of incubation). This difference may be explained by the different incubation periods.
In the current study, the mode of failure of specimens was inspected under a stereomicroscope at x16 magnification. Different modes of failure may be explained by different size of particles, which would affect the penetration of cements into dentinal tubules. Small size of particles and similar elements may play a role in better interlocking of biomaterials in dentin, which would eventually result in cohesive failure within the cement [36]. The mode of failure in a study by Guneser et al. [37], was adhesive in all groups, which was similar to the results of Shokouhinejad et al. [4], Saghiri et al. [21,22], and Hong et al. [38], who reported that the mode of failure was dominantly adhesive. This mode of failure may be due to short duration of storage prior to measurement of bond strength, which was 2 days in the study by Guneser et al. [37], 3 days in the study by Saghiri et al., [22] and 7 days in the study by Vanderweele et al. [39]. In the present study, the mode of failure was cohesive in most cases, which was different from the results of previous studies, probably due to the short duration of storage of specimens (10 minutes and 4 hours) prior to the PBS test.
Rahoma et al. [40] compared the PBS of OrthoMTA, MTA Angelus, and ProRoot MTA. They stored the specimens in distilled water for 6 months. The results showed that the PBS was 68.69±29 MPa for OrthoMTA, 54.42±32 MPa for MTA Angelus, and 72.75±26 MPa for ProRoot MTA. The difference in the PBS of the three materials was not significant, which was different from our findings.
Jain et al. [41] evaluated the effect of intracanal medicaments and acidic environment on PBS of Biodentine and MTA Plus. They evaluated 40 teeth in four groups (n=10) of calcium hydroxide in presence of acidic environment, calcium hydroxide in absence of acidic environment, no medicament in presence of acidic environment, and no medicament in absence of acidic environment. The specimens were stored at room temperature for 7 days. They used Biodentine and MTA Plus, and found no significant difference between their PBS. They concluded that MTA was more suitable for apexification. Their results were in agreement with our findings.
Prasanthi et al. [42] . evaluated the effect of 17% EDTA and 2% chitosan on PBS of Biodentine and ProRoot MTA. They evaluated 60 Biodentine and ProRoot MTA specimens. The samples were immersed in 17% EDTA, 2% chitosan, and saline for 30 minutes and incubated them for 48 hours. Biodentine showed higher PBS than ProRoot MTA, which was different from our results.
Conclusion
In vital pulp therapy and MTA plug placement, the PBS of MTA would not be high enough for placement of the final restoration earlier than 4 hours. According to the current results, RetroMTA had higher PBS than ProRoot MTA and OrthoMTA.
Figure 5. PBS of the groups
{kind=link}
Regarding the mode of failure of the materials at different time points (Table 2), adhesive failure had the highest frequency (60%) at 4 hours; while, cohesive failure had the highest frequency (50%) at 10 minutes in OrthoMTA group. Cohesive failure had the highest frequency at both 4 hours (60%) and 10 minutes (80%) in ProRoot MTA group. Cohesive failure had the highest frequency at both 4 hours (50%) and 10 minutes (60%) in RetroMTA group.
Discussion
In this study, the PBS of ProRoot MTA, OrthoMTA, and RetroMTA was measured after 10 minutes and 4 hours. An ideal material should be able to seal the root canal, root end cavity, and the surrounding tissues, prevent bacterial leakage from the peri-radicular areas, and resist the dislodging forces. MTA has the majority of these properties, and is the gold-standard root-end filling material [18] and vital pulp therapy material due to its high sealing ability [19]. The success of endodontic treatment after vital pulp therapy depends on optimal application of filling material to well resist the dislodging forces applied during the condensation of permanent restorative material. The compressive force applied for condensation of amalgam can be as high as 9.4±8.2 MPa and 5.8±5.1 MPa by using a condenser [20]. Such a high pressure can lead to dislodgement of the biomaterial used for vital pulp therapy [4,5,21,22]. Thus, the PBS of such materials is an important factor in the clinical setting. In the present study, the PBS of all types of MTA at both 10 minutes and 4 hours was lower than the amalgam condensing forces, which can result in dislodgement of MTA. Thus, a strong base or liner such as resin modified glass ionomer is needed to cover the MTA before amalgam condensation.
This study evaluated 40 single-rooted human canine teeth, which was close to the sample size of a study by Chen et al. [23] Canine teeth were used in this study since they have longer roots, and higher number of dentin discs can be obtained from them. The root canals were enlarged by 1.3 mm using Gates-Glidden drills to simulate a perforation in the clinical setting, and were mounted in acrylic resin. They were then sectioned into 2 mm thick slices to obtain cavities with similar depth and diameter for standardized application of materials. The obtained discs were wrapped in a moist gauze and stored at 37°C and 100% humidity to simulate the oral clinical setting. The PBS was measured after 10 minutes; because in the clinical setting, the time interval between the application of MTA and final restoration of the tooth is approximately 10 minutes. The 4-hour assessment time point was according to the brochure of the materials, stating that the primary setting time of the materials is 4 hours. The results showed that the PBS was 0.16±0.04 MPa and 0.31±0.32 MPa for OrthoMTA, 0.34±0.08 MPa and 0.76±0.46 MPa for RetroMTA, and 0.2167±0.1 MPa and 0.39±0.21 MPa for ProRoot MTA after 10 minutes and 4 hours, respectively. The materials showed significantly different PBS values at 10 minutes and 4 hours (P=0.048).
It has been discussed that optimal biocompatibility and sealability of MTA are attributed to the physicochemical reactions between the MTA and dentin. The PBS of MTA to dentin indicates the rate of adhesion between them. Several tests are used to assess the adhesion of dental materials to dentin such as the tensile, shear and PBS tests [24]. Despite the availability of several techniques for assessment of the bond strength of MTA, the PBS test provides reliable and efficient results [25]. Thus, the PBS test was used in the present study to assess the bond strength of different types of MTA to dentin.
Presence of moisture is important for the MTA setting. The curing conditions are also important in MTA retention because the PBS of dry-cured MTA is significantly lower than that of wet-cured MTA. Thus, in order to achieve an optimal PBS, wet environment is required during MTA setting. Moreover, the retention and PBS of MTA improve proportionally to the duration of storage in a wet environment. Thus, in the clinical setting, at least the first 3 days of MTA curing should be in presence of water to achieve optimally high retention. Also, presence of moisture for at least the first 3 days is imperative to achieve adequate resistance of MTA against the dislodging forces [2]. It has been reported that MTA stored in a humid environment for 2-7 days has higher strength compared with MTA stored for 4 hours in a wet environment [26]. In the current study, the specimens were stored in a humid environment for 10 minutes and 4 hours.
The sealability of MTA may increase by its apatite-forming potential and bioactivity [27]. ProRoot MTA contains dicalcium silicate, tricalcium silicate, tricalcium aluminoferrite, tricalcium aluminate, calcium sulfate dihydrate, bismuth oxide, tricalcium oxide, and other oxides that can set in presence of water [28,29]. ProRoot MTA has a relatively slow setting reaction. Although this property may minimize leakage, ProRoot MTA may be washed off in case of bleeding when used for vital pulp therapy, and lead to treatment failure [3]. Difficult handling and high cost are among the main reasons reported by endodontists for not using ProRoot MTA [12].
OrthoMTA contains dicalcium silicate, tricalcium silicate, tetracalcium aluminoferrite, tricalcium aluminate, calcium sulfate, free calcium oxides, and bismuth oxide [28]. It is bioactive and results in release of calcium ions through the apical foramen, leading to formation of a hydroxyapatite layer. Moreover, the manufacturer claims that OrthoMTA has lower content of heavy metals than ProRoot MTA [30]. Shahi et al. [31] simulated the in vivo environment by wrapping the root segments in a gauze dipped in simulated tissue fluid. Formation of hydroxyapatite layer and intratubular mineralization may affect the PBS. In the current study, the samples were wrapped in a moist gauze to provide sufficient humidity for MTA setting and were then incubated.
Water sorption is a complex process, which can affect the chemical, biological, and physical characteristics of the materials [32]. Presence of excess water during mixing can complicate the handling and application of materials. The amount of water should be proportionate to the amount of powder in order not to affect the bioactivity, handling, or physical properties of the material. Nekoufar et al [33]. reported variations in the amount of water supplied in ProRoot MTA packages, which may result in unpredictable consequences in the clinical and in vitro settings such as incomplete setting (which might affect the PBS) and poor handling properties. Encapsulation of predetermined amounts of MTA powder and water would be beneficial because it would standardize the powder to water ratio and the mixing technique. Moreover, it would lower the risk of common manipulations and errors during weighing and mixing. Nonetheless, they showed that use of encapsulated MTA did not improve the PBS in comparison with other mixing methods namely ultrasonic and conventional mixing. In our study, conventional mixing was performed, and the correct ratio of powder to water was observed.
Kim et al. compared the biological characteristics of ProRoot MTA, OrthoMTA, and EndocemMTA [28]. They compared the setting time of the three materials and reported that the setting time was 318.56±0.0 minutes for ProRoot MTA and 324.2±3.1 minutes for OrthoMTA. In their study, OrthoMTA had a longer setting time, which was in agreement with our findings regarding lower PBS of OrthoMTA than ProRoot MTA. Alsubait et al, in 2014 compared the PBS of ProRoot MTA, BioAggregate, and Biodentine [34]. They incubated the specimens for 3 days and reported that the mean PBS of ProRoot MTA was 26.49±23.5 MPa, which was different from the value in our study (0.39±0.21 MPa); this difference may be attributed to different incubation times of specimens. Aggarwal et al, in 2013 compared the PBS of three biomaterials for furcal perforation repair [35]. They used ProRoot MTA and measured its PBS after 24 hours, which was found to be 5.0±2.4 MPa; this value was different from that in our study. In the present study, the maximum PBS of ProRoot MTA after 4 hours was 96.27±0.0 MPa. Difference in the results of the two studies in this respect may be due to different incubation times. Ertas et al. compared the PBS of different MTA types [15]. They used ProRoot MTA and incubated the specimens for 3 days. They reported that the mean PBS of ProRoot MTA was 12.5±2.7 MPa, which was different from the reported value in our study (96.27±0.0 MPa after 4 hours of incubation). This difference may be explained by the different incubation periods.
In the current study, the mode of failure of specimens was inspected under a stereomicroscope at x16 magnification. Different modes of failure may be explained by different size of particles, which would affect the penetration of cements into dentinal tubules. Small size of particles and similar elements may play a role in better interlocking of biomaterials in dentin, which would eventually result in cohesive failure within the cement [36]. The mode of failure in a study by Guneser et al. [37], was adhesive in all groups, which was similar to the results of Shokouhinejad et al. [4], Saghiri et al. [21,22], and Hong et al. [38], who reported that the mode of failure was dominantly adhesive. This mode of failure may be due to short duration of storage prior to measurement of bond strength, which was 2 days in the study by Guneser et al. [37], 3 days in the study by Saghiri et al., [22] and 7 days in the study by Vanderweele et al. [39]. In the present study, the mode of failure was cohesive in most cases, which was different from the results of previous studies, probably due to the short duration of storage of specimens (10 minutes and 4 hours) prior to the PBS test.
Rahoma et al. [40] compared the PBS of OrthoMTA, MTA Angelus, and ProRoot MTA. They stored the specimens in distilled water for 6 months. The results showed that the PBS was 68.69±29 MPa for OrthoMTA, 54.42±32 MPa for MTA Angelus, and 72.75±26 MPa for ProRoot MTA. The difference in the PBS of the three materials was not significant, which was different from our findings.
Jain et al. [41] evaluated the effect of intracanal medicaments and acidic environment on PBS of Biodentine and MTA Plus. They evaluated 40 teeth in four groups (n=10) of calcium hydroxide in presence of acidic environment, calcium hydroxide in absence of acidic environment, no medicament in presence of acidic environment, and no medicament in absence of acidic environment. The specimens were stored at room temperature for 7 days. They used Biodentine and MTA Plus, and found no significant difference between their PBS. They concluded that MTA was more suitable for apexification. Their results were in agreement with our findings.
Prasanthi et al. [42] . evaluated the effect of 17% EDTA and 2% chitosan on PBS of Biodentine and ProRoot MTA. They evaluated 60 Biodentine and ProRoot MTA specimens. The samples were immersed in 17% EDTA, 2% chitosan, and saline for 30 minutes and incubated them for 48 hours. Biodentine showed higher PBS than ProRoot MTA, which was different from our results.
Conclusion
In vital pulp therapy and MTA plug placement, the PBS of MTA would not be high enough for placement of the final restoration earlier than 4 hours. According to the current results, RetroMTA had higher PBS than ProRoot MTA and OrthoMTA.
Type of Study: Original article |
Subject:
Endodontics
References
1. Hartwell GR, England MC. Healing of furcation perforations in primate teeth after repair with decalcified freeze-dried bone: a longitudinal study. J Endod. 1993 Jul; 19 (7):357-61. [DOI:10.1016/S0099-2399(06)81363-4] [PMID]
2. Gancedo-Caravia L, Garcia-Barbero E. Influence of humidity and setting time on the push-out strength of mineral trioxide aggregate obturations. J Endod. 2006 Sep; 32(9):894-6. [DOI:10.1016/j.joen.2006.03.004] [PMID]
3. Kogan P, He J, Glickman GN, Watanabe I. The effects of various additives on setting properties of MTA. J Endod. 2006 Jun;32(6):569-72. [DOI:10.1016/j.joen.2005.08.006] [PMID]
4. Shokouhinejad N, Nekoofar MH, Iravani A, Kharrazifard MJ, Dummer PM. Effect of acidic environment on the push-out bond strength of mineral trioxide aggregate. J Endod. 2010 May;36(5):871-4. [DOI:10.1016/j.joen.2009.12.025] [PMID]
5. Hashem AA, Wanees Amin SA. The effect of acidity on dislodgment resistance of mineral trioxide aggregate and bioaggregate in furcation perforations: an in vitro comparative study. J Endod. 2012 Feb;38(2):245-9. [DOI:10.1016/j.joen.2011.09.013] [PMID]
6. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod. 1993 Dec;19(12):591-5. [DOI:10.1016/S0099-2399(06)80271-2] [PMID]
7. Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod. 1993 Nov;19(11):541-4. [DOI:10.1016/S0099-2399(06)81282-3] [PMID]
8. Belli S, Zhang Y, Pereira PN, Pashley DH. Adhesive sealing of the pulp chamber. J Endod. 2001 Aug;27(8):521-6. [DOI:10.1097/00004770-200108000-00006] [PMID]
9. Chng HK, Islam I, Yap AU, Tong YW, Koh ET. Properties of a new root-end filling material. J Endod. 2005 Sep;31(9): 665-8. [DOI:10.1097/01.don.0000157993.89164.be] [PMID]
10. Torabinejad M, Parirokh M. Mineral trioxide aggregate: a comprehensive literature review--part II: leakage and biocompatibility investigations. J Endod. 2010 Feb;36(2): 190-202. [DOI:10.1016/j.joen.2009.09.010] [PMID]
11. Johnson BR. Considerations in the selection of a root-end filling material. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Apr;87(4):398-404. [DOI:10.1016/S1079-2104(99)70237-4] [PMID]
12. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review--Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010 Mar;36(3):400-13. [DOI:10.1016/j.joen.2009.09.009] [PMID]
13. Eskandarizadeh A, Shahpasandzadeh MH, Shahpasandzadeh M, Torabi M, Parirokh M. A comparative study on dental pulp response to calcium hydroxide, white and grey mineral trioxide aggregate as pulp capping agents. J Conserv Dent. 2011 Oct;14(4):351-5. [DOI:10.4103/0972-0707.87196] [PMID] [PMCID]
14. Adl A, Sobhnamayan F, Kazemi O. Comparison of push-out bond strength of mineral trioxide aggregate and calcium enriched mixture cement as root end filling materials. Dent Res J (Isfahan). 2014 Sep;11(5):564-7.
15. Ertas H, Kucukyilmaz E, Ok E, Uysal B. Push-out bond strength of different mineral trioxide aggregates. Eur J Dent. 2014 Jul;8(3):348-52. [DOI:10.4103/1305-7456.137646] [PMID] [PMCID]
16. BioMTA technologies. Physiochemical analysis. Available at: https://www.biomta.com.
17. Chang SW, Baek SH, Yang HC, Seo DG, Hong ST, Han SH, Lee Y, Gu Y, Kwon HB, Lee W, Bae KS, Kum KY. Heavy metal analysis of ortho MTA and ProRoot MTA. J Endod. 2011 Dec; 37(12):1673-6. [DOI:10.1016/j.joen.2011.08.020] [PMID]
18. Torabinejad M, Chivian N. Clinical appslications of mineral trioxide aggregate. J Endod. 1999 Mar;25(3):197-205. [DOI:10.1016/S0099-2399(99)80142-3] [PMID]
19. Saunders WP. A prospective clinical study of periradicular surgery using mineral trioxide aggregate as a root-end filling. J Endod. 2008 Jun;34(6):660-5. [DOI:10.1016/j.joen.2008.03.002] [PMID]
20. Lussi A, Brunner M, Portmann P, Buergin W. Condensation pressure during amalgam placement in patients. Eur J Oral Sci. 1995 Dec;103(6):388-93. [DOI:10.1111/j.1600-0722.1995.tb01862.x] [PMID]
21. Saghiri MA, Shokouhinejad N, Lotfi M, Aminsobhani M, Saghiri AM. Push-out bond strength of mineral trioxide aggregate in the presence of alkaline pH. J Endod. 2010 Nov; 36(11):1856-9. [DOI:10.1016/j.joen.2010.08.022] [PMID]
22. Saghiri MA, Garcia-Godoy F, Gutmann JL, Lotfi M, Asatourian A, Ahmadi H. Push-out bond strength of a nano-modified mineral trioxide aggregate. Dent Traumatol. 2013 Aug;29(4):323-7. [DOI:10.1111/j.1600-9657.2012.01176.x] [PMID]
23. Chen Q, Wei XY, Yi M, Bai YY, Cai Q, Wang XZ. Effect on the bond strengths of glass fiber posts functionalized with polydopamine after etching with hydrogen peroxide. Dent Mater J. 2015;34(6):740-5. [DOI:10.4012/dmj.2014-259] [PMID]
24. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J Endod. 2005 Feb;31(2):97-100. [DOI:10.1097/01.DON.0000133155.04468.41] [PMID]
25. Goracci C, Tavares AU, Fabianelli A, Monticelli F, Raffaelli O, Cardoso PC, Tay F, Ferrari M. The adhesion between fiber posts and root canal walls: comparison between microtensile and push-out bond strength measurements. Eur J Oral Sci. 2004 Aug;112(4):353-61. [DOI:10.1111/j.1600-0722.2004.00146.x] [PMID]
26. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review--Part I: chemical, physical, and antibacterial properties. J Endod. 2010 Jan;36(1):16-27. [DOI:10.1016/j.joen.2009.09.006] [PMID]
27. Gandolfi MG, Taddei P, Siboni F, Modena E, Ginebra MP, Prati C. Fluoride-containing nanoporous calcium-silicate MTA cements for endodontics and oral surgery: early fluorapatite formation in a phosphate-containing solution. Int Endod J. 2011 Oct;44(10):938-49. [DOI:10.1111/j.1365-2591.2011.01907.x] [PMID]
28. Kim M, Yang W, Kim H, Ko H. Comparison of the biological properties of ProRoot MTA, OrthoMTA, and Endocem MTA cements. J Endod. 2014 Oct;40(10):1649-53. [DOI:10.1016/j.joen.2014.04.013] [PMID]
29. Asgary S, Eghbal MJ, Parirokh M, Ghoddusi J, Kheirieh S, Brink F. Comparison of mineral trioxide aggregate's composition with Portland cements and a new endodontic cement. J Endod. 2009 Feb;35(2):243-50. [DOI:10.1016/j.joen.2008.10.026] [PMID]
30. Lee BN, Son HJ, Noh HJ, Koh JT, Chang HS, Hwang IN, Hwang YC, Oh WM. Cytotoxicity of newly developed ortho MTA root-end filling materials. J Endod. 2012 Dec; 38(12): 1627-30. [DOI:10.1016/j.joen.2012.09.004] [PMID]
31. Shahi S, Rahimi S, Yavari HR, Samiei M, Janani M, Bahari M, Abdolrahimi M, Pakdel F, Aghbali A. Effects of various mixing techniques on push-out bond strengths of white mineral trioxide aggregate. J Endod. 2012 Apr;38(4):501-4. [DOI:10.1016/j.joen.2012.01.001] [PMID]
32. Camilleri J. Hydration mechanisms of mineral trioxide aggregate. Int Endod J. 2007 Jun;40(6):462-70. [DOI:10.1111/j.1365-2591.2007.01248.x] [PMID]
33. Nekoofar MH, Haddad DC, Nolde J, Aseeley Z. Water content of ampoule packaged with ProRoot MTA. Int Endod J. 2009 Jun;42(6):549-51; author reply 552-3. [DOI:10.1111/j.1365-2591.2009.01541.x] [PMID]
34. Alsubait SA, Hashem Q, AlHargan N, AlMohimeed K, Alkahtani A. Comparative evaluation of push-out bond strength of ProRoot MTA, bioaggregate and biodentine. J Contemp Dent Pract. 2014 May 1;15(3):336-40. [DOI:10.5005/jp-journals-10024-1539] [PMID]
35. Aggarwal V, Singla M, Miglani S, Kohli S. Comparative evaluation of push-out bond strength of ProRoot MTA, Biodentine, and MTA Plus in furcation perforation repair. J Conserv Dent. 2013 Sep;16(5):462-5. doi: 10.4103/0972-0707.117504. Erratum in: J Conserv Dent. 2014 Jan;17(1):95. [DOI:10.4103/0972-0707.117504] [PMID] [PMCID]
36. Atmeh AR, Chong EZ, Richard G, Festy F, Watson TF. Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. J Dent Res. 2012 May;91(5):454-9. [DOI:10.1177/0022034512443068] [PMID] [PMCID]
37. Guneser MB, Akbulut MB, Eldeniz AU. Effect of various endodontic irrigants on the push-out bond strength of biodentine and conventional root perforation repair materials. J Endod. 2013 Mar;39(3):380-4. [DOI:10.1016/j.joen.2012.11.033] [PMID]
38. Hong ST, Bae KS, Baek SH, Kum KY, Shon WJ, Lee W. Effects of root canal irrigants on the push-out strength and hydration behavior of accelerated mineral trioxide aggregate in its early setting phase. J Endod. 2010;36(12):1995-9. [DOI:10.1016/j.joen.2010.08.039] [PMID]
39. Vanderweele RA, Schwartz SA, Beeson TJ. Effect of blood contamination on retention characteristics of MTA when mixed with different liquids. J Endod. 2006 May;32(5):421-4. [DOI:10.1016/j.joen.2005.09.007] [PMID]
40. Rahoma A, AlShwaimi E, Majeed A. Push-out bond strength of different types of mineral trioxide aggregate in root dentin. Int J Health Sci (Qassim). 2018 Sep-Oct;12 (5):66-9.
41. Jain P, Nanda Z, Deore R, Gandhi A. Effect of acidic environment and intracanal medicament on push-out bond strength of biodentine and mineral trioxide aggregate plus: an in vitro study. Med Pharm Rep. 2019 Jul;92(3):277-81. [DOI:10.15386/mpr-1057]
42. Prasanthi P, Garlapati R, Nagesh B, Sujana V, Kiran Naik KM, Yamini B. Effect of 17% ethylenediaminetetraacetic acid and 0.2% chitosan on pushout bond strength of biodentine and ProRoot mineral trioxide aggregate: An in vitro study. J Conserv Dent. 2019 Jul-Aug;22(4):387-90. [DOI:10.4103/JCD.JCD_56_19] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
