Journal of Research in Dental
and Maxillofacial Sciences
Volume 7, Issue 4 (10-2022)
J Res Dent Maxillofac Sci 2022, 7(4): 219-225 |
Back to browse issues page


Ethics code: ]IR.MAZUMS.1398.1010
Clinical trials code: 0000
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mesgarani A, Hoshyari N, Mousazadeh M, Kabbazzadeh A. Ex Vivo Comparison of File Fracture and File
Deformation in Canals with Moderate Curvature: Neolix Rotary System versus Manual K-files. J Res Dent Maxillofac Sci 2022; 7 (4) :219-225
URL: http://jrdms.dentaliau.ac.ir/article-1-393-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-393-en.html



1- Department of Endodontics, Sari Dental School, Mazandaran University of Medical Sciences, Sari, Iran
2- Department of Endodontics, Sari Dental School, Mazandaran University of Medical Sciences, Sari, Iran ,narjeshoshyari@rocketmail.com
3- Health Science Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran
4- Private Dentistry Practice, Sari, Iran
2- Department of Endodontics, Sari Dental School, Mazandaran University of Medical Sciences, Sari, Iran ,
3- Health Science Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran
4- Private Dentistry Practice, Sari, Iran
Full-Text [PDF 764 kb]
(1548 Downloads)
| Abstract (HTML) (3118 Views)
Introduction
Cleaning and shaping of the canal are an important step in root canal treatment [1]. Root canals are shaped conical for subsequent obturation [2]. Canal preparation can be performed with hand and rotary endodontic files [3]. However, procedural errors may occur due to file defects or fatigue and affect the success of treatment [4]. Instrument fracture in the canal is among the biggest concerns of dental clinicians, which compromises the treatment outcome [5]. Thus, adequate information about the deformation characteristics of the files during instrumentation is important [6].
Moreover, poor-quality endodontic treatment can cause periapical lesion and treatment failure [7, 8]. Therefore, using flexible instruments can be helpful due to higher risk of procedural errors in cleaning and shaping of curved canals compared with straight canals [9, 10]. Nickel-titanium (NiTi) alloy was introduced to endodontics in 1988 [11]. Unlike stainless steel files, NiTi files are super elastic and can be used in curved canals; they return to their original state after filing and do not undergo permanent deformation [12-15]. Deformation of less than 10% is reversible in NiTi instruments, while this value is 1% in ordinary alloys. In addition, using NiTi instruments reduces the preparation time of the root canal space and canal transportation [16, 17]. Despite their benefits, rotary files have some disadvantages, including locking in the canal, creating high stress and microcracks in the root, file fatigue, and high cost [18].
Furthermore, several studies have reported the possibility of rotary file fracture [19-20].
Although studies have shown that events such as zipping or canal transportation occur less frequently when using NiTi rotary files, compared with manual stainless steel files, it is generally presumed that the frequency of file fracture in rotary files is more than that in manual files [21-23].
The Neolix rotary system (Neolix Co., France) has two models. The first one is Neoniti C1 (size: 25, taper at the tip: 12%, length: 15 mm, rectangular cross-section) which is used to open and dilate the root canal with the rotational speed of 300-500 rpm and 1.5 N/cm torque. The second one is Neoniti A1 (sizes 20 and 25 with the taper at the tip of 8%, size 40 with the taper at the tip of 4%, and length of 25 mm), which is used for root canal preparation to the apical part of the root canal. This file has a non-cutting rounded tip.
Moreover, it has appropriate flexibility throughout the working length, and precisely prepares the curved canals while maintaining the original canal anatomy [24].
Factors such as dentist’s high level of expertise and use of modern instruments and techniques for cleaning and shaping of the canal lead to successful root canal treatment [25]. Despite a lot of studies, one cannot prefer one single method over others with ideal results [26]. Although previous studies have mentioned the advantages of Neolix rotary system, there are some contradictions [27]. Procedural errors in the course of treatment should be prevented to improve the prognosis of treatment [28]. Thus, this study aimed to investigate the fracture rate of Neolix rotating files and the manual K-files in the mesiobuccal canal of maxillary first molars with moderate curvature.
Materials and Methods
This ex-vivo experimental study was conducted on 60 extracted teeth collected from Sari Clinics [29]. The study was approved by the ethics committee of Sari University of Medical Sciences (IR.MAZUMS.REC.1398.1010). The inclusion criteria were: 1) mature roots with closed apices, 2) moderate canal curvature (5-25°), 3) canals types I, II, and III, 4) roots with no caries and resorption, and 5) apical patency as large as a #15 file. The exclusion criteria were: 1) roots with immature apex, 2) extensive root caries, 3) dilacerations, 4) curvature in more than one direction, and 5) evidence of internal resorption [29]. The degree of root curvature was determined using the Schneider’s method [30]. First, periapical radiographic images were obtained from the teeth. On the radiograph, a straight line was drawn along the longitudinal axis of the canal from the orifice; the point where the canal deviated from this line was called point A. Then, a second line was drawn from the apical foramen to point A. The angle between these two lines, measured with a protractor, determined the curvature angle. Root curvature was categorized into three grades: slight curvature (less than 5°), moderate curvature (5-25°), and severe curvature (25-70°) [30].
Radiographs were assessed for canal resorption or curvature in more than one direction, and other anomalies. Such teeth were excluded from the study. The teeth included in the study were divided into two groups: 30 in the manual K-file group and 30 in the rotary file group. To disinfect the teeth and remove the attached soft tissues, they were immersed in 5.25% sodium hypochlorite for one hour. Then, they were stored in saline at room temperature until the experiment [29].
First, access cavity was prepared using a fissure diamond bur, and the orifice of the canals was negotiated with an endo explorer. The patency in each canal was confirmed with a #10 file. Canals in which #10 and #15 K-files got stuck in apical constriction were selected. Then, the crowns were cut with a fissure bur and high-speed handpiece under abundant water spray such that the working length in all teeth was 13 mm from the apical foramen. The working length was visually determined using a #10 K-file. If the tooth had two orifices and one foramen (type II), one canal was evaluated [29].
In this study, teeth were examined in two groups of rotatory (Neolix, France) and manual K-files. (Dentsply, Ballaigues, Switzerland). In the Neolix rotary file group, #15 file was introduced into the mesiobuccal canal of the maxillary first molar to the working length before using the rotary system. Then, C1 rotary file size 25 with 0.12 taper or the orifice shaper was used to shape the orifice and coronal third of the root canal. Then, red A1 file size 25 with 0.08 taper was used with circumferential filing movement to the middle third, and yellow A1 file size 20 with 0.08 taper was used with a pecking motion to the apical third of the working length. After the yellow file reached the working length, the red file was used [31]. Instrumentation was performed with an electric motor and a reduction handpiece with a gear of 1:16 (NSK Endo micro motor, Japan) at the speed of 300 rpm. Before using each file, the instrument was assessed at x8 magnification; it would be excluded from the study and replaced with a functioning instrument if it was defective. After using each file, the canals were irrigated with 1 mL of 2.5% sodium hypochlorite. Patency was confirmed after using each file using a #15 K-file.
In the second group, the mesiobuccal canal of the tooth was cleaned using a manual K-file (Dentsply, Ballaigues, Switzerland) with the passive step-back method. Instrumentation was continued until #25 master apical file. Gates Glidden drills #1 and #2 were used to enlarge the coronal part of the canal. One operator performed all the procedures. The teeth were fixed in a mini clamp to prepare the canal.
Then, the files were cleaned with an alcohol-soaked gauze and inspected with a magnifier at x8 magnification after the preparation of each canal to determine the failure rate of the files in both rotary and manual groups. If the file was defective, another file of the same size replaced it. The length of each file was evaluated after preparation to determine if a minor fracture had occurred at the tip of the file.
Each file was used until fracture or deformation, and the number of cleaned canals by each file was recorded. All files with defects or fractures were recorded by the type and location of the defect. Also, the number of prepared canals until defect occurrence was recorded. The instruments that fractured due to flexural stresses had sharp edges, and there was no trace of plastic deformation in them. Accordingly, the fractured files were divided into two groups of torsional and flexural groups.
The data were first reported using descriptive statistics, including frequency, ratio, and percentage for qualitative data and mean and standard deviation for quantitative data. Then, the data were analyzed by the Mann-Whitney U test using SPSS version 21 at a significance level of 0.05.
Results
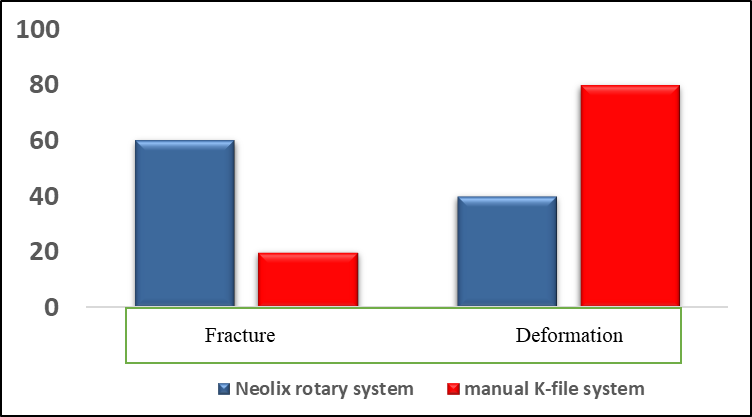
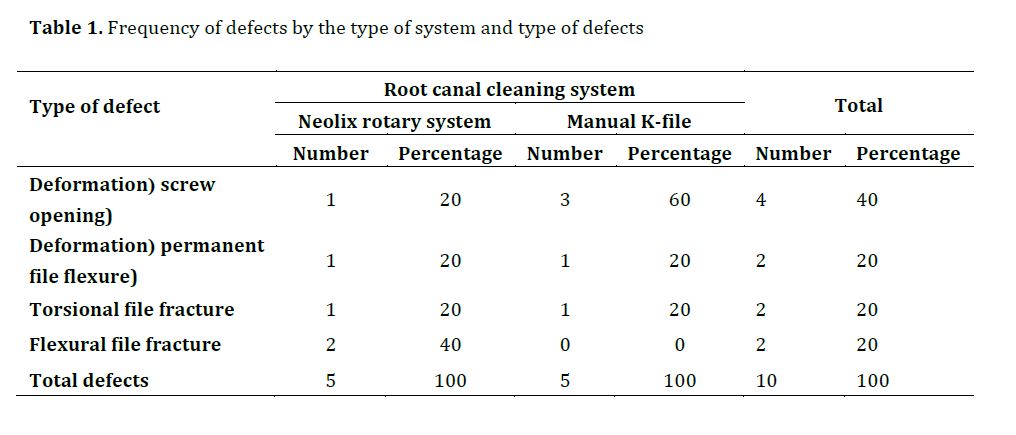
A total of eight manual files (#15, #20, and #25 files) were used to clean 30 canals, and eight rotary files (orifice shaper, red and yellow A1) were utilized to clean and shape the remaining 30 canals. At the end of the preparation (30 canals in each group), 10 instruments had defects; six were deformed in the file flutes, and four had a fracture. Among the defective instruments, five files belonged to the Neolix rotary system group (50%) and five to the manual file group (50%) (Table 1).
Among the six deformed files, four had opening screws (66.6%), and two had irreversible flexure (44.4%), while there were two torsional and two flexural fractures among the four fractured files. In this study, defects occurred in the apical third and middle third (Figure 1).
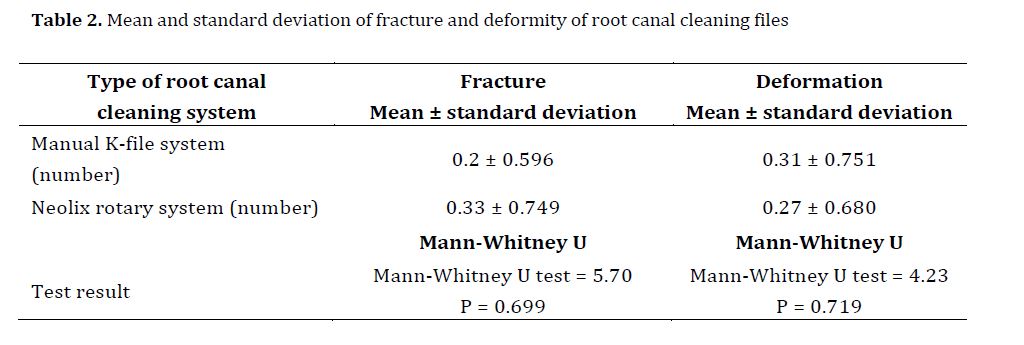
According to Table 2, the results of the Mann-Whitney U test showed no significant difference between the root canal cleaning systems in fracture (P=0.699) or deformation (P=0.719) rate.
Discussion
Full-Text: (1503 Views)
| Abstract
Background and Aim: Cleaning and shaping is one of the important steps in endodontic treatment, which has an important role in root canal treatment outcome. This study evaluated the rate of file fracture and file deformation in Neolix rotary system and K-files in shaping of the mesiobuccal canal of maxillary first molars with moderate curvature. Materials and Methods: In this ex vivo experimental study, the mesiobuccal root curvature of maxillary first molars was measured by the Schneider’s method, and canal preparation was performed in 2 groups of 30 with Neolix rotary system and manual K-files. To determine the fracture rate of files, a file was used until it broke or deformed, and the number of canals cleaned by that file was recorded. The data were analyzed by the Mann-Whitney U test. Results: File fracture rate in the rotary group was slightly higher than that in the manual K-file group but, the frequency of file deformation in manual K-files was slightly more than that in the rotary group. There was no statistically significant relationship between file type and frequency of file fracture or deformation (P>0.05). Conclusion: Manual stainless steel K files and Neolix NiTi rotary files were the same in terms of file fracture and file deformation in preparation of canals with moderate curvature. Key Words: Endodontics; Root Canal Preparation; Equipment Design |
Introduction
Cleaning and shaping of the canal are an important step in root canal treatment [1]. Root canals are shaped conical for subsequent obturation [2]. Canal preparation can be performed with hand and rotary endodontic files [3]. However, procedural errors may occur due to file defects or fatigue and affect the success of treatment [4]. Instrument fracture in the canal is among the biggest concerns of dental clinicians, which compromises the treatment outcome [5]. Thus, adequate information about the deformation characteristics of the files during instrumentation is important [6].
Moreover, poor-quality endodontic treatment can cause periapical lesion and treatment failure [7, 8]. Therefore, using flexible instruments can be helpful due to higher risk of procedural errors in cleaning and shaping of curved canals compared with straight canals [9, 10]. Nickel-titanium (NiTi) alloy was introduced to endodontics in 1988 [11]. Unlike stainless steel files, NiTi files are super elastic and can be used in curved canals; they return to their original state after filing and do not undergo permanent deformation [12-15]. Deformation of less than 10% is reversible in NiTi instruments, while this value is 1% in ordinary alloys. In addition, using NiTi instruments reduces the preparation time of the root canal space and canal transportation [16, 17]. Despite their benefits, rotary files have some disadvantages, including locking in the canal, creating high stress and microcracks in the root, file fatigue, and high cost [18].
Furthermore, several studies have reported the possibility of rotary file fracture [19-20].
Although studies have shown that events such as zipping or canal transportation occur less frequently when using NiTi rotary files, compared with manual stainless steel files, it is generally presumed that the frequency of file fracture in rotary files is more than that in manual files [21-23].
The Neolix rotary system (Neolix Co., France) has two models. The first one is Neoniti C1 (size: 25, taper at the tip: 12%, length: 15 mm, rectangular cross-section) which is used to open and dilate the root canal with the rotational speed of 300-500 rpm and 1.5 N/cm torque. The second one is Neoniti A1 (sizes 20 and 25 with the taper at the tip of 8%, size 40 with the taper at the tip of 4%, and length of 25 mm), which is used for root canal preparation to the apical part of the root canal. This file has a non-cutting rounded tip.
Moreover, it has appropriate flexibility throughout the working length, and precisely prepares the curved canals while maintaining the original canal anatomy [24].
Factors such as dentist’s high level of expertise and use of modern instruments and techniques for cleaning and shaping of the canal lead to successful root canal treatment [25]. Despite a lot of studies, one cannot prefer one single method over others with ideal results [26]. Although previous studies have mentioned the advantages of Neolix rotary system, there are some contradictions [27]. Procedural errors in the course of treatment should be prevented to improve the prognosis of treatment [28]. Thus, this study aimed to investigate the fracture rate of Neolix rotating files and the manual K-files in the mesiobuccal canal of maxillary first molars with moderate curvature.
Materials and Methods
This ex-vivo experimental study was conducted on 60 extracted teeth collected from Sari Clinics [29]. The study was approved by the ethics committee of Sari University of Medical Sciences (IR.MAZUMS.REC.1398.1010). The inclusion criteria were: 1) mature roots with closed apices, 2) moderate canal curvature (5-25°), 3) canals types I, II, and III, 4) roots with no caries and resorption, and 5) apical patency as large as a #15 file. The exclusion criteria were: 1) roots with immature apex, 2) extensive root caries, 3) dilacerations, 4) curvature in more than one direction, and 5) evidence of internal resorption [29]. The degree of root curvature was determined using the Schneider’s method [30]. First, periapical radiographic images were obtained from the teeth. On the radiograph, a straight line was drawn along the longitudinal axis of the canal from the orifice; the point where the canal deviated from this line was called point A. Then, a second line was drawn from the apical foramen to point A. The angle between these two lines, measured with a protractor, determined the curvature angle. Root curvature was categorized into three grades: slight curvature (less than 5°), moderate curvature (5-25°), and severe curvature (25-70°) [30].
Radiographs were assessed for canal resorption or curvature in more than one direction, and other anomalies. Such teeth were excluded from the study. The teeth included in the study were divided into two groups: 30 in the manual K-file group and 30 in the rotary file group. To disinfect the teeth and remove the attached soft tissues, they were immersed in 5.25% sodium hypochlorite for one hour. Then, they were stored in saline at room temperature until the experiment [29].
First, access cavity was prepared using a fissure diamond bur, and the orifice of the canals was negotiated with an endo explorer. The patency in each canal was confirmed with a #10 file. Canals in which #10 and #15 K-files got stuck in apical constriction were selected. Then, the crowns were cut with a fissure bur and high-speed handpiece under abundant water spray such that the working length in all teeth was 13 mm from the apical foramen. The working length was visually determined using a #10 K-file. If the tooth had two orifices and one foramen (type II), one canal was evaluated [29].
In this study, teeth were examined in two groups of rotatory (Neolix, France) and manual K-files. (Dentsply, Ballaigues, Switzerland). In the Neolix rotary file group, #15 file was introduced into the mesiobuccal canal of the maxillary first molar to the working length before using the rotary system. Then, C1 rotary file size 25 with 0.12 taper or the orifice shaper was used to shape the orifice and coronal third of the root canal. Then, red A1 file size 25 with 0.08 taper was used with circumferential filing movement to the middle third, and yellow A1 file size 20 with 0.08 taper was used with a pecking motion to the apical third of the working length. After the yellow file reached the working length, the red file was used [31]. Instrumentation was performed with an electric motor and a reduction handpiece with a gear of 1:16 (NSK Endo micro motor, Japan) at the speed of 300 rpm. Before using each file, the instrument was assessed at x8 magnification; it would be excluded from the study and replaced with a functioning instrument if it was defective. After using each file, the canals were irrigated with 1 mL of 2.5% sodium hypochlorite. Patency was confirmed after using each file using a #15 K-file.
In the second group, the mesiobuccal canal of the tooth was cleaned using a manual K-file (Dentsply, Ballaigues, Switzerland) with the passive step-back method. Instrumentation was continued until #25 master apical file. Gates Glidden drills #1 and #2 were used to enlarge the coronal part of the canal. One operator performed all the procedures. The teeth were fixed in a mini clamp to prepare the canal.
Then, the files were cleaned with an alcohol-soaked gauze and inspected with a magnifier at x8 magnification after the preparation of each canal to determine the failure rate of the files in both rotary and manual groups. If the file was defective, another file of the same size replaced it. The length of each file was evaluated after preparation to determine if a minor fracture had occurred at the tip of the file.
Each file was used until fracture or deformation, and the number of cleaned canals by each file was recorded. All files with defects or fractures were recorded by the type and location of the defect. Also, the number of prepared canals until defect occurrence was recorded. The instruments that fractured due to flexural stresses had sharp edges, and there was no trace of plastic deformation in them. Accordingly, the fractured files were divided into two groups of torsional and flexural groups.
The data were first reported using descriptive statistics, including frequency, ratio, and percentage for qualitative data and mean and standard deviation for quantitative data. Then, the data were analyzed by the Mann-Whitney U test using SPSS version 21 at a significance level of 0.05.
Results
A total of eight manual files (#15, #20, and #25 files) were used to clean 30 canals, and eight rotary files (orifice shaper, red and yellow A1) were utilized to clean and shape the remaining 30 canals. At the end of the preparation (30 canals in each group), 10 instruments had defects; six were deformed in the file flutes, and four had a fracture. Among the defective instruments, five files belonged to the Neolix rotary system group (50%) and five to the manual file group (50%) (Table 1).
Among the six deformed files, four had opening screws (66.6%), and two had irreversible flexure (44.4%), while there were two torsional and two flexural fractures among the four fractured files. In this study, defects occurred in the apical third and middle third (Figure 1).
According to Table 2, the results of the Mann-Whitney U test showed no significant difference between the root canal cleaning systems in fracture (P=0.699) or deformation (P=0.719) rate.
{kind=link}
Table 1. Frequency of defects by the type of system and type of defects
Table 2. Mean and standard deviation of fracture and deformity of root canal cleaning files
{kind=link}
Table 2. Mean and standard deviation of fracture and deformity of root canal cleaning files
{kind=link}
Discussion
Similar to other dental procedures, endodontic treatment is occasionally associated with unwanted and unforeseen events, called procedural errors. Knowledge about the causes of these errors is essential to prevent them [16]. Unfortunately, the process of cleaning and shaping of the canal, especially the curved canals, is not always without problems. Various studies have reported deviation of the canal path, occurrence of apical perforation, access cavity perforation, and instrument fracture within the canal [26,27,31]. Preparing an access cavity along a straight line, pre-curving of the files, and using them passively are strategies that can prevent procedural errors [32-34].
Manual files, existing in different forms and designs, are undoubtedly the most widely used manual instruments in canal preparation. These files are made of stainless steel and NiTi alloys. Considering the new technology of rotary file systems and their diversity, this study investigated the fracture rate of Neolix rotary files and manual K-files in the mesiobuccal canal of maxillary first molars with moderate curvature.
In this study, canal preparation was performed up to master apical file size 25 in the manual file group; this is appropriate in terms of safety and reducing errors such as transportation, ledge formation, or canal perforation [34].
The results of the present study showed that the frequency of file fracture was slightly higher in the rotary group compared with the manual K-file (10% vs. 3.3%), although no statistically significant difference was found in this study.
Nagaratna et al. [35] compared stainless steel hand instruments and NiTi rotary instruments in root canal preparation of permanent and primary molars. They observed that 40% of the manual files in deciduous teeth and 30% of manual files in permanent teeth became deformed, although they did not fracture. In contrast, 10% of the rotary files used in deciduous teeth and 20% of the rotary files used in permanent teeth fractured. Their results contradicted the results of the present study, which can be due to differences in the types of rotary files and the teeth. On the other hand, Parvathaneni et al. [36]
compared canal preparation with stainless steel and NiTi hand and NiTi engine-driven instruments. They examined 50 extracted molar teeth and used 15 files from each file series. After implementing the treatment, they reported one stainless steel file fracture and one permanent file deformity. Moreover, there was a file fracture in the NiTi rotary instrument group. Finally, they revealed that NiTi rotary files had lower failure rate compared with stainless steel hand files, although it was not statistically significant. This finding was in line with the present results. In another study on 100 general dentists and 100 endodontists in Tehran, Mozayeni et al. [37] found that the most common errors occurring following the application of rotary files were file fracture (88.5%), canal transportation (76.5%), and ledge formation (68%).
Conclusion
It can be concluded that both hand K files and Neolix rotary files are similar in case of file fracture and deformation; thus, they both can be used for instrumentation and may be expected to have comparable rate of procedural errors.
Manual files, existing in different forms and designs, are undoubtedly the most widely used manual instruments in canal preparation. These files are made of stainless steel and NiTi alloys. Considering the new technology of rotary file systems and their diversity, this study investigated the fracture rate of Neolix rotary files and manual K-files in the mesiobuccal canal of maxillary first molars with moderate curvature.
In this study, canal preparation was performed up to master apical file size 25 in the manual file group; this is appropriate in terms of safety and reducing errors such as transportation, ledge formation, or canal perforation [34].
The results of the present study showed that the frequency of file fracture was slightly higher in the rotary group compared with the manual K-file (10% vs. 3.3%), although no statistically significant difference was found in this study.
Nagaratna et al. [35] compared stainless steel hand instruments and NiTi rotary instruments in root canal preparation of permanent and primary molars. They observed that 40% of the manual files in deciduous teeth and 30% of manual files in permanent teeth became deformed, although they did not fracture. In contrast, 10% of the rotary files used in deciduous teeth and 20% of the rotary files used in permanent teeth fractured. Their results contradicted the results of the present study, which can be due to differences in the types of rotary files and the teeth. On the other hand, Parvathaneni et al. [36]
compared canal preparation with stainless steel and NiTi hand and NiTi engine-driven instruments. They examined 50 extracted molar teeth and used 15 files from each file series. After implementing the treatment, they reported one stainless steel file fracture and one permanent file deformity. Moreover, there was a file fracture in the NiTi rotary instrument group. Finally, they revealed that NiTi rotary files had lower failure rate compared with stainless steel hand files, although it was not statistically significant. This finding was in line with the present results. In another study on 100 general dentists and 100 endodontists in Tehran, Mozayeni et al. [37] found that the most common errors occurring following the application of rotary files were file fracture (88.5%), canal transportation (76.5%), and ledge formation (68%).
Conclusion
It can be concluded that both hand K files and Neolix rotary files are similar in case of file fracture and deformation; thus, they both can be used for instrumentation and may be expected to have comparable rate of procedural errors.
Type of Study: Original article |
Subject:
Endodontics
References
1. Ahangari Z, Rahmani M, Eslami G, Kangarloo A. The effectiveness of Mtwo and step back instrumentation techniques on the elimination of enterococcus faecalis from root canal. Journal of Dental School, Shahid Beheshti University of Medical Science.2011;29(1):87.
2. Abageru A, Pop M, Kovács M, Stoica A, Monea M. Evaluation of the Apical Seal after Root Canal Cleaning and Shaping with Two Nickel-Titanium Systems. Acta Marisiensis - Seria Medica. 2019;65(4): 135-9.
3. Parashos P, Messer HH. Questionnaire survey on the use of rotary nickel-titanium endodontic instruments by Australian dentists. Int Endod J. 2004 Apr;37(4):249-59. [DOI:10.1111/j.0143-2885.2004.00784.x] [PMID]
4. Amza O, Dimitriu B, Suciu I, Bartok R, Chirila M. Etiology and Prevention of an Endodontic Iatrogenic Event: Instrument Fracture. J Med Life. 2020 Jul-Sep;13(3):378-81.
5. Di Nardo D, Zanza A, Seracchiani M, Donfrancesco O, Gambarini G, Testarelli L. Angle of Insertion and Torsional Resistance of Nickel-Titanium Rotary Instruments. Materials (Basel). 2021 Jul 4;14(13):3744. [DOI:10.3390/ma14133744] [PMID] [PMCID]
6. Khalil W, Alghamdi F. Fracture and deformation rate of Protaper next file among postgraduate students. Egyptian Dental Journal. 2019April; 65(2):1559-66. [DOI:10.21608/edj.2019.72580]
7. Boucher Y, Matossian L, Rilliard F, Machtou P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int Endod J. 2002 Mar;35(3):229-38. [DOI:10.1046/j.1365-2591.2002.00469.x] [PMID]
8. Kirkevang LL, Hörsted-Bindslev P, Orstavik D, Wenzel A. A comparison of the quality of root canal treatment in two Danish subpopulations examined 1974-75 and 1997-98. Int Endod J. 2001 Dec;34(8):607-12. [DOI:10.1046/j.1365-2591.2001.00436.x] [PMID]
9. Kwak SW, Ha JH, Shen Y, Haapasalo M, Kim HC. Effects of Root Canal Curvature and Mechanical Properties of Nickel-Titanium Files on Torque Generation. J Endod. 2021 Sep;47(9):1501-6. [DOI:10.1016/j.joen.2021.06.019] [PMID]
10. Silva EJNL, Vieira VTL, Hecksher F, Dos Santos Oliveira MRS, Dos Santos Antunes H, Moreira EJL. Cyclic fatigue using severely curved canals and torsional resistance of thermally treated reciprocating instruments. Clin Oral Investig. 2018 Sep;22(7):2633-8. [DOI:10.1007/s00784-018-2362-9] [PMID]
11. Funaki H, Ozeki R. y. International Journal of Oral-Medical Sciences. 2020 Jun 3;19(1):44-9. [DOI:10.5466/ijoms.19.44]
12. Kum KY, Spängberg L, Cha BY, Il-Young J, Msd, Seung-Jong L, Chan-Young L. Shaping ability of three ProFile rotary instrumentation techniques in simulated resin root canals. J Endod. 2000 Dec;26(12):719-23. [DOI:10.1097/00004770-200012000-00013] [PMID]
13. Rhodes JS, Ford TR, Lynch JA, Liepins PJ, Curtis RV. A comparison of two nickel-titanium instrumentation techniques in teeth using microcomputed tomography. Int Endod J. 2000 May;33(3):279-85. [DOI:10.1046/j.1365-2591.1999.00306.x] [PMID]
14. Tabassum S, Zafar K, Umer F. Nickel-Titanium Rotary File Systems: What's New? Eur Endod J. 2019 Oct 18;4(3):111-7.
15. Harshavardhan J M, Dhanavel C, Vijayaraja S, Manoj KT, Bakkiyalakshmi A, Sitharthan K. Metallurgy of Rotary Files-A Review. Journal of Current Medical Research and Opinion. 2021 Jun 21;4(6):975-80.
16. Kumar S, Kumar A, Marandi L, Sen I. Assessment of small-scale deformation characteristics and stress-strain behavior of NiTi based shape memory alloy using nanoindentation. Acta Materialia. 2020 Dec 1;201:303-15. [DOI:10.1016/j.actamat.2020.09.080]
17. Vaudt J, Bitter K, Neumann K, Kielbassa AM. Ex vivo study on root canal instrumentation of two rotary nickel-titanium systems in comparison to stainless steel hand instruments. Int Endod J. 2009 Jan;42(1):22-33. [DOI:10.1111/j.1365-2591.2008.01489.x] [PMID]
18. Ruiz X, Karanam KD. Rotary Endodontics: A Brief Review. MAR Dental Sciences. 2021 Apr 1;2(4):1-10.
19. Gomes MS, Vieira RM, Böttcher DE, Plotino G, Celeste RK, Rossi-Fedele G. Clinical fracture incidence of rotary and reciprocating NiTi files: A systematic review and meta-regression. Aust Endod J. 2021 Aug;47(2):372-85. [DOI:10.1111/aej.12484] [PMID]
20. Seracchiani M, Miccoli G, Di Nardo D, Zanza A, Cantore M, Gambarini G, Testarelli L. Effect of Flexural Stress on Torsional Resistance of NiTi Instruments. J Endod. 2021 Mar;47(3):472-6. [DOI:10.1016/j.joen.2020.10.011] [PMID]
21. Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod. 2006 Nov;32(11):1031-43. [DOI:10.1016/j.joen.2006.06.008] [PMID]
22. Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-titanium endodontic instruments after clinical use. J Endod. 2004 Oct;30(10):722-5. [DOI:10.1097/01.DON.0000129963.42882.C9] [PMID]
23. Alapati SB, Brantley WA, Svec TA, Powers JM, Nusstein JM, Daehn GS. SEM observations of nickel-titanium rotary endodontic instruments that fractured during clinical Use. J Endod. 2005 Jan;31(1):40-3. [DOI:10.1097/01.DON.0000132301.87637.4A] [PMID]
24. Rabie MI, Hassan HY, Elshaboury EI. Cleanliness Efficacy of Neolix and Silk Rotary Systems in Root Canal Retreatment. Egyptian Dental Journal. 2019 Jul;65(3):2795-800. [DOI:10.21608/edj.2019.72657]
25. Fariniuk LF, Baratto-Filho F, Guerisoli DM, Barbizam JV, Pécora JD, Sousa-Neto MD. Modeling capacity of ENDOflash files in simulated root canals. Braz Dent J. 2001;12(1):39-42.
26. Harandi A, Mirzaeerad S, Mehrabani M, Mahmoudi E, Bijani A. Incidence of dentinal crack after root canal preparation by ProTaper universal, Neolix and SafeSider systems. Iran Endod J. 2017;12(4):432-8.
27. Gayatri K, Tammineedi S, Bolla N, Vemuri S, Basam RC, Sunil CR. Effect of autoclaving on the cyclic fatigue resistance of nickel-titanium rotary instruments: An in vitro study. J Conserv Dent. 2021 Sep-Oct;24(5):440-4. [DOI:10.4103/jcd.jcd_182_21] [PMID] [PMCID]
28. Khoshbin E, Donyavi Z, Abbasi Atibeh E, Roshanaei G, Amani F. The Effect of Canal Preparation with Four Different Rotary Systems on Formation of Dentinal Cracks: An In Vitro Evaluation. Iran Endod J. 2018 Spring;13(2):163-8.
29. Zarabi M, Javidi M, Mesgarani A, Poursattar Bageh Mir A. Number of Severely Curved Root Canals Preparation Leading to either Defect or Fracture using three Rotary Systems. Journal of Dentistry. 2011;12(3):252-60.
30. Balani P, Niazi F, Rashid H. A brief review of the methods used to determine the curvature of root canals. Journal of Restorative Dentistry. 2015;3(4):57-63. [DOI:10.4103/2321-4619.168733]
31. Kuzekanani M, Sadeghi F, Hatami N, Rad M, Darijani M, Walsh LJ. Comparison of Canal Transportation, Separation Rate, and Preparation Time between One Shape and Neoniti (Neolix): An In Vitro CBCT Study. Int J Dent. 2021 Sep 7; 2021:6457071. [DOI:10.1155/2021/6457071] [PMID] [PMCID]
32. Moushekhian, S., Bagheri, H., Shahabi, A., Forghani, M. Laboratory Evaluation of Fracture and Deformation in ProTaper Universal and Neoniti Rotary Files. Journal of Mashhad Dental School. 2016; 40(4): 381-8.
33. Sivakumar P, Ganapathy D. Prevalence of perforation in root canal treatment and knowledge of management among undergraduate students. J Pharm Sci Res. 2020:12(2);310-3.
34. Yancheshmeh SS. Examining the Factors Affecting Endodontic Therapy Failure. J Mol Biol Res. 2020 March; 10 (1):1-5. [DOI:10.5539/jmbr.v10n1p1]
35. Nagaratna PJ, Shashikiran ND, Subbareddy VV. In vitro comparison of NiTi rotary instruments and stainless steel hand instruments in root canal preparations of primary and permanent molar. J Indian Soc Pedod Prev Dent. 2006 Dec;24(4):186-91. [DOI:10.4103/0970-4388.28075] [PMID]
36. Parvathaneni K, Goel B, Parvathaneni BD. A comparison of root canal preparations using stainless steel, Ni-Ti hand, and Ni-Ti engine-driven endodontic instruments-an in vitro study. Bangladesh Journal of Medical Science. 2010 December;9(4):223-30. [DOI:10.3329/bjms.v9i4.6689]
37. Mozayeni M, Golshah A, Nik Kerdar N. A survey on NiTi rotary instruments usage by endodontists and general dentist in Tehran. Iran Endod J 2012; 6(4):168-75.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |