Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 144-153 |
Back to browse issues page


Ethics code: no
Clinical trials code: no
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mahmoudian S, Farhadi S, Hosseinzadeh M. Management of Patients with Concomitant
Somatosensory Tinnitus and Temporomandibular Disorder: A Case Series. J Res Dent Maxillofac Sci 2023; 8 (2) :144-153
URL: http://jrdms.dentaliau.ac.ir/article-1-391-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-391-en.html



1- Head and Neck Research Center, Haz-rat Rasoul Akram Hospital; The Five Senses Health Institute, Iran University of Medical Sciences, Teh-ran, Iran
2- Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Tehran Islamic Azad Medical Sciences University, Tehran, Iran ,dr.sfarhadi@gmail.com
3- Private Dental Practice, Tehran, Iran
2- Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Tehran Islamic Azad Medical Sciences University, Tehran, Iran ,
3- Private Dental Practice, Tehran, Iran
Keywords: Tinnitus, Temporomandibular Joint Disorders, Temporomandibular Joint Dysfunction Syndrome, Somatosensory Disorders
Full-Text [PDF 600 kb]
(1505 Downloads)
| Abstract (HTML) (3725 Views)
Full-Text: (1606 Views)
Abstract
Background and Aim: Multiple studies have shown the common co-occurrence of tinnitus and temporomandibular disorders (TMDs). This study assessed the effectiveness of a conservative treatment for TMD signs and symptoms of six patients with tinnitus-related complaints.
Materials and Methods: Six patients with persistent non-pulsatile tinnitus were evaluated in this case series. The tinnitus characteristics evaluated included pitch and loudness matching (PMT-LMT), minimum masking level (MML), and residual inhibition (RI). In addition, the Persian versions of the 52-item Tinnitus Questionnaire (TQ), the Tinnitus Handicap Inventory (THI), and the Steigerwald/Maher TMD Disability Index (SMTDI) were used. The corresponding TMD treatment plan was subsequently implemented, taking into account the subtype of the disease. The data were statistically analyzed at 0.05 level of significance.
Materials and Methods: Six patients with persistent non-pulsatile tinnitus were evaluated in this case series. The tinnitus characteristics evaluated included pitch and loudness matching (PMT-LMT), minimum masking level (MML), and residual inhibition (RI). In addition, the Persian versions of the 52-item Tinnitus Questionnaire (TQ), the Tinnitus Handicap Inventory (THI), and the Steigerwald/Maher TMD Disability Index (SMTDI) were used. The corresponding TMD treatment plan was subsequently implemented, taking into account the subtype of the disease. The data were statistically analyzed at 0.05 level of significance.
Results: The mean SMTDI score significantly decreased after treatment (P=0.0001) and the symptoms of TMD effectively resolved. Comparison of visual analog scale (VAS) scores of tinnitus patients before and after TMD therapy indicated statistically significant changes (P<0.05) in intensity, irritation, and awareness. Comparison of the mean tinnitus evaluation test scores before and after TMD therapy in tinnitus patients indicated a significant change only in PMT (P=0.039). Comparison of THI and TQ scores before and after TMD therapy revealed significant changes in tinnitus patients (P<0.05).
Conclusion: In case of correct selection of patients with concurrent somatosensory tinnitus and TMD signs and symptoms, TMD therapy might alleviate this condition, according to the present findings. Consequently, a multidisciplinary approach may be useful in treatment of such cases.
Conclusion: In case of correct selection of patients with concurrent somatosensory tinnitus and TMD signs and symptoms, TMD therapy might alleviate this condition, according to the present findings. Consequently, a multidisciplinary approach may be useful in treatment of such cases.
Key Words: Tinnitus; Temporomandibular Joint Disorders; Temporomandibular Joint Dysfunction Syndrome; Somatosensory Disorders
Introduction
Tinnitus is defined as perception of sound in absence of an external or environmental acoustic stimulus. It is often characterized as one sound or collection of noises [1] and might be experienced in one ear, both ears, or the patient's head [2]. The prevalence of tinnitus in adults varies from 10% to 15% [3], and it approaches 18% in those >60 years old [4].
According to a previous study, the prevalence of this ailment in the Iranian population is 4.6%, i.e., 6.4% and 14.6% among individuals in their sixth and seventh decades of life, and 16.8% among those >70 years old [5]. In addition to the impacts of the central auditory neurons, the majority of patients also suffer from subjective tinnitus alterations due to the somatosensory system. These individuals may alter volume and pitch by contraction of their neck, head, or oral muscles [6]. In addition to hearing loss or noise stress, somatic or somatosensory system abnormalities of the cervical spines or the temporomandibular joints (TMJ) may cause tinnitus [7, 8]. This may account for the common co-occurrence of tinnitus and temporomandibular joint disorder (TMD) syndrome reported in a number of studies [9-13]. Manfredini et al. [14] in their study on individuals with TMD, observed a prevalence rate of 30.4% for tinnitus. In addition, Lam et al. [10] found that 64% of individuals presenting with tinnitus had TMD. Buergers et al. [11] reported that people with this condition were eight times more likely to have tinnitus than those without it. The experience of tinnitus may change by firmly clenching the teeth [3]. Also, 36-43% of the population with subjective tinnitus have been reported to have somatic or somatosensory tinnitus. Evidence shows that effective treatment of TMD may alleviate the perception of tinnitus. Therefore, conservative therapy based on scientific data should target the multifaceted etiology of TMD. TMD should be treated with a multidisciplinary approach because numerous biological, psychological, and social factors are involved in its onset and progression [15]. In addition, patients must be educated about the potential causes of this disorder, and they must recognize their vital role in its management [16]. Each patient's therapy should be customized depending on the diagnosis and cause. Dentists and physical therapists may provide such patients with multimodal, customized, and conservative treatment [17]. Moreover, Sherman and Turk [18] observed that TMD therapy led to substantial improvements when paired with psychological therapies as opposed to traditional dental care alone, indicating that psychological components should be included in TMD treatments [18]. Similarly, Aggarwal et al. [19] observed that a complete treatment strategy integrating cognitive behavior therapy, postural control, and biofeedback might give participants with orofacial pain longer-lasting pain alleviation than standard care. Collectively, these data suggest that the diagnosis and treatment of TMD need a complex and interdisciplinary approach. Therefore, the purpose of the current study was to evaluate the effectiveness of conservative TMJ therapy in six patients with tinnitus by identifying their TMD signs and symptoms and documenting their improvements in the studied indices.
Materials and Methods
The patients in this case series had persistent subjective tinnitus and were selected among those referred to Tehran Tinnitus Center. Six male patients with chronic non-pulsatile tinnitus (duration > 6 months) and a mean age of 45.34 ±9.57 years were included in this study [20]. The patients had not received any treatment for their medical condition or therapeutic interventions on their brain or ears (e.g., acoustic, electrical, etc.) for 3 months prior to the onset of this study.
Patients who were evaluated in this study had no history of neurological conditions, head injuries, or brain tumor and had a definite diagnosis of chronic subjective idiopathic tinnitus (duration: > 6 months) confirmed by an audiologist and an otorhinolaryngologist. They also had normal external and middle ear function confirmed by otoscopy and tympanometry and the ability to read, speak, and write in Persian, and consented to participation in the study and completion of follow-ups. In addition, the participants had no history of chronic neurological or auditory diseases, had not taken neurological/psychiatric medications within the past three months, no pregnancy or nursing, no treatment for tinnitus within the past 3 months, no alcohol consumption or drug abuse, no head and neck diseases or space-occupying lesions, and their tinnitus was not secondary to a systemic medical condition. All patients were informed about the study and signed informed consent forms before the experiment.
Measurements and evaluations:
A complete medical history was taken from each patient and all patients underwent physical and psychological evaluations. All patients also underwent subjective and objective assessments for tinnitus prior to receiving TMD therapy. The magnetic resonance imaging gadolinium contrast medium indicated that there were no identifiable abnormalities in the temporal lobe or brain of the individuals. In situations of bilateral tinnitus, the dominant side with more severe symptoms was evaluated. In participants whose complaints were identical on both sides, measures from both ears were included in the study. All patients underwent audiological evaluations (i.e., pure tone audiometry and tympanometry) and tinnitus-related psychoacoustic measurements (i.e., pitch and loudness matching).
Tinnitus psychoacoustic assessments:
The diagnostic characteristics for tinnitus were examined using a clinical audiometer (Madsen®Astera2, Natus) with two channels for recreating the most bothersome tinnitus (MTT) at the same frequency and intensity. The pitch matching and loudness matching of tinnitus (PMT-LMT), minimum masking level (MML), and residual inhibition (RI) factors of tinnitus were evaluated. The precision of the equipment calibration met the American National Standard Specification for Audiometers tolerance requirements (Accuracy no.: #S3.6-200412). All participants' tinnitus parameters were assessed both before and after TMD treatment. For the PMT examination, a forced-choice format with two options was used. For this objective, multiple pairs of pitch sounds were created at 11 frequencies ranging from 125 Hz to 12 kHz. The pitch was then lowered or raised, and the participants were asked to identify which pitch best matched their tinnitus. Lastly, an octave confusion test was utilized to establish the frequency of tinnitus more precisely. Before presenting each pair, the loudness levels of tone pairs were modified to match those of the tinnitus. The LMT was also determined for each test tone in the PMT technique, after which the subject's auditory threshold at that particular frequency (A) was raised in 1-dB increments until they reported that the external tone was as loud as the tinnitus (B). Subsequently, the sound volume was adjusted in 1-dB increments to achieve a threshold somewhat higher than the tinnitus threshold (C). The mean level of loudness between (B) and (C) represented the volume of the tinnitus. This formula calculated the volume (expressed in decibels of the feeling level43):
Loudness of tinnitus=[(B+C)/2–A](dB SL) [20]
The MML was further assessed by the narrow-band noise in the afflicted ear until the tinnitus was completely masked. The RI was then measured using a narrow-band noise with an intensity of 10 dB greater than MML for 60 seconds. Importantly, tinnitus may be temporarily muted by an adequate masking stimulus, also known as RI. After the stimulus is deactivated, one of the following outcomes may occur: full RI (CRI), partial RI (PRI), non-residual inhibition (NRI), and lastly rebound effect (RF, or facilitated tinnitus), resulting in an increase in the loudness of tinnitus as experienced by the individuals. CRI is the condition in which tinnitus remains inaudible even after removing the masking stimuli. PRI also refers to a condition in which tinnitus is diminished but remains audible to the sufferer. When the tinnitus remains intact after the cessation of masking stimuli, this condition is known as NRI. In addition, the increase in the volume of tinnitus that occurs after turning off masking stimuli is known as the RF phenomenon [20].
Self-report tinnitus questionnaires:
The 52-item Tinnitus Questionnaire (TQ) [20-22], originally created by Hallam, was used in order to assess the behavioral side effects of tinnitus. The questionnaire has a Cronbach's alpha value of 0.95 and a test-retest reliability of 0.91 to 0.94 [15]. The subscales of the TQ comprised auditory-perceptual difficulties, intrusiveness, sleep issues, physical symptoms, and emotional and cognitive abnormalities. The Tinnitus Handicap Inventory (THI) [22,23], which was originally developed by Newman et al. [23] and consists of 25 questions, was then used to characterize the functional, emotional, and catastrophic implications of tinnitus on the patients' everyday life. This version was easy to administer and interpret as a very effective psychometric instrument. Currently, it is also used in other health/treatment facilities globally. The THI item analysis revealed that this self-report questionnaire has great internal consistency and sufficient convergent and construct validity. The THI scores were classified as 0–16 for mild, 18–36 for moderate, 38–56 for severe, 58–76 for severe, and 78–100 for suffering.
Visual analogue scale (VAS):
This questionnaire is a certified psychometric response scale which can be used to assess the effect of tinnitus on ordinary everyday living in terms of severity, irritation, and awareness. Responding to the VAS, respondents ranked the loudness, irritation, and disruption of tinnitus on a continuum from 0 to 10.
TMD evaluation:
The assessed patients completed the Steigerwald/Maher TMD Disability Index (SMTDI) [24]. Besides, VAS score for the existing tinnitus was recorded at baseline.
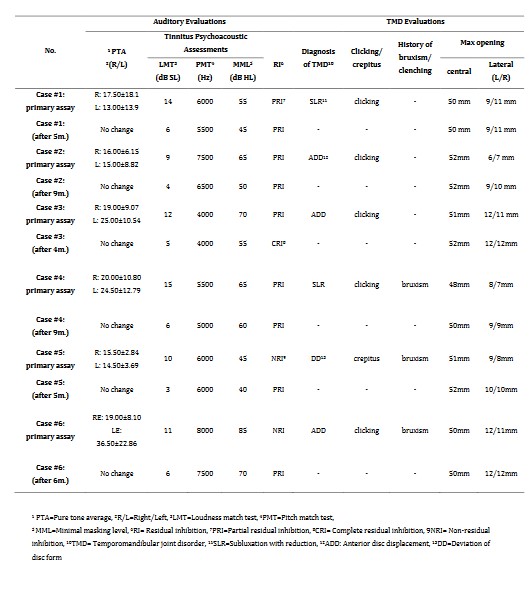
TMD was diagnosed based on symptom evaluation; the most often used diagnostic classification systems were the Research Diagnostic Criteria for TMD and the American Academy of Orofacial Pain classification [12]. The patients were evaluated by noting their TMD signs and symptoms, such as pain and TMJ sounds (i.e., clicking and crepitus), limitation and pain on mouth opening, any mandibular deviation during mouth opening, a history of bruxism and clenching, and measurements of central and lateral opening and evaluation of occlusion parameters, such as central and lateral occlusal contacts. Then, a treatment plan was designed based on the diagnostic data. All six patients were meticulously examined in accordance with the procedure, and their therapy regimens were established using the TMD method to account for the absence or weakness of other causative variables. Upon registration, the TMJ examination, the definitive diagnosis of TMD based on clinical assessment, and the associated subtype of TMD, including "capsulitis, deviation of disc form, anterior disc displacement, and subluxation with or without reduction" were also recorded. None of the subjects tested exhibited TMJ discomfort or tenderness. Two patients were also identified with subluxation with reduction, three patients with anterior disc displacement, and one patient with disc deviation. For each instance, the use of the bite guard (i.e., the flat occlusal splint) with regard to its occlusal adjustment, precise occlusal adjustment of teeth, and exclusive physical treatment, including therapeutic jaw exercise linked to either subtype of existing TMD were planned. Six patients were treated for an average of 8 months. The overview of the principal test and variance of measured parameters for each patient are provided in Table 1.
Results
• TMD Treatment
Two of the six patients evaluated were diagnosed with subluxation with reduction, three with anterior disc displacement, and one with disc deviation. After therapy, clicking and crepitus improved for 7.1 ±0.9 months. After therapy, three patients with a history of bruxism reported no parafunction. The mean SMTDI score decreased from 34.50 ±1.3 to 24.37 ±8.6, and this difference was significant according to paired-samples t-test (P=0.0001). The majority of patients did not have mouth opening limitation; therefore, appropriate room was either already available or was significantly enlarged in such cases.
• Tinnitus improvement
The assessed auditory and TMD indices for six patients are listed in Table 1.
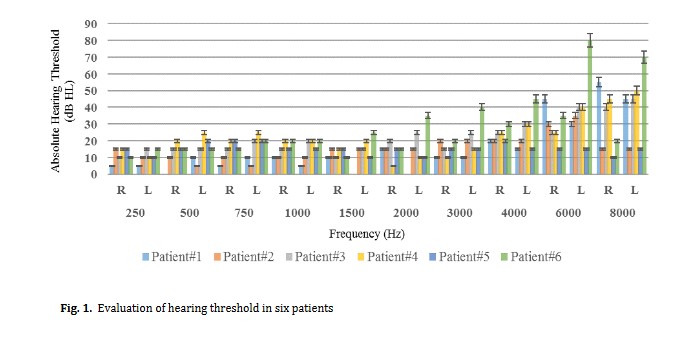
The predicted marginal pure-tone average (PTA) thresholds for both ears was recorded with 95% confidence interval (CI). Additionally, the mean values of audiometric thresholds at 250–8000 Hz octave frequencies were recorded in dBs of hearing level (dB HL) independently for the left and right ears of patients with tinnitus and TMD, with no significant differences between the groups (P>0.05) (Fig. 1).
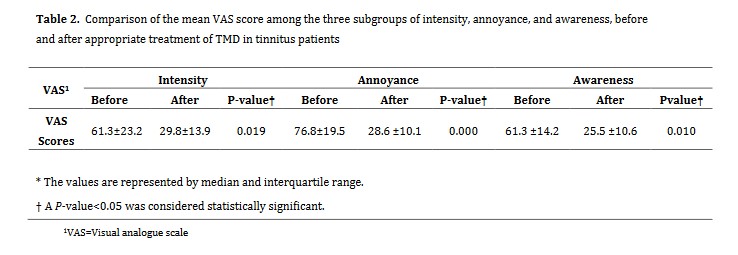
The change in VAS scores in the three subgroups of intensity, annoyance, and awareness, after TMD treatment compared with before in patients with tinnitus was significant for all parameters (P<0.05, Table 2).
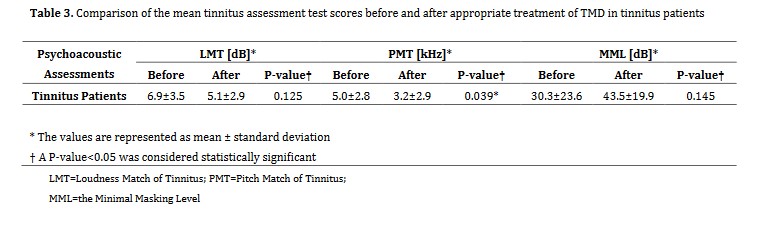
Comparing the mean tinnitus assessment test scores before and after TMD treatment in patients suffering from tinnitus revealed a significant change only in PMT (P=0.039, Table 3).
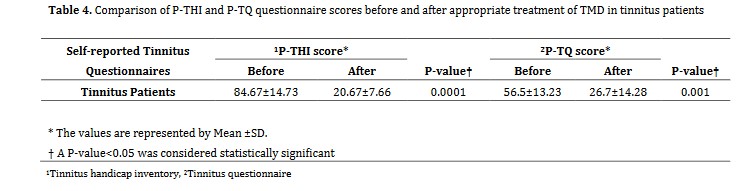
Comparing THI and TQ scores before and after TMD treatment in patients with tinnitus indicated that the differences were significant for both assessed scores (P<0.05, Table 4).
Fig. 1. Evaluation of hearing threshold in six patients
This study evaluated the efficacy of conservative TMD treatment for management of somatosensory tinnitus and TMJ-related parameters. Through an anatomical relationship, TMJ disease (e.g., disc displacement) or hypertonia of the masticatory muscles may affect middle ear muscular tension or ventilation (e.g., the tensor veli palatini, the Eustachian tube, or several ligaments). These factors would produce afferent signals that would affect the auditory circuits. Recent research has shown anatomical and functional links between the trigeminal and dorsal column systems of the somatosensory system and the cochlear nucleus of the auditory system in the medulla oblongata. The spinal trigeminal nucleus receives nociceptive and proprioceptive information from the head, face, oral structures, TMJ, and cervical spine (C1–C3). A proposed function of auditory-somatosensory interactions is the discrimination between external auditory signals and those produced by the body [24]. This functional link between the auditory and somatosensory systems in the brainstem may underlie the correlation between subjective tinnitus and TMD [24,25]. The present results demonstrated that the linked tinnitus and TMD indices and symptoms improved in six individuals after conservative TMD therapy. The strengths of the current study included a comprehensive evaluation of pertinent somatosensory tinnitus characteristics, as well as accurate case selection and treatment of TMD. In patients presenting with tinnitus and TMD or oral parafunctional habits, improvements in tinnitus may be accomplished by examining and treating TMJ-related symptoms [26]; nevertheless, case selection is essential for achieving optimal therapeutic effects. In addition, it is vital to develop proper TMJ treatment strategies for tinnitus problems to achieve maximum recovery. Several animal studies have provided physiological reasons for the frequent co-occurrence of tinnitus and TMD, revealing links between the somatosensory system of the cervical spine and the TMJ region and the cochlear nuclei.
Afferent fibers transmit somatosensory information from the cervical and temporomandibular regions to the brain through their cell bodies in the dorsal root ganglia or trigeminal ganglion. A number of these afferent fibers project to the central auditory system and, more specifically, to the dorsal cochlear nuclei [10], allowing the somatosensory system to influence the auditory system by modifying the spontaneous rates (i.e., not excited by auditory stimuli) or the synchronous firing of neurons in the central nucleus, inferior colliculus, or auditory cortex. Thus, the somatosensory system may affect the severity and features of tinnitus by forcibly contracting the neck or oral muscles or by increasing tension in the tensor tympani muscle [11]. At present, by recognizing the advantages of this treatment option, its comprehension and acceptance have been enhanced. This study was a preliminary effort to analyze and report beneficial changes in somatosensory tinnitus linked with TMD with regards to accurate case selection, which is crucial for success. Currently, the clinical assessment of somatosensory tinnitus is based on generally accepted anamnestic criteria [27,28]. According to these criteria, this type of tinnitus is suspected if it is associated with a history of head or neck trauma, premature tooth contacts, cervical spine, recurrent pains in the head, neck, or shoulder girdle, temporal coincidence of onset or increase in pain and tinnitus, and severe tinnitus. In addition, these criteria suggest a temporal and mechanical link between dysfunction of the TMJ or cervical spine and tinnitus-related symptoms.
Therefore, if one of the aforementioned criteria is present, somatosensory tinnitus is suspected, and more examinations are advised [29]. Other investigations [30-33] explored the alteration of tinnitus during intense contractions of the neck and oral muscles. However, similar tests evoked sound sensations in 65% of asymptomatic participants in a control group with no tinnitus complaints, reducing the diagnostic value of modulation testing for somatosensory tinnitus. To identify somatosensory tinnitus, this study included a combination of psychological, otorhinolaryngological, audiological, and temporomandibular examinations in addition to the diagnostic criteria indicated before. Since all of the primary etiological causes for tinnitus were removed, patients with severe subjective tinnitus and TMD symptoms were recruited in order to better understand the subjective tinnitus patients who potentially benefit from a therapeutic intervention.
Conclusion
TMD therapy might alleviate tinnitus in individuals with somatosensory tinnitus and simultaneous TMD signs and symptoms, according to the results of the present study. Consequently, a multidisciplinary approach may be useful in treatment of such patients.
Acknowledgment
This study was conducted with close cooperation of “Tehran Tinnitus Center”. The authors appreciate the technical and scientific supports provided by this center.
Introduction
Tinnitus is defined as perception of sound in absence of an external or environmental acoustic stimulus. It is often characterized as one sound or collection of noises [1] and might be experienced in one ear, both ears, or the patient's head [2]. The prevalence of tinnitus in adults varies from 10% to 15% [3], and it approaches 18% in those >60 years old [4].
According to a previous study, the prevalence of this ailment in the Iranian population is 4.6%, i.e., 6.4% and 14.6% among individuals in their sixth and seventh decades of life, and 16.8% among those >70 years old [5]. In addition to the impacts of the central auditory neurons, the majority of patients also suffer from subjective tinnitus alterations due to the somatosensory system. These individuals may alter volume and pitch by contraction of their neck, head, or oral muscles [6]. In addition to hearing loss or noise stress, somatic or somatosensory system abnormalities of the cervical spines or the temporomandibular joints (TMJ) may cause tinnitus [7, 8]. This may account for the common co-occurrence of tinnitus and temporomandibular joint disorder (TMD) syndrome reported in a number of studies [9-13]. Manfredini et al. [14] in their study on individuals with TMD, observed a prevalence rate of 30.4% for tinnitus. In addition, Lam et al. [10] found that 64% of individuals presenting with tinnitus had TMD. Buergers et al. [11] reported that people with this condition were eight times more likely to have tinnitus than those without it. The experience of tinnitus may change by firmly clenching the teeth [3]. Also, 36-43% of the population with subjective tinnitus have been reported to have somatic or somatosensory tinnitus. Evidence shows that effective treatment of TMD may alleviate the perception of tinnitus. Therefore, conservative therapy based on scientific data should target the multifaceted etiology of TMD. TMD should be treated with a multidisciplinary approach because numerous biological, psychological, and social factors are involved in its onset and progression [15]. In addition, patients must be educated about the potential causes of this disorder, and they must recognize their vital role in its management [16]. Each patient's therapy should be customized depending on the diagnosis and cause. Dentists and physical therapists may provide such patients with multimodal, customized, and conservative treatment [17]. Moreover, Sherman and Turk [18] observed that TMD therapy led to substantial improvements when paired with psychological therapies as opposed to traditional dental care alone, indicating that psychological components should be included in TMD treatments [18]. Similarly, Aggarwal et al. [19] observed that a complete treatment strategy integrating cognitive behavior therapy, postural control, and biofeedback might give participants with orofacial pain longer-lasting pain alleviation than standard care. Collectively, these data suggest that the diagnosis and treatment of TMD need a complex and interdisciplinary approach. Therefore, the purpose of the current study was to evaluate the effectiveness of conservative TMJ therapy in six patients with tinnitus by identifying their TMD signs and symptoms and documenting their improvements in the studied indices.
Materials and Methods
The patients in this case series had persistent subjective tinnitus and were selected among those referred to Tehran Tinnitus Center. Six male patients with chronic non-pulsatile tinnitus (duration > 6 months) and a mean age of 45.34 ±9.57 years were included in this study [20]. The patients had not received any treatment for their medical condition or therapeutic interventions on their brain or ears (e.g., acoustic, electrical, etc.) for 3 months prior to the onset of this study.
Patients who were evaluated in this study had no history of neurological conditions, head injuries, or brain tumor and had a definite diagnosis of chronic subjective idiopathic tinnitus (duration: > 6 months) confirmed by an audiologist and an otorhinolaryngologist. They also had normal external and middle ear function confirmed by otoscopy and tympanometry and the ability to read, speak, and write in Persian, and consented to participation in the study and completion of follow-ups. In addition, the participants had no history of chronic neurological or auditory diseases, had not taken neurological/psychiatric medications within the past three months, no pregnancy or nursing, no treatment for tinnitus within the past 3 months, no alcohol consumption or drug abuse, no head and neck diseases or space-occupying lesions, and their tinnitus was not secondary to a systemic medical condition. All patients were informed about the study and signed informed consent forms before the experiment.
Measurements and evaluations:
A complete medical history was taken from each patient and all patients underwent physical and psychological evaluations. All patients also underwent subjective and objective assessments for tinnitus prior to receiving TMD therapy. The magnetic resonance imaging gadolinium contrast medium indicated that there were no identifiable abnormalities in the temporal lobe or brain of the individuals. In situations of bilateral tinnitus, the dominant side with more severe symptoms was evaluated. In participants whose complaints were identical on both sides, measures from both ears were included in the study. All patients underwent audiological evaluations (i.e., pure tone audiometry and tympanometry) and tinnitus-related psychoacoustic measurements (i.e., pitch and loudness matching).
Tinnitus psychoacoustic assessments:
The diagnostic characteristics for tinnitus were examined using a clinical audiometer (Madsen®Astera2, Natus) with two channels for recreating the most bothersome tinnitus (MTT) at the same frequency and intensity. The pitch matching and loudness matching of tinnitus (PMT-LMT), minimum masking level (MML), and residual inhibition (RI) factors of tinnitus were evaluated. The precision of the equipment calibration met the American National Standard Specification for Audiometers tolerance requirements (Accuracy no.: #S3.6-200412). All participants' tinnitus parameters were assessed both before and after TMD treatment. For the PMT examination, a forced-choice format with two options was used. For this objective, multiple pairs of pitch sounds were created at 11 frequencies ranging from 125 Hz to 12 kHz. The pitch was then lowered or raised, and the participants were asked to identify which pitch best matched their tinnitus. Lastly, an octave confusion test was utilized to establish the frequency of tinnitus more precisely. Before presenting each pair, the loudness levels of tone pairs were modified to match those of the tinnitus. The LMT was also determined for each test tone in the PMT technique, after which the subject's auditory threshold at that particular frequency (A) was raised in 1-dB increments until they reported that the external tone was as loud as the tinnitus (B). Subsequently, the sound volume was adjusted in 1-dB increments to achieve a threshold somewhat higher than the tinnitus threshold (C). The mean level of loudness between (B) and (C) represented the volume of the tinnitus. This formula calculated the volume (expressed in decibels of the feeling level43):
Loudness of tinnitus=[(B+C)/2–A](dB SL) [20]
The MML was further assessed by the narrow-band noise in the afflicted ear until the tinnitus was completely masked. The RI was then measured using a narrow-band noise with an intensity of 10 dB greater than MML for 60 seconds. Importantly, tinnitus may be temporarily muted by an adequate masking stimulus, also known as RI. After the stimulus is deactivated, one of the following outcomes may occur: full RI (CRI), partial RI (PRI), non-residual inhibition (NRI), and lastly rebound effect (RF, or facilitated tinnitus), resulting in an increase in the loudness of tinnitus as experienced by the individuals. CRI is the condition in which tinnitus remains inaudible even after removing the masking stimuli. PRI also refers to a condition in which tinnitus is diminished but remains audible to the sufferer. When the tinnitus remains intact after the cessation of masking stimuli, this condition is known as NRI. In addition, the increase in the volume of tinnitus that occurs after turning off masking stimuli is known as the RF phenomenon [20].
Self-report tinnitus questionnaires:
The 52-item Tinnitus Questionnaire (TQ) [20-22], originally created by Hallam, was used in order to assess the behavioral side effects of tinnitus. The questionnaire has a Cronbach's alpha value of 0.95 and a test-retest reliability of 0.91 to 0.94 [15]. The subscales of the TQ comprised auditory-perceptual difficulties, intrusiveness, sleep issues, physical symptoms, and emotional and cognitive abnormalities. The Tinnitus Handicap Inventory (THI) [22,23], which was originally developed by Newman et al. [23] and consists of 25 questions, was then used to characterize the functional, emotional, and catastrophic implications of tinnitus on the patients' everyday life. This version was easy to administer and interpret as a very effective psychometric instrument. Currently, it is also used in other health/treatment facilities globally. The THI item analysis revealed that this self-report questionnaire has great internal consistency and sufficient convergent and construct validity. The THI scores were classified as 0–16 for mild, 18–36 for moderate, 38–56 for severe, 58–76 for severe, and 78–100 for suffering.
Visual analogue scale (VAS):
This questionnaire is a certified psychometric response scale which can be used to assess the effect of tinnitus on ordinary everyday living in terms of severity, irritation, and awareness. Responding to the VAS, respondents ranked the loudness, irritation, and disruption of tinnitus on a continuum from 0 to 10.
TMD evaluation:
The assessed patients completed the Steigerwald/Maher TMD Disability Index (SMTDI) [24]. Besides, VAS score for the existing tinnitus was recorded at baseline.
TMD was diagnosed based on symptom evaluation; the most often used diagnostic classification systems were the Research Diagnostic Criteria for TMD and the American Academy of Orofacial Pain classification [12]. The patients were evaluated by noting their TMD signs and symptoms, such as pain and TMJ sounds (i.e., clicking and crepitus), limitation and pain on mouth opening, any mandibular deviation during mouth opening, a history of bruxism and clenching, and measurements of central and lateral opening and evaluation of occlusion parameters, such as central and lateral occlusal contacts. Then, a treatment plan was designed based on the diagnostic data. All six patients were meticulously examined in accordance with the procedure, and their therapy regimens were established using the TMD method to account for the absence or weakness of other causative variables. Upon registration, the TMJ examination, the definitive diagnosis of TMD based on clinical assessment, and the associated subtype of TMD, including "capsulitis, deviation of disc form, anterior disc displacement, and subluxation with or without reduction" were also recorded. None of the subjects tested exhibited TMJ discomfort or tenderness. Two patients were also identified with subluxation with reduction, three patients with anterior disc displacement, and one patient with disc deviation. For each instance, the use of the bite guard (i.e., the flat occlusal splint) with regard to its occlusal adjustment, precise occlusal adjustment of teeth, and exclusive physical treatment, including therapeutic jaw exercise linked to either subtype of existing TMD were planned. Six patients were treated for an average of 8 months. The overview of the principal test and variance of measured parameters for each patient are provided in Table 1.
Results
• TMD Treatment
Two of the six patients evaluated were diagnosed with subluxation with reduction, three with anterior disc displacement, and one with disc deviation. After therapy, clicking and crepitus improved for 7.1 ±0.9 months. After therapy, three patients with a history of bruxism reported no parafunction. The mean SMTDI score decreased from 34.50 ±1.3 to 24.37 ±8.6, and this difference was significant according to paired-samples t-test (P=0.0001). The majority of patients did not have mouth opening limitation; therefore, appropriate room was either already available or was significantly enlarged in such cases.
• Tinnitus improvement
The assessed auditory and TMD indices for six patients are listed in Table 1.
The predicted marginal pure-tone average (PTA) thresholds for both ears was recorded with 95% confidence interval (CI). Additionally, the mean values of audiometric thresholds at 250–8000 Hz octave frequencies were recorded in dBs of hearing level (dB HL) independently for the left and right ears of patients with tinnitus and TMD, with no significant differences between the groups (P>0.05) (Fig. 1).
The change in VAS scores in the three subgroups of intensity, annoyance, and awareness, after TMD treatment compared with before in patients with tinnitus was significant for all parameters (P<0.05, Table 2).
Comparing the mean tinnitus assessment test scores before and after TMD treatment in patients suffering from tinnitus revealed a significant change only in PMT (P=0.039, Table 3).
Comparing THI and TQ scores before and after TMD treatment in patients with tinnitus indicated that the differences were significant for both assessed scores (P<0.05, Table 4).
Fig. 1. Evaluation of hearing threshold in six patients
{kind=link}
Table 1. Tinnitus and TMD indexes evaluated in six patients
Discussion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This study evaluated the efficacy of conservative TMD treatment for management of somatosensory tinnitus and TMJ-related parameters. Through an anatomical relationship, TMJ disease (e.g., disc displacement) or hypertonia of the masticatory muscles may affect middle ear muscular tension or ventilation (e.g., the tensor veli palatini, the Eustachian tube, or several ligaments). These factors would produce afferent signals that would affect the auditory circuits. Recent research has shown anatomical and functional links between the trigeminal and dorsal column systems of the somatosensory system and the cochlear nucleus of the auditory system in the medulla oblongata. The spinal trigeminal nucleus receives nociceptive and proprioceptive information from the head, face, oral structures, TMJ, and cervical spine (C1–C3). A proposed function of auditory-somatosensory interactions is the discrimination between external auditory signals and those produced by the body [24]. This functional link between the auditory and somatosensory systems in the brainstem may underlie the correlation between subjective tinnitus and TMD [24,25]. The present results demonstrated that the linked tinnitus and TMD indices and symptoms improved in six individuals after conservative TMD therapy. The strengths of the current study included a comprehensive evaluation of pertinent somatosensory tinnitus characteristics, as well as accurate case selection and treatment of TMD. In patients presenting with tinnitus and TMD or oral parafunctional habits, improvements in tinnitus may be accomplished by examining and treating TMJ-related symptoms [26]; nevertheless, case selection is essential for achieving optimal therapeutic effects. In addition, it is vital to develop proper TMJ treatment strategies for tinnitus problems to achieve maximum recovery. Several animal studies have provided physiological reasons for the frequent co-occurrence of tinnitus and TMD, revealing links between the somatosensory system of the cervical spine and the TMJ region and the cochlear nuclei.
Afferent fibers transmit somatosensory information from the cervical and temporomandibular regions to the brain through their cell bodies in the dorsal root ganglia or trigeminal ganglion. A number of these afferent fibers project to the central auditory system and, more specifically, to the dorsal cochlear nuclei [10], allowing the somatosensory system to influence the auditory system by modifying the spontaneous rates (i.e., not excited by auditory stimuli) or the synchronous firing of neurons in the central nucleus, inferior colliculus, or auditory cortex. Thus, the somatosensory system may affect the severity and features of tinnitus by forcibly contracting the neck or oral muscles or by increasing tension in the tensor tympani muscle [11]. At present, by recognizing the advantages of this treatment option, its comprehension and acceptance have been enhanced. This study was a preliminary effort to analyze and report beneficial changes in somatosensory tinnitus linked with TMD with regards to accurate case selection, which is crucial for success. Currently, the clinical assessment of somatosensory tinnitus is based on generally accepted anamnestic criteria [27,28]. According to these criteria, this type of tinnitus is suspected if it is associated with a history of head or neck trauma, premature tooth contacts, cervical spine, recurrent pains in the head, neck, or shoulder girdle, temporal coincidence of onset or increase in pain and tinnitus, and severe tinnitus. In addition, these criteria suggest a temporal and mechanical link between dysfunction of the TMJ or cervical spine and tinnitus-related symptoms.
Therefore, if one of the aforementioned criteria is present, somatosensory tinnitus is suspected, and more examinations are advised [29]. Other investigations [30-33] explored the alteration of tinnitus during intense contractions of the neck and oral muscles. However, similar tests evoked sound sensations in 65% of asymptomatic participants in a control group with no tinnitus complaints, reducing the diagnostic value of modulation testing for somatosensory tinnitus. To identify somatosensory tinnitus, this study included a combination of psychological, otorhinolaryngological, audiological, and temporomandibular examinations in addition to the diagnostic criteria indicated before. Since all of the primary etiological causes for tinnitus were removed, patients with severe subjective tinnitus and TMD symptoms were recruited in order to better understand the subjective tinnitus patients who potentially benefit from a therapeutic intervention.
Conclusion
TMD therapy might alleviate tinnitus in individuals with somatosensory tinnitus and simultaneous TMD signs and symptoms, according to the results of the present study. Consequently, a multidisciplinary approach may be useful in treatment of such patients.
Acknowledgment
This study was conducted with close cooperation of “Tehran Tinnitus Center”. The authors appreciate the technical and scientific supports provided by this center.
Type of Study: Original article |
Subject:
Prosthodontics
References
1. Han BI, Lee HW, Kim TY, Lim JS, Shin KS. Tinnitus: characteristics, causes, mechanisms, and treatments. J Clin Neu-rol. 2009 Mar;5(1):11-9. [DOI:10.3988/jcn.2009.5.1.11] [PMID] [PMCID]
2. Heller AJ. Classification and epidemiology of tinnitus. Otolaryngol Clin North Am. 2003 Apr;36(2):239-48. [DOI:10.1016/S0030-6665(02)00160-3] [PMID]
3. Baguley D, McFerran D, Hall D. Tinnitus. Lancet. 2013 Nov 9;382(9904):1600-7. [DOI:10.1016/S0140-6736(13)60142-7] [PMID]
4. Bhatt JM, Lin HW, Bhattacharyya N. Prevalence, Severity, Exposures, and Treatment Patterns of Tinnitus in the United States. JAMA Otolaryngol Head Neck Surg. 2016 Oct 1; 142 (10):959-65. [DOI:10.1001/jamaoto.2016.1700] [PMID] [PMCID]
5. Jalessi M, Farhadi M, Asghari A, Kamrava SK, Amintehran E, Ghalehbaghi S, Heshmatzadeh Behzadi A, Pousti SB. Tinnitus: an epidemiologic study in Iranian population. Acta Med Iran. 2013;51(12):886-91.
6. Björne A. Assessment of temporomandibular and cervical spine disorders in tinnitus patients. Prog Brain Res. 2007; 166:215-9. [DOI:10.1016/S0079-6123(07)66019-1] [PMID]
7. Teachey WS, Wijtmans EH, Cardarelli F, Levine RA. Tinnitus of myofascial origin. Int Tinnitus J. 2012;17(1):70-3.
8. Saldanha AD, Hilgenberg PB, Pinto LM, Conti PC. Are temporomandibular disorders and tinnitus associated? Cranio. 2012 Jul;30(3):166-71. [DOI:10.1179/crn.2012.026] [PMID]
9. Zhan X, Pongstaporn T, Ryugo DK. Projections of the second cervical dorsal root ganglion to the cochlear nucleus in rats. J Comp Neurol. 2006 May 20;496(3):335-48. [DOI:10.1002/cne.20917] [PMID] [PMCID]
10. Lam DK, Lawrence HP, Tenenbaum HC. Aural symptoms in temporomandibular disorder patients attending a craniofacial pain unit. J Orofac Pain. 2001 Spring;15(2):146-57.
11. Buergers R, Kleinjung T, Behr M, Vielsmeier V. Is there a link between tinnitus and temporomandibular disorders? J Prosthet Dent. 2014 Mar;111(3):222-7. [DOI:10.1016/j.prosdent.2013.10.001] [PMID]
12. Okeson JP. Orofacial pain: guidelines for assessment, diagno-sis, and management. Chicago: Quintessence Pub. Co.; 1996. 285 p.
13. Upton LG, Wijeyesakere SJ. The incidence of tinnitus in peo-ple with disorders of the temporomandibular joint. Int Tinnitus J. 2004;10(2):174-6.
14. Manfredini D, Olivo M, Ferronato G, Marchese R, Martini A, Guarda-Nardini L. Prevalence of tinnitus in patients with differ-ent temporomandibular disorders symptoms. Int Tinnitus J. 2015;19(2):47-51. [DOI:10.5935/0946-5448.20150008] [PMID]
15. Adler RH. Engel's biopsychosocial model is still relevant today. J Psychosom Res. 2009 Dec;67(6):607-11. [DOI:10.1016/j.jpsychores.2009.08.008] [PMID]
16. Durham J, Wassell RW. Recent Advancements in Temporo-mandibular Disorders (TMDs). Rev Pain. 2011 Mar;5 (1):18-25. [DOI:10.1177/204946371100500104] [PMID] [PMCID]
17. de Souza RF, Lovato da Silva CH, Nasser M, Fedorowicz Z, Al-Muharraqi MA. Interventions for the management of temporo-mandibular joint osteoarthritis. Cochrane Database Syst Rev. 2012 Apr 18;2012(4):CD007261. [DOI:10.1002/14651858.CD007261.pub2] [PMID] [PMCID]
18. Sherman JJ, Turk DC. Nonpharmacologic approaches to the management of myofascial temporomandibular disorders. Curr Pain Headache Rep. 2001 Oct;5(5):421-31. [DOI:10.1007/s11916-001-0053-7] [PMID]
19. Aggarwal VR, Lovell K, Peters S, Javidi H, Joughin A, Goldthorpe J. Psychosocial interventions for the management of chronic orofacial pain. Cochrane Database Syst Rev. 2011 Nov 9;(11):CD0084565. [DOI:10.1002/14651858.CD008456.pub2]
20. Daneshi A, Mahmoudian S, Farhadi M, Hasanzadeh S, Ghale-baghi B. Auditory electrical tinnitus suppression in patients with and without implants. Int Tinnitus J. 2005; 11 (1):85-91.
21. McKenna L, Handscomb L, Hoare DJ, Hall DA. A scientific cognitive-behavioral model of tinnitus: novel conceptualizations of tinnitus distress. Front Neurol. 2014 Oct 6;5:196. [DOI:10.3389/fneur.2014.00196] [PMID] [PMCID]
22. Mahmoudian S, Shahmiri E, Rouzbahani M, Jafari Z, Keyhani MR, Rahimi F, et al. Persian language version of the "Tinnitus Handicap Inventory": translation, standardization, validity and reliability. Int Tinnitus J. 2011;16(2):93-103.
23. Newman CW, Jacobson GP, Spitzer JB. Development of the Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1996 Feb;122(2):143-8. [DOI:10.1001/archotol.1996.01890140029007] [PMID]
24. Bousema EJ, Koops EA, van Dijk P, Dijkstra PU. Association Between Subjective Tinnitus and Cervical Spine or Temporomandibular Disorders: A Systematic Review. Trends Hear. 2018 Jan-Dec;22:2331216518800640. [DOI:10.1177/2331216518800640] [PMID] [PMCID]
25. Dehmel S, Cui YL, Shore SE. Cross-modal interactions of audi-tory and somatic inputs in the brainstem and midbrain and their imbalance in tinnitus and deafness. Am J Audiol. 2008 Dec;17(2):S193-209. [DOI:10.1044/1059-0889(2008/07-0045)] [PMID]
26. González-Iglesias J, Cleland JA, Neto F, Hall T, Fernández-de-las-Peñas C. Mobilization with movement, tho-racic spine manipulation, and dry needling for the management of temporomandibular disorder: a prospective case series. Physiother Theory Pract. 2013 Nov;29(8):586-95. [DOI:10.3109/09593985.2013.783895] [PMID]
27. Delgado De La Serna P, Plaza-Manzano G, Cleland J, Fernández-De-Las-Peñas C, Martín-Casas P, Díaz-Arribas MJ. Effects of Cervico-Mandibular Manual Therapy in Patients with Temporomandibular Pain Disorders and Associated Somatic Tinnitus: A Randomized Clinical Trial. Pain Medicine. 2020;21(3):613-24. [DOI:10.1093/pm/pnz278] [PMID]
28. Mahmoudian S, Lenarz M, Esser KH, Salamat B, Alaeddini F, Dengler R, Farhadi M, Lenarz T. Alterations in early auditory evoked potentials and brainstem transmission time associated with tinnitus residual inhibition induced by auditory electrical stimulation. Int Tinnitus J. 2013;18(1):63-74. [DOI:10.5935/0946-5448.20130009] [PMID]
29. Wright EF. Otologic symptom improvement through TMD therapy. Quintessence Int. 2007 Oct;38(9):e564-71.
30. Sanchez TG, Rocha CB. Diagnosis and management of soma-tosensory tinnitus: review article. Clinics (Sao Paulo). 2011;66(6):1089-94. [DOI:10.1590/S1807-59322011000600028] [PMID] [PMCID]
31. Won JY, Yoo S, Lee SK, Choi HK, Yakunina N, Le Q, Nam EC. Prevalence and factors associated with neck and jaw muscle modulation of tinnitus. Audiol Neurootol. 2013; 18 (4):261-73. [DOI:10.1159/000351685] [PMID]
32. Abel MD, Levine RA. Muscle contractions and auditory per-ception in tinnitus patients and nonclinical subjects. Cranio. 2004 Jul;22(3):181-91. [DOI:10.1179/crn.2004.024] [PMID]
33. Delgado de la Serna P, Plaza-Manzano G, Cleland J, Fernández-de-Las-Peñas C, Martín-Casas P, Díaz-Arribas MJ. Effects of Cervico-Mandibular Manual Therapy in Patients with Temporomandibular Pain Disorders and Associated Somat-ic Tinnitus: A Randomized Clinical Trial. Pain Med. 2020 Mar;21(3):613-624. [DOI:10.1093/pm/pnz278] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |