

Volume 7, Issue 4 (10-2022)
J Res Dent Maxillofac Sci 2022, 7(4): 202-209 |
Back to browse issues page


Ethics code: IR.MAZUMS.REC.1398.521
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Taghian M, Sadri L, Soleimani B, Moosazadeh M, Dehestani A, Tabarestani A. Oral Health-Related Quality of Life of 2 to 5-Year-Old Children in Iran. J Res Dent Maxillofac Sci 2022; 7 (4) :202-209
URL: http://jrdms.dentaliau.ac.ir/article-1-389-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-389-en.html



1- Department of Oral and maxillofacial surgery Dentistry, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran
2- Department of Pediatric Dentistry, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran , sadri.leyli@yahoo.com
3- Department of Pediatric Dentistry, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran
4- Faculty of Health, Health Sciences Research Center, Mazandaran University of Medical Sciences, Sari, Iran
5- Faculty of Dentistry, Mazandaran Uni-versity of Medical Sciences, Sari, Iran
6- Student research committee, Faculty of Dentistry, Mazandaran university of medical sciences, Sari, Iran
2- Department of Pediatric Dentistry, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran , sadri.leyli@yahoo.com
3- Department of Pediatric Dentistry, Dental Research Center, Faculty of Dentistry, Mazandaran University of Medical Sciences, Sari, Iran
4- Faculty of Health, Health Sciences Research Center, Mazandaran University of Medical Sciences, Sari, Iran
5- Faculty of Dentistry, Mazandaran Uni-versity of Medical Sciences, Sari, Iran
6- Student research committee, Faculty of Dentistry, Mazandaran university of medical sciences, Sari, Iran
Full-Text [PDF 726 kb]
(568 Downloads)
| Abstract (HTML) (885 Views)
Introduction
The present descriptive cross-sectional study was conducted on children between 2 to 5 years of age who were selected from kindergartens in Sari, Iran. A total of 1,750 children attended 69 kindergartens present in Sari city. A total of 1000 children were 4 to 5 years old, and 750 children were between 2 to 4 years of age.
The sample size was calculated according to a study by Gomes et al.[19] They reported the negative effect of oral health on children’s QoL to be 32.1%. Considering this value, the confidence interval of 95%, and accuracy of 0.04, the sample size was calculated to be 540 children using the sample size calculation formula. The children were selected after obtaining written permission from the Welfare Organization of Mazandaran Province (Ethics approval number: IR.MAZUMS.REC.1398.521).
Thirty kindergartens out of 69 were randomly selected. Then, census sampling was used for inclusion of children from the aforementioned 30 kindergartens. The sampling method was proportional to the sample size, and 310 children were selected from 4 to 5-year-old age group, and 230 children were selected from the 2 to 4-year-old age group.
The inclusion criteria consisted of children between 2 to 5 years of age with no systemic disease (based on reports of caregivers/ parents). The children with one or more erupted permanent teeth and incomplete questionnaires were excluded from the study. Written informed consent was obtained from all parents for enrollment of their children.
The ECOHIS was used for data collection. Jabarifar et al. confirmed the reliability and validity of this scale by a Cronbach's alpha coefficient of 0.93 [20]. It contains 13 questions and has two main parts: Family Impact Section (FIS) and Child Impact Section (CIS). The CIS section has 4 components of symptoms (1 item), child’s performance (4 items), mental health (2 items), and child’s social interactions and self-confidence (2 items). The FIS section includes areas of parents’ concern (2 items) and family performance (2 items).
According to the 5-point Likert scale, scoring was as follows: never: zero, very rarely: 1, only several times: 2, several times: 3, many times: 4, and I do not know: 5. In general, the total raw scores of this index can range from 0 to 52, which is from 0 to 36 in the CIS part and from 0 to 16 in the FIS part. The larger the final ECOHIS score, the greater the oral health issues and the lower the OHRQoL would be.
Incomplete questionnaires were those with one or more unanswered questions in the FIS part or two or more unanswered questions in the CIS part, and they were not included in the analysis. After receiving the questionnaires and obtaining informed consent, clinical examinations in kindergarten were performed by an examiner who had been previously calibrated under the supervision of an instructor. In case of dental trauma, a history was taken from the parents.
To evaluate the DMFT index, the tooth surfaces were cleaned with a sterile piece of gauze and carefully examined using a #20 explorer and a disposable mirror under natural light for caries or tooth-colored and non-tooth-colored restorations. The “M” stands for the number of missing teeth because of caries. A decayed tooth, i.e., “D” was considered in case of presence of caries in the fissures and pits or on smooth dental surfaces, undermined enamel or softening of the enamel and surrounding areas. Teeth with cavities restored with temporary filling materials and restored teeth with caries were considered as teeth with caries. Filled teeth were considered as restored teeth with normal function, size, and appearance “F”, which also included teeth with endodontic treatment and those restored with restorative materials or crowns. The mean of the scores was calculated as the DMFT score.
Data were analyzed with SPSS 16. Normal distribution of data was analyzed by the Shapiro-Wilk test. Data were described as percentage, mean, standard deviation, median, magnitude of change, and quartiles. Data were analyzed by independent t-test, ANOVA, and Chi-square test. The significance level was considered as P<0.05.
Results
Of 540 questionnaires administered, 25 were incomplete and were not included in the analysis because of having two or more unanswered questions in the CIS part (five items), one or more unanswered questions in the FIS part (eight items), or an incomplete questionnaire (12 items). The scores of “I do not know” answers were not included in the total score of each section.
Mothers completed 89.5% (n=461) of the questionnaires. The findings indicated that there was no significant difference between girls and boys in terms of age distribution (P=0.607).
Table 1 presents the mean scores for different parts of the ECOHIS. The total score range was 0-23 for the CIS section, and 0-12 for the FIS section. The total range of ECOHIS scores in this study was 0-35 with a mean and standard deviation of 4.3±6.5.
Table 1. Mean scores of different parts of the ECOHIS
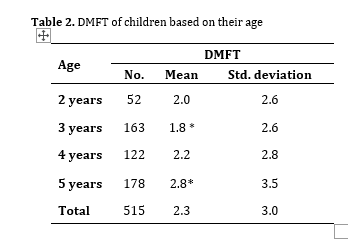
According to the results, the mean OHRQoL scores were not significantly different between girls and boys (P=0.672). The mean DMFT was 2.3±3.07. It should be noted that 46.9% of the children had DMFT=0. Table 2 shows the DMFT of children based on their age. ANOVA showed a statistically significant correlation between DMFT and age (P=0.014). According to the Tukey’s post-hoc test, the difference was only significant between the 3-year-old and 5-year-old groups, such that the latter group had a significantly higher DMFT (P=0.008).
Table 2. DMFT of children based on their age
Males and females did not show a significant difference in terms of the mean DMFT (P=0.067). According to the results, there was a positive correlation between DMFT and different sections of the OHRQoL (CIS: coefficient=0.479, P<0.001, FIS: coefficient=0.605, P<0.001, ECOHIS: coefficient=0.571, P<0.001). Based on the questionnaire, higher scores indicated poorer QoL. Therefore, higher DMFT values indicated poorer QoL.
Regarding the parents, out of 254 girl participants and 261 boy participants, 7.9% (20 cases) and 14.9% (39 cases) had a history of TDI, respectively. A comparison of the age groups with the Chi-square test showed that 2-year-olds had higher frequency of TDI compared with others (P=0.004). According to the Chi-square test, boys showed a higher frequency of TDI compared with girls (P=0.012). The relationship between the mean OHRQoL score and TDI based on independent t-test is shown in Table 3. According to the findings, there was a significant relationship between the positive responses regarding TDI and the mean FIS, CIS, and the total ECOHIS scores (P=0.001). It means a poorer QoL in those with a positive history of previous TDI.
Regarding the FIS, the FIS score and age did not have a significant relationship (P=0.090). It means that aging in children did not affect the parents’ QoL. Also, in the CIS section, a significant difference was found between the 3- and 5-year-old age groups (P=0.001) such that the 3-year-old age group had a significantly lower mean CIS score compared with 5-year-olds.
Table 3. Relationship of OHRQoL and TDI
Discussion
In recent years, the motivation for OHRQoL assessment has increased. This has been a significant development because a high number of children worldwide are affected by problems such as caries, TDI, and dental malformations [21, 22]. Poor oral health status can negatively affect the performance and well-being of young children and their families [22]. With assessment of oral health effects on QoL of children, the relationship of parents, patients, and dentists can be improved and a criterion can be presented for assessing the quality of treatment [21-24].
A crucial challenge in assessing the oral health issues of children is the unreliable responses and lack of knowledge. As a result, parents must participate in assessing the QoL of their children [25]. It should be noted that completing the ECOHIS entirely depends on the level of awareness and information of parents about diseases and oral health status of their children. A mother might behave differently towards her baby’s health compared with other parents and even the child himself. This causes social and individual differences and affects the accuracy of parents’ responses to questions [20].
In this study, the relationship of DMFT index and TDI with OHRQoL was investigated by using the Persian translation of ECOHIS, the reliability and validity of which, have been previously confirmed by Jabarifar et al. [20] As shown by the findings, higher mean DMFT and a positive history of TDI negatively impacted the QoL of young children and their parents.
The mean score of the CIS part of the ECOHIS in this study was 2.7±4.2. However, in a study by Scarpelli et al. [22] in Brazil, this score was 2.6±3.3. The mean FIS score in the present study was 1.8±3.0; this value was 1.4±2.2 in the study by Scarpelli et al. [22] In the present study, the oral health impact on the QoL was almost the same in both the family and child sections, and was even slightly higher than the results obtained in Brazil [22]. The mean total score of ECOHIS reported by Pani et al, in Saudi Arabia was 5.5±9.4, which was slightly higher than the score obtained in the present study [26].
In this study, the mean dmft was 2.3±3.7, and almost half of the children had dmft=0. However, the mentioned results are slightly in agreement with the results of Scarpelli et al. [22] In addition, the mean DMFT in the study in Saudi Arabia [26] was 2.7±4.0. The abovementioned results indicate that children’s oral health in the present study was consistent with the aforementioned studies.
As indicated by the present results, oral problems of children influence their own QoL more than their parents’ QoL. The mean score was 2.7±4.2 for children, and 1.8±3.0 for the parents. These findings are consistent with many studies [18, 22, 27]. It is possible to assess the effect of children’s oral health on their QoL by the observed impacts on their weight, social relationships, growth, self-confidence, and even their learning abilities [20, 28].
The correlation between OHRQoL scores and the DMFT index was positive in this study. This means that an increase in a child’s oral problems is directly correlated with a decrease in the QoL of both children and their parents. Interestingly, the correlation coefficient in the FIS section was higher than that in the CIS section. This might be because children’s oral problems can force parents to take leave from work or feel more financially burdened by dental care costs [19, 29, 30].
In the present study, according to parental responses, 11.5% of children had TDI. However, although the TDI prevalence was found to be low in this study, it had a significant adverse effect on children’s and parents’ QoL, consistent with many studies [19, 30]. Such oral problems can take a long time for parents for the urgent nature of the symptoms of pain and the possibility of functional constraints for the child [24, 31]. Although a strong association was found between the negative impact of TDI and QoL, some studies did not find such a correlation [22, 32]. This might be because of differences in the type of TDI examined in such studies because the adverse effect of TDI is more noticeable in severe cases [22, 30].
In this study, the difference in the OHRQoL of children was significant between the 3- and 5-year-old age groups. It means that 5-year-olds had a lower QoL compared with 3-year-olds. Li et al. reported a strong association between age and QoL. Another study showed that the oral health impact on QoL increased with age [27]. It can be because of the children’s incapability in reporting discomfort and pain during food intake. The low social development and cognition of young children make them less sensitive to the impact of social factors such as not talking and not laughing [18].
The mean scores of OHRQoL in males and females were the same in this study, consistent with many studies [18, 33]. Preschoolers are usually not different in diet, oral hygiene, parental care, and hormonal changes. Nevertheless, with aging over time, these differences between the sexes might increase [18].
The present findings indicated the necessity of developing oral health promotion courses for supporting caregivers and parents of children to enhance their oral health knowledge. Behavior changes to improve the OHRQoL require practical and motivational tools and training of parents to overcome the problems in this area. Also, they should be motivated towards preventive dental care. Patient-focused counseling methods and concise and useful methods like motivational interviews have proven to be effective in enhancing young children’s oral health in developed and some developing countries [34, 35].
Limitations
This study had the limitations of cross-sectional studies, including the possibility of fading effect bias when completing the questionnaire. However, an attempt was made to reduce such errors by using a scale with a confirmed reliability and validity.
Conclusion
The present study confirmed the inverse correlation of the mean DMFT in children and their QoL and that of their parents. Besides, the findings indicated the greater effect of oral health status on children’s QoL compared with their parents’ QoL. TDI had an inverse correlation with children’s QoL.
Full-Text: (331 Views)
|
Abstract
Background and Aim: Traumatic dental injuries (TDI) and dental caries are among the prevalent oral health issues in preschool children that can lead to psychosocial and physical complications. Therefore, it is crucial to assess their effects on children’s oral health-related quality of life (OHRQoL). This study aimed to assess the effect of oral health status on OHRQoL of 2- to 5-year-old children in Sari, Iran. Materials and Methods: This cross-sectional study was conducted on 540 randomly selected children between 2 to 5 years. Their decayed, missing, and filled teeth (DMFT) indices was determined by oral clinical examination. The Early Childhood Oral Health Impact Scale (ECOHIS) was completed by the parents. SPSS 16 was used for statistical analysis by the Chi-square test, independent t-test, and ANOVA. Results: The ECOHIS mean scores in the Family Impact Section (FIS) and Child Impact Section (CIS) were 1.8±3.0 and 2.7±4.2, respectively. The mean DMFT score of children was 3.2±3.07, with 47% having a DMFT of 0. The frequency of TDI was 11.5%. The DMFT index and ECOHIS were significantly correlated (r=0.571, P<0.001). A statistically significant correlation was found between ECOHIS and TDI, indicating lower quality of life (QoL) in patients with a history of TDI (P<0.001). Conclusion: Children’s oral health considerably affects their own and their parents’ QoL. Its effect on children’s QoL is greater than its impact on the QoL of the parents. Key Words: DMFT Index; Child, Preschool; Oral Health; Quality of Life |
Introduction
Oral health affects the oral cavity and the children’s mental and physical status and appearance; it also affects their growth and development, speech, sense of taste, mastication, social relations, and establishing a sense of social satisfaction [1]. Oral health can be compromised by various factors, including traumatic dental injuries (TDI) and dental caries [2]. Severe caries causes a reduction in children’s quality of life (QoL) since such children experience discomfort, pain, chronic and acute infections, poor appearance, and absenteeism. It also increases the need for hospitalization, imposes high treatment costs, and results in lower learning ability [3]. Dental caries also adversely affects nutrition and growth status [4].
Dental pain and infection affect nutrition and sleep patterns [5]. Disturbed sleep alters the children’s QoL in various ways, as it affects glucocorticoid production and decreases red blood cell and hemoglobin production [6].
TDI are defined as traumas applied to the teeth and their supporting structures, leading to tooth fracture, luxation or avulsion, and destruction of supporting structures such as the gingiva and bone.[7, 8] Also, TDI can lead to functional, esthetic, psychological, and social problems, and significantly affect the QoL [9-11].
Various studies have identified different factors that influence the oral health-related quality of life (OHRQoL) of children, such as the family’s socioeconomic status, parents’ educational level, and parents’ oral health status and awareness about the oral health of their children [12-15]. Oral health has a significant correlation with these factors. Also, oral health of children can affect the family’s QoL. On the other hand, factors such as parents’ socioeconomic status can affect their understanding of the importance of caring for their children’s oral health [16].
There are a few scales for measurement of OHRQoL of preschool children, one of which is the Early Childhood Oral Health Impact Scale (ECOHIS). This scale is one of the tools with a good level of sensitivity and response as reported in previous studies [17,18].
Therefore, considering the importance of oral health, this study investigated the relationship of OHRQoL and oral health status in 2 to 5-year-old children in Sari, Iran, in 2019.
Materials and Methods
Dental pain and infection affect nutrition and sleep patterns [5]. Disturbed sleep alters the children’s QoL in various ways, as it affects glucocorticoid production and decreases red blood cell and hemoglobin production [6].
TDI are defined as traumas applied to the teeth and their supporting structures, leading to tooth fracture, luxation or avulsion, and destruction of supporting structures such as the gingiva and bone.[7, 8] Also, TDI can lead to functional, esthetic, psychological, and social problems, and significantly affect the QoL [9-11].
Various studies have identified different factors that influence the oral health-related quality of life (OHRQoL) of children, such as the family’s socioeconomic status, parents’ educational level, and parents’ oral health status and awareness about the oral health of their children [12-15]. Oral health has a significant correlation with these factors. Also, oral health of children can affect the family’s QoL. On the other hand, factors such as parents’ socioeconomic status can affect their understanding of the importance of caring for their children’s oral health [16].
There are a few scales for measurement of OHRQoL of preschool children, one of which is the Early Childhood Oral Health Impact Scale (ECOHIS). This scale is one of the tools with a good level of sensitivity and response as reported in previous studies [17,18].
Therefore, considering the importance of oral health, this study investigated the relationship of OHRQoL and oral health status in 2 to 5-year-old children in Sari, Iran, in 2019.
Materials and Methods
The present descriptive cross-sectional study was conducted on children between 2 to 5 years of age who were selected from kindergartens in Sari, Iran. A total of 1,750 children attended 69 kindergartens present in Sari city. A total of 1000 children were 4 to 5 years old, and 750 children were between 2 to 4 years of age.
The sample size was calculated according to a study by Gomes et al.[19] They reported the negative effect of oral health on children’s QoL to be 32.1%. Considering this value, the confidence interval of 95%, and accuracy of 0.04, the sample size was calculated to be 540 children using the sample size calculation formula. The children were selected after obtaining written permission from the Welfare Organization of Mazandaran Province (Ethics approval number: IR.MAZUMS.REC.1398.521).
Thirty kindergartens out of 69 were randomly selected. Then, census sampling was used for inclusion of children from the aforementioned 30 kindergartens. The sampling method was proportional to the sample size, and 310 children were selected from 4 to 5-year-old age group, and 230 children were selected from the 2 to 4-year-old age group.
The inclusion criteria consisted of children between 2 to 5 years of age with no systemic disease (based on reports of caregivers/ parents). The children with one or more erupted permanent teeth and incomplete questionnaires were excluded from the study. Written informed consent was obtained from all parents for enrollment of their children.
The ECOHIS was used for data collection. Jabarifar et al. confirmed the reliability and validity of this scale by a Cronbach's alpha coefficient of 0.93 [20]. It contains 13 questions and has two main parts: Family Impact Section (FIS) and Child Impact Section (CIS). The CIS section has 4 components of symptoms (1 item), child’s performance (4 items), mental health (2 items), and child’s social interactions and self-confidence (2 items). The FIS section includes areas of parents’ concern (2 items) and family performance (2 items).
According to the 5-point Likert scale, scoring was as follows: never: zero, very rarely: 1, only several times: 2, several times: 3, many times: 4, and I do not know: 5. In general, the total raw scores of this index can range from 0 to 52, which is from 0 to 36 in the CIS part and from 0 to 16 in the FIS part. The larger the final ECOHIS score, the greater the oral health issues and the lower the OHRQoL would be.
Incomplete questionnaires were those with one or more unanswered questions in the FIS part or two or more unanswered questions in the CIS part, and they were not included in the analysis. After receiving the questionnaires and obtaining informed consent, clinical examinations in kindergarten were performed by an examiner who had been previously calibrated under the supervision of an instructor. In case of dental trauma, a history was taken from the parents.
To evaluate the DMFT index, the tooth surfaces were cleaned with a sterile piece of gauze and carefully examined using a #20 explorer and a disposable mirror under natural light for caries or tooth-colored and non-tooth-colored restorations. The “M” stands for the number of missing teeth because of caries. A decayed tooth, i.e., “D” was considered in case of presence of caries in the fissures and pits or on smooth dental surfaces, undermined enamel or softening of the enamel and surrounding areas. Teeth with cavities restored with temporary filling materials and restored teeth with caries were considered as teeth with caries. Filled teeth were considered as restored teeth with normal function, size, and appearance “F”, which also included teeth with endodontic treatment and those restored with restorative materials or crowns. The mean of the scores was calculated as the DMFT score.
Data were analyzed with SPSS 16. Normal distribution of data was analyzed by the Shapiro-Wilk test. Data were described as percentage, mean, standard deviation, median, magnitude of change, and quartiles. Data were analyzed by independent t-test, ANOVA, and Chi-square test. The significance level was considered as P<0.05.
Results
Of 540 questionnaires administered, 25 were incomplete and were not included in the analysis because of having two or more unanswered questions in the CIS part (five items), one or more unanswered questions in the FIS part (eight items), or an incomplete questionnaire (12 items). The scores of “I do not know” answers were not included in the total score of each section.
Mothers completed 89.5% (n=461) of the questionnaires. The findings indicated that there was no significant difference between girls and boys in terms of age distribution (P=0.607).
Table 1 presents the mean scores for different parts of the ECOHIS. The total score range was 0-23 for the CIS section, and 0-12 for the FIS section. The total range of ECOHIS scores in this study was 0-35 with a mean and standard deviation of 4.3±6.5.
Table 1. Mean scores of different parts of the ECOHIS
{kind=link}
According to the results, the mean OHRQoL scores were not significantly different between girls and boys (P=0.672). The mean DMFT was 2.3±3.07. It should be noted that 46.9% of the children had DMFT=0. Table 2 shows the DMFT of children based on their age. ANOVA showed a statistically significant correlation between DMFT and age (P=0.014). According to the Tukey’s post-hoc test, the difference was only significant between the 3-year-old and 5-year-old groups, such that the latter group had a significantly higher DMFT (P=0.008).
Table 2. DMFT of children based on their age
{kind=link}
Males and females did not show a significant difference in terms of the mean DMFT (P=0.067). According to the results, there was a positive correlation between DMFT and different sections of the OHRQoL (CIS: coefficient=0.479, P<0.001, FIS: coefficient=0.605, P<0.001, ECOHIS: coefficient=0.571, P<0.001). Based on the questionnaire, higher scores indicated poorer QoL. Therefore, higher DMFT values indicated poorer QoL.
Regarding the parents, out of 254 girl participants and 261 boy participants, 7.9% (20 cases) and 14.9% (39 cases) had a history of TDI, respectively. A comparison of the age groups with the Chi-square test showed that 2-year-olds had higher frequency of TDI compared with others (P=0.004). According to the Chi-square test, boys showed a higher frequency of TDI compared with girls (P=0.012). The relationship between the mean OHRQoL score and TDI based on independent t-test is shown in Table 3. According to the findings, there was a significant relationship between the positive responses regarding TDI and the mean FIS, CIS, and the total ECOHIS scores (P=0.001). It means a poorer QoL in those with a positive history of previous TDI.
Regarding the FIS, the FIS score and age did not have a significant relationship (P=0.090). It means that aging in children did not affect the parents’ QoL. Also, in the CIS section, a significant difference was found between the 3- and 5-year-old age groups (P=0.001) such that the 3-year-old age group had a significantly lower mean CIS score compared with 5-year-olds.
Table 3. Relationship of OHRQoL and TDI
{kind=link}
Discussion
In recent years, the motivation for OHRQoL assessment has increased. This has been a significant development because a high number of children worldwide are affected by problems such as caries, TDI, and dental malformations [21, 22]. Poor oral health status can negatively affect the performance and well-being of young children and their families [22]. With assessment of oral health effects on QoL of children, the relationship of parents, patients, and dentists can be improved and a criterion can be presented for assessing the quality of treatment [21-24].
A crucial challenge in assessing the oral health issues of children is the unreliable responses and lack of knowledge. As a result, parents must participate in assessing the QoL of their children [25]. It should be noted that completing the ECOHIS entirely depends on the level of awareness and information of parents about diseases and oral health status of their children. A mother might behave differently towards her baby’s health compared with other parents and even the child himself. This causes social and individual differences and affects the accuracy of parents’ responses to questions [20].
In this study, the relationship of DMFT index and TDI with OHRQoL was investigated by using the Persian translation of ECOHIS, the reliability and validity of which, have been previously confirmed by Jabarifar et al. [20] As shown by the findings, higher mean DMFT and a positive history of TDI negatively impacted the QoL of young children and their parents.
The mean score of the CIS part of the ECOHIS in this study was 2.7±4.2. However, in a study by Scarpelli et al. [22] in Brazil, this score was 2.6±3.3. The mean FIS score in the present study was 1.8±3.0; this value was 1.4±2.2 in the study by Scarpelli et al. [22] In the present study, the oral health impact on the QoL was almost the same in both the family and child sections, and was even slightly higher than the results obtained in Brazil [22]. The mean total score of ECOHIS reported by Pani et al, in Saudi Arabia was 5.5±9.4, which was slightly higher than the score obtained in the present study [26].
In this study, the mean dmft was 2.3±3.7, and almost half of the children had dmft=0. However, the mentioned results are slightly in agreement with the results of Scarpelli et al. [22] In addition, the mean DMFT in the study in Saudi Arabia [26] was 2.7±4.0. The abovementioned results indicate that children’s oral health in the present study was consistent with the aforementioned studies.
As indicated by the present results, oral problems of children influence their own QoL more than their parents’ QoL. The mean score was 2.7±4.2 for children, and 1.8±3.0 for the parents. These findings are consistent with many studies [18, 22, 27]. It is possible to assess the effect of children’s oral health on their QoL by the observed impacts on their weight, social relationships, growth, self-confidence, and even their learning abilities [20, 28].
The correlation between OHRQoL scores and the DMFT index was positive in this study. This means that an increase in a child’s oral problems is directly correlated with a decrease in the QoL of both children and their parents. Interestingly, the correlation coefficient in the FIS section was higher than that in the CIS section. This might be because children’s oral problems can force parents to take leave from work or feel more financially burdened by dental care costs [19, 29, 30].
In the present study, according to parental responses, 11.5% of children had TDI. However, although the TDI prevalence was found to be low in this study, it had a significant adverse effect on children’s and parents’ QoL, consistent with many studies [19, 30]. Such oral problems can take a long time for parents for the urgent nature of the symptoms of pain and the possibility of functional constraints for the child [24, 31]. Although a strong association was found between the negative impact of TDI and QoL, some studies did not find such a correlation [22, 32]. This might be because of differences in the type of TDI examined in such studies because the adverse effect of TDI is more noticeable in severe cases [22, 30].
In this study, the difference in the OHRQoL of children was significant between the 3- and 5-year-old age groups. It means that 5-year-olds had a lower QoL compared with 3-year-olds. Li et al. reported a strong association between age and QoL. Another study showed that the oral health impact on QoL increased with age [27]. It can be because of the children’s incapability in reporting discomfort and pain during food intake. The low social development and cognition of young children make them less sensitive to the impact of social factors such as not talking and not laughing [18].
The mean scores of OHRQoL in males and females were the same in this study, consistent with many studies [18, 33]. Preschoolers are usually not different in diet, oral hygiene, parental care, and hormonal changes. Nevertheless, with aging over time, these differences between the sexes might increase [18].
The present findings indicated the necessity of developing oral health promotion courses for supporting caregivers and parents of children to enhance their oral health knowledge. Behavior changes to improve the OHRQoL require practical and motivational tools and training of parents to overcome the problems in this area. Also, they should be motivated towards preventive dental care. Patient-focused counseling methods and concise and useful methods like motivational interviews have proven to be effective in enhancing young children’s oral health in developed and some developing countries [34, 35].
Limitations
This study had the limitations of cross-sectional studies, including the possibility of fading effect bias when completing the questionnaire. However, an attempt was made to reduce such errors by using a scale with a confirmed reliability and validity.
Conclusion
The present study confirmed the inverse correlation of the mean DMFT in children and their QoL and that of their parents. Besides, the findings indicated the greater effect of oral health status on children’s QoL compared with their parents’ QoL. TDI had an inverse correlation with children’s QoL.
Type of Study: Original article |
Subject:
pediatric
References
1. Matichescu A, Matichescu ML, Ogodescu AS, Luca MM, Rosu S. Oral hygiene behaviour. Case study of primary school children from Timis county. Revista de Cercetare si Interventie Sociala. 2016;54:142-55.
2. Pakkhesal M, Riyahi E, Naghavi Alhosseini A, Amdjadi P, Behnampour N. Impact of dental caries on oral health related quality of life among preschool children: perceptions of parents. BMC Oral Health. 2021 Feb 15;21(1):68. [DOI:10.1186/s12903-021-01396-4] [PMID] [PMCID]
3. Gerritsen AE, Allen PF, Witter DJ, Bronkhorst EM, Creugers NH. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Out-comes. 2010 Nov 5;8:126. [DOI:10.1186/1477-7525-8-126] [PMID] [PMCID]
4. Karki S, Päkkilä J, Laitala ML, Humagain M, Anttonen V. Influ-ence of dental caries on oral health‐related quality of life, school absenteeism and school performance among Nepalese school-children. Community Dent Oral Epidemiol. 2019 Jul;47(6):461-9. [DOI:10.1111/cdoe.12485] [PMID]
5. Tsakos G, Steele JG, Marcenes W, Walls AW, Sheiham A. Clinical correlates of oral health-related quality of life: evidence from a national sample of British older people. Eur J Oral Sci. 2006 Oct;114(5):391-5. [DOI:10.1111/j.1600-0722.2006.00398.x] [PMID]
6. Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. 2011 Nov;90(11):1264-70. [DOI:10.1177/0022034511399918] [PMID] [PMCID]
7. Gupta M, Kumar S, Kaur J, Gupta S, Bansal V, Dwiedi A. Preva-lence, risk factors, and treatment needs of traumatic dental inju-ries of anterior teeth among 11-15 year old children attending government and private schools of Bhopal City, India. India. J Adv Oral Res 2016;7(2):32-9. [DOI:10.1177/2229411220160206]
8. Andreasen JA, Andersson L. Textbook and Color Atlas of Traumatic Injuries to the Teeth, 4th Edition.Oxford: Wiley-Blackwell; 2013.912p.
9. Kargul B, Cağlar E, Tanboga I. Dental trauma in Turkish chil-dren, Istanbul. Dent Traumatol. 2003 Apr;19(2):72-5. [DOI:10.1034/j.1600-9657.2003.00091.x] [PMID]
10. Ramos-Jorge ML, Bosco VL, Peres MA, Nunes AC. The impact of treatment of dental trauma on the quality of life of adolescents - a case-control study in southern Brazil. Dent Traumatol. 2007 Apr;23(2):114-9. [DOI:10.1111/j.1600-9657.2005.00409.x] [PMID]
11. Jokovic A, Locker D, Stephens M, Kenny D, Tompson B, Guyatt G. Measuring parental perceptions of child oral health-related quality of life. J Public Health Dent. 2003 Spring;63(2):67-72. [DOI:10.1111/j.1752-7325.2003.tb03477.x] [PMID]
12. Sanders AE, Spencer AJ. Childhood circumstances, psychosocial factors and the social impact of adult oral health. Community Dent Oral Epidemiol. 2005 Oct;33(5): 370-7. [DOI:10.1111/j.1600-0528.2005.00237.x] [PMID]
13. Goursand D, Paiva SM, Zarzar PM, Ramos-Jorge ML, Cornacchia GM, Pordeus IA, Allison PJ. Cross-cultural adaptation of the Child Perceptions Questionnaire 11-14 (CPQ11-14) for the Brazilian Portuguese language. Health Qual Life Outcomes. 2008 Jan 14;6:2. [DOI:10.1186/1477-7525-6-2] [PMID] [PMCID]
14. Locker D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent Oral Epi-demiol. 2007 Oct;35(5):348-56. [DOI:10.1111/j.1600-0528.2006.00323.x] [PMID]
15. Paula JS, Leite IC, Almeida AB, Ambrosano GM, Perei-ra AC, Mialhe FL. The influence of oral health conditions, socioeconomic status and home environment factors on schoolchildren's self-perception of quality of life. Health Qual Life Out-comes. 2012 Jan 13;10:6. [DOI:10.1186/1477-7525-10-6] [PMID] [PMCID]
16. Nilchian F, Jabbarifar SE, Larijani M, Navaei H. Evaluation of the impact of children's oral health on their family quality of life in Amol, Iran. J Isfahan Dent Sch. 2013;8(7):662-8.
17. Saleki M, Jabbarifar SE, Soheilipour S, Hajjizadeh F. Assessing the sensitivity and responsiveness of Early Childhood Oral Health Impact Scale to routine dental treatments on life quality of preschool children in Isfahan in 2011. J Isfahan Dent Sch. 2012;7(5):688-97.
18. Sajadi FS, Pishbin L, Azhari SH, Moosazadeh M. Impact of oral and dental health on children's and parents' quality of life based on Early Childhood Oral Health Impact Scale (ECOHIS) Index. Int J Dent Sci Res. 2015;3(2):28-31. [DOI:10.12691/ijdsr-3-2-2]
19. Gomes MC, Pinto-Sarmento TC, Costa EM, Martins CC, Gran-ville-Garcia AF, Paiva SM. Impact of oral health conditions on the quality of life of preschool children and their families: a cross-sectional study. Health Qual Life Outcomes. 2014 Apr 18;12:55. [DOI:10.1186/1477-7525-12-55] [PMID] [PMCID]
20. Jabarifar SE, Golkari A, Ijadi MH, Jafarzadeh M, Khadem P. Validation of a Farsi version of the early childhood oral health impact scale (F-ECOHIS). BMC Oral Health. 2010 Apr 6;10:4. [DOI:10.1186/1472-6831-10-4] [PMID] [PMCID]
21. McGrath C, Broder H, Wilson-Genderson M. Assessing the impact of oral health on the life quality of children: implications for research and practice. Community Dent Oral Epidemiol. 2004 Apr;32(2):81-5. [DOI:10.1111/j.1600-0528.2004.00149.x] [PMID]
22. Scarpelli AC, Oliveira BH, Tesch FC, Leão AT, Pordeus IA, Paiva SM. Psychometric properties of the Brazilian version of the Early Childhood Oral Health Impact Scale (B-ECOHIS). BMC Oral Health. 2011 Jun 13;11:19. [DOI:10.1186/1472-6831-11-19] [PMID] [PMCID]
23. Sheiham A, Maizels JE, Cushing AM. The concept of need in dental care. Int Dent J. 1982 Sep;32(3):265-70.
24. Kramer PF, Feldens CA, Ferreira SH, Bervian J, Rodrigues PH, Peres MA. Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dent Oral Epidemiol. 2013 Aug;41(4):327-35. [DOI:10.1111/cdoe.12035] [PMID]
25. Eiser C, Morse R. Can parents rate their child's health-related quality of life? Results of a systematic review. Qual Life Res. 2001;10(4):347-57. [DOI:10.1023/A:1012253723272] [PMID]
26. Pani SC, Badea L, Mirza S, Elbaage N. Differences in perceptions of early childhood oral health-related quality of life between fathers and mothers in Saudi Arabia. Int J Paediatr Dent. 2012 Jul;22(4):244-9. [DOI:10.1111/j.1365-263X.2011.01185.x] [PMID]
27. Li S, Veronneau J, Allison PJ. Validation of a French language version of the Early Childhood Oral Health Impact Scale (ECOHIS). Health Qual Life Outcomes. 2008 Jan 22;6:9. [DOI:10.1186/1477-7525-6-9] [PMID] [PMCID]
28. Martins-Júnior PA, Ramos-Jorge J, Paiva SM, Marques LS, Ramos-Jorge ML. Validations of the Brazilian version of the Early Childhood Oral Health Impact Scale (ECOHIS). Cad Saude Publica. 2012 Feb;28(2):367-74. [DOI:10.1590/S0102-311X2012000200015] [PMID]
29. Abanto J, Tello G, Bonini GC, Oliveira LB, Murakami C, Bönecker M. Impact of traumatic dental injuries and malocclusions on quality of life of preschool children: a population-based study. Int J Paediatr Dent. 2015 Jan;25(1): 18-28. [DOI:10.1111/ipd.12092] [PMID]
30. Abanto J, Tsakos G, Ardenghi TM, Paiva SM, Raggio DP, Shei-ham A, Bönecker M. Responsiveness to change for the Brazilian Scale of Oral Health Outcomes for 5-year-old children (SOHO-5). Health Qual Life Outcomes. 2013 Aug 9; 11:137. [DOI:10.1186/1477-7525-11-137] [PMID] [PMCID]
31. Aldrigui JM, Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bönecker M, Raggio DP. Impact of traumatic dental injuries and malocclusions on quality of life of young children. Health Qual Life Outcomes. 2011 Sep 24;9:78. [DOI:10.1186/1477-7525-9-78] [PMID] [PMCID]
32. Viegas CM, Scarpelli AC, Carvalho AC, Ferreira Fde M, Porde-us IA, Paiva SM. Impact of traumatic dental injury on quality of life among Brazilian preschool children and their families. Pedi-atr Dent. 2012 Jul-Aug;34(4):300-6.
33. Kavand G, Younesian F, Safar Shahroudi A, Dori M,Akbarzadeh Baghban AR, Khoushnevisan MH. Oral Health Relat-ed Quality Of Life Among Iranian Children: Part I - Validity, Reli-ability, Prevalence And Severity Assessment Of Daily Impact Factors. J Dent Sch. 2010;27(4):187-96.
34. Yevlahova D, Satur J. Models for individual oral health pro-motion and their effectiveness: a systematic review. Aust Dent J. 2009 Sep;54(3):190-7. [DOI:10.1111/j.1834-7819.2009.01118.x] [PMID]
35. Naidu R, Nunn J, Irwin JD. The effect of motivational interviewing on oral healthcare knowledge, attitudes and be-haviour of parents and caregivers of preschool children: an exploratory cluster randomised controlled study. BMC Oral Health. 2015 Sep 2;15:101. [DOI:10.1186/s12903-015-0068-9] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
