Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 3 (8-2023)
J Res Dent Maxillofac Sci 2023, 8(3): 217-220 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yadegari Naini A, Kobravi S, Jafari A. Intraoral Management of a Root Displaced into the Submandibular Space: A Case Report. J Res Dent Maxillofac Sci 2023; 8 (3) :217-220
URL: http://jrdms.dentaliau.ac.ir/article-1-385-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-385-en.html



1- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry (Khorasgan), Isfahan Azad University, Isfahan, Iran
2- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Tehran Azad University, Tehran, Iran ,sepehr.kobravi@gmail.com
3- Faculty of Dentistry (Khorasgan), Isfahan Azad University, Isfahan, Iran
2- Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Tehran Azad University, Tehran, Iran ,
3- Faculty of Dentistry (Khorasgan), Isfahan Azad University, Isfahan, Iran
Full-Text [PDF 781 kb]
(881 Downloads)
| Abstract (HTML) (2136 Views)
Introduction
Full-Text: (2696 Views)
|
Abstract
Background and Aim: Displacement of a tooth or part of it into the adjacent anatomical structures is a serious complication of oral surgical procedures. Herein, we report intraoral management of a root displaced into the submandibular space.
Case Presentation: A 46-year-old female was referred by a dentist to the department of oral and maxillofacial surgery for management of a displaced right mandibular third molar root into the submandibular space. The patient had undergone unsuccessful extraction of the tooth under local anesthesia 2 weeks earlier. On clinical examination, the floor of the mouth was tender on palpation, and slight edema was noted extra-orally at the right mandibular angle. Panoramic radiography and cone beam computed tomography (CBCT) were requested, which showed presence of a residual root segment (high density mass) in the right submandibular region. The dislodged root was removed intraorally under general anesthesia without any postoperative complication. Conclusion: Displacement of tooth/tooth fragments into anatomical spaces after molar extraction can be avoided by adequate preoperative evaluation of patient and adoption of a meticulous surgical technique by an expert oral surgeon. Key Words: Molar; Mandible; Tooth Extraction; Tooth Root |
Introduction
Displacement of a tooth or part of it into the adjacent anatomical structures is a serious complication that may occur during surgical removal of third molars. It can result in infection, alveolar osteitis, dysesthesia, hemorrhage, and paresthesia [1]. The maxillary sinuses and the submandibular space are the most common sites of displacement [2]. Tooth displacement may occur as the result of anatomical variations such as distolingual angulation of teeth or lingual cortical plate dehiscence, or improper manipulation, excessive or uncontrolled force application, or inadequate preoperative clinical and radiographic examinations [3].
Case Presentation
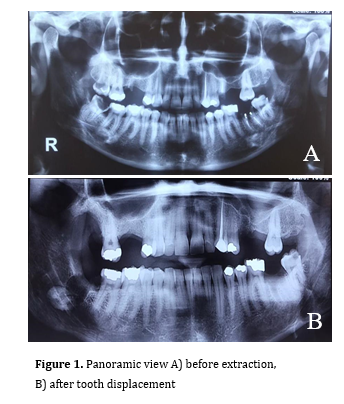
A 46-year-old Iranian female was referred by a dentist to Isfahan Azad University, Faculty of Dentistry, Oral and Maxillofacial Surgery Department, for management of a displaced mandibular right third molar root into the submandibular space 2 weeks earlier. The patient signed informed consent form before the procedure. The patient reported that the tooth broke during extraction and the dentist tried to remove the residual root segment with a cow-horn forceps but accidently the root was pushed into the submandibular space. The patient described the procedure as difficult and complicated. On clinical examination, slight swelling of the floor of the mouth in the right side was noted. The patient reported discomfort during swallowing with no sign of pus or infection and a history of one-week trismus after unsuccessful extraction. She could open her mouth with slight pain and discomfort within the range of normal maximum mouth opening. She had two panoramic radiographs with her. One had been taken before the extraction procedure (Figure 1A) and the other one had been taken after the incident showing the displaced root in the right submandibular space (Figure 1B). There was no palpable mass in the posterior region of the floor of the mouth.
Figure 1. Panoramic view A) before extraction, B) after tooth displacement
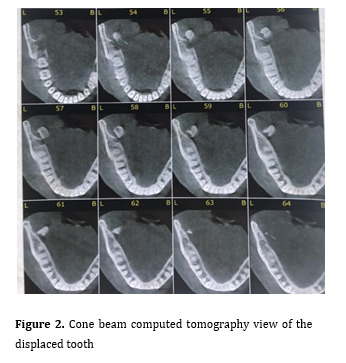
Radiographic examination was completed by ordering a cone beam computed tomography, and axial and coronal sections were evaluated (Figure 2), which showed a radiopaque lesion similar to the appearance of a third molar tooth root located in the right submandibular region.
The patient consented to surgical removal of the mass under general anesthesia. It was planned to first attempt intraoral removal of the root, and if the attempt was unsuccessful, then try to remove it through an extra-oral submandibular approach.
Figure 2. Cone beam computed tomography view of the displaced tooth
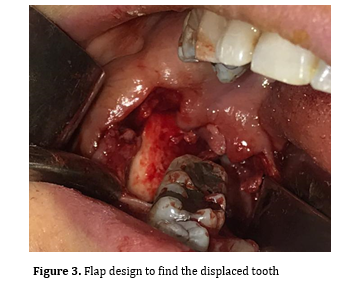
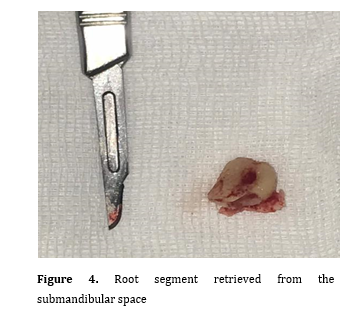
Under general anesthesia, an incision was made starting from the buccal sulcus towards the distolingual angle of the second molar. It was extended at the gingival margin to the coronoid process. Another incision was made in the lingual gingival margin of second molar (Figure 3). Blunt dissection was done until a sign of root mass was observed. Then, with a medium size spoon-shaped curette, the root was stabilized from the bottom in order not to be dislocated more in the anatomical space, and then it was grasped with a pair of artery forceps (Figure 4). The region was sutured with 4-0 vicryl sutures. The patient was given 500 mg cephalexin and 200 mg ibuprofen for 1 week. The postoperative course was uneventful, and the patient was asymptomatic at the 2-month follow-up visit.
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Figure 3. Flap design to find the displaced tooth
Figure 4. Root segment retrieved from the submandibular space
Discussion
In surgical extractions, the whole tooth or part of it may be dislodged and disappear as seen in our case. The patient may swallow it, or it may slip into the soft tissue or pharynx in the worst-case scenario.
Displacement of a mandibular third molar or part of it into the adjacent anatomical spaces during its extraction is a rare complication [4]. The sublingual, submandibular, and pterygomandibular spaces are the most common sites of dislodgment of an impacted mandibular third molar or its fragments [5]. In present case, the tooth had slipped into the submandibular space. Literature is scarce regarding tooth displacement into the submandibular space. However, it may occur due to incorrect surgical technique, lingual location of the tooth, or fenestration of the lingual cortical plate with subsequent root exposure. The incidence of this complication is reportedly < 1% [4]. In a literature review by Huang et al. [6], it was reported that out of five tissue spaces, the submandibular space was most commonly involved. Lingual plate fracture or perforation during extraction is the most common cause of this complication.
Application of excessive pressure with elevators may push the root deep into the adjacent anatomical spaces. Attempts to remove the fragment without sufficient vision and lack of surgical skills often lead to further and deeper displacement of the tooth or root fragment. Hence, such cases must be immediately referred to an expert oral surgeon. A CT scan may be requested if the fragment is not palpable and the panoramic or occlusal radiographs are inconclusive [4]. Three-dimensional reconstruction with a multi-slice CT has the added advantage of revealing the tooth/ fragment position and its anatomical relations as was done in our case [5].
The management plan for teeth displaced into the submandibular space depends on the size and palpability of the tooth/ fragment. When a tooth slips away in the process of extraction, it may be immediately stabilized by placing a finger over the medial side. The extraction socket may be subsequently widened with the support of a fissure bur to avoid inferior alveolar nerve canal and the tooth being teased back through the socket. The fragment may also be removed by elevation of an intraoral flap; in case of failure, extraoral approach may be adopted through a submandibular incision. In a modified approach, an osteotomy of the lingual plate is performed to retrieve the tooth/fragment [6, 7]. In our case, the surgeon approached the tooth through the fractured lingual plate using artery forceps in one hand while palpating the location of the tooth lingually by another hand. Once the tooth was locked by the forceps, it was removed. Hence, the adopted technique may vary depending on the location, size of tooth/fragment, and level of expertise of the surgeon.
Anesthesia, paresthesia, or dysesthesia are more serious sequelae of a complicated tooth extraction in case of traumatization of inferior alveolar nerve or lingual nerve. Taste could be altered if the lingual nerve is damaged. The sensation could improve over a period of time but there is also a greater chance that it may not improve [8]. Lingual nerve injury during third molar surgical extraction may occur due to anatomical proximity of the tooth to the nerve, separated by just the periosteum. The sensory disturbances following nerve injury can be troublesome and are a common cause of medico-legal litigations [9]. In our case, fortunately the lingual nerve remained intact and no sensory problems were reported by the patient.
Conclusion
Surgical extraction of mandibular third molars is a routine oral surgical procedure which can have complications such as nerve injury or displacement of tooth/tooth fragments into the adjacent tissues and anatomical spaces. Such complications can be avoided by adequate preoperative evaluation and adoption of a meticulous surgical technique by an expert oral surgeon.
Case Presentation
A 46-year-old Iranian female was referred by a dentist to Isfahan Azad University, Faculty of Dentistry, Oral and Maxillofacial Surgery Department, for management of a displaced mandibular right third molar root into the submandibular space 2 weeks earlier. The patient signed informed consent form before the procedure. The patient reported that the tooth broke during extraction and the dentist tried to remove the residual root segment with a cow-horn forceps but accidently the root was pushed into the submandibular space. The patient described the procedure as difficult and complicated. On clinical examination, slight swelling of the floor of the mouth in the right side was noted. The patient reported discomfort during swallowing with no sign of pus or infection and a history of one-week trismus after unsuccessful extraction. She could open her mouth with slight pain and discomfort within the range of normal maximum mouth opening. She had two panoramic radiographs with her. One had been taken before the extraction procedure (Figure 1A) and the other one had been taken after the incident showing the displaced root in the right submandibular space (Figure 1B). There was no palpable mass in the posterior region of the floor of the mouth.
Figure 1. Panoramic view A) before extraction, B) after tooth displacement
{kind=link}
Radiographic examination was completed by ordering a cone beam computed tomography, and axial and coronal sections were evaluated (Figure 2), which showed a radiopaque lesion similar to the appearance of a third molar tooth root located in the right submandibular region.
The patient consented to surgical removal of the mass under general anesthesia. It was planned to first attempt intraoral removal of the root, and if the attempt was unsuccessful, then try to remove it through an extra-oral submandibular approach.
Figure 2. Cone beam computed tomography view of the displaced tooth
{kind=link}
Under general anesthesia, an incision was made starting from the buccal sulcus towards the distolingual angle of the second molar. It was extended at the gingival margin to the coronoid process. Another incision was made in the lingual gingival margin of second molar (Figure 3). Blunt dissection was done until a sign of root mass was observed. Then, with a medium size spoon-shaped curette, the root was stabilized from the bottom in order not to be dislocated more in the anatomical space, and then it was grasped with a pair of artery forceps (Figure 4). The region was sutured with 4-0 vicryl sutures. The patient was given 500 mg cephalexin and 200 mg ibuprofen for 1 week. The postoperative course was uneventful, and the patient was asymptomatic at the 2-month follow-up visit.
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Figure 3. Flap design to find the displaced tooth
{kind=link}
Figure 4. Root segment retrieved from the submandibular space
{kind=link}
Discussion
In surgical extractions, the whole tooth or part of it may be dislodged and disappear as seen in our case. The patient may swallow it, or it may slip into the soft tissue or pharynx in the worst-case scenario.
Displacement of a mandibular third molar or part of it into the adjacent anatomical spaces during its extraction is a rare complication [4]. The sublingual, submandibular, and pterygomandibular spaces are the most common sites of dislodgment of an impacted mandibular third molar or its fragments [5]. In present case, the tooth had slipped into the submandibular space. Literature is scarce regarding tooth displacement into the submandibular space. However, it may occur due to incorrect surgical technique, lingual location of the tooth, or fenestration of the lingual cortical plate with subsequent root exposure. The incidence of this complication is reportedly < 1% [4]. In a literature review by Huang et al. [6], it was reported that out of five tissue spaces, the submandibular space was most commonly involved. Lingual plate fracture or perforation during extraction is the most common cause of this complication.
Application of excessive pressure with elevators may push the root deep into the adjacent anatomical spaces. Attempts to remove the fragment without sufficient vision and lack of surgical skills often lead to further and deeper displacement of the tooth or root fragment. Hence, such cases must be immediately referred to an expert oral surgeon. A CT scan may be requested if the fragment is not palpable and the panoramic or occlusal radiographs are inconclusive [4]. Three-dimensional reconstruction with a multi-slice CT has the added advantage of revealing the tooth/ fragment position and its anatomical relations as was done in our case [5].
The management plan for teeth displaced into the submandibular space depends on the size and palpability of the tooth/ fragment. When a tooth slips away in the process of extraction, it may be immediately stabilized by placing a finger over the medial side. The extraction socket may be subsequently widened with the support of a fissure bur to avoid inferior alveolar nerve canal and the tooth being teased back through the socket. The fragment may also be removed by elevation of an intraoral flap; in case of failure, extraoral approach may be adopted through a submandibular incision. In a modified approach, an osteotomy of the lingual plate is performed to retrieve the tooth/fragment [6, 7]. In our case, the surgeon approached the tooth through the fractured lingual plate using artery forceps in one hand while palpating the location of the tooth lingually by another hand. Once the tooth was locked by the forceps, it was removed. Hence, the adopted technique may vary depending on the location, size of tooth/fragment, and level of expertise of the surgeon.
Anesthesia, paresthesia, or dysesthesia are more serious sequelae of a complicated tooth extraction in case of traumatization of inferior alveolar nerve or lingual nerve. Taste could be altered if the lingual nerve is damaged. The sensation could improve over a period of time but there is also a greater chance that it may not improve [8]. Lingual nerve injury during third molar surgical extraction may occur due to anatomical proximity of the tooth to the nerve, separated by just the periosteum. The sensory disturbances following nerve injury can be troublesome and are a common cause of medico-legal litigations [9]. In our case, fortunately the lingual nerve remained intact and no sensory problems were reported by the patient.
Conclusion
Surgical extraction of mandibular third molars is a routine oral surgical procedure which can have complications such as nerve injury or displacement of tooth/tooth fragments into the adjacent tissues and anatomical spaces. Such complications can be avoided by adequate preoperative evaluation and adoption of a meticulous surgical technique by an expert oral surgeon.
Type of Study: Case report |
Subject:
Oral & maxillofacial surgery
References
1. Goldberg MH, Nemarich AN, Marco WP 2nd. Complications after mandibular third molar surgery: a statistical analysis of 500 consecutive procedures in private practice. J Am Dent As-soc. 1985 Aug;111(2):277-9. [DOI:10.14219/jada.archive.1985.0098]
2. Ozyuvaci H, Firat D, Tanyel C. Accidental displacement of a mandibular third molar: a case report. Quintessence Int. 2003 Apr;34(4):278-80.
3. Esen E, Aydoğan LB, Akçali MC. Accidental displacement of an impacted mandibular third molar into the lateral pharyngeal space. J Oral Maxillofac Surg. 2000 Jan;58(1):96-7. [DOI:10.1016/S0278-2391(00)80024-5] [PMID]
4. Kose I, Koparal M, Güneş N, Atalay Y, Yaman F, Atilgan S, Kaya G. Displaced lower third molar tooth into the submandibular space: Two case reports. J Nat Sci Biol Med. 2014 Jul;5(2):482-4. [DOI:10.4103/0976-9668.136274] [PMID] [PMCID]
5. Jolly SS, Rattan V, Rai SK. Intraoral management of displaced root into submandibular space under local anaesthesia -A case report and review of literature. Saudi Dent J. 2014 Oct;26(4):181-4. [DOI:10.1016/j.sdentj.2014.05.004] [PMID] [PMCID]
6. Huang IY, Wu CW, Worthington P. The displaced lower third molar: a literature review and suggestions for management. J Oral Maxillofac Surg. 2007 Jun;65(6):1186-90. [DOI:10.1016/j.joms.2006.11.031] [PMID]
7. Silveira RJ, Garcia RR, Botelho TL, Franco A, Silva RF. Accidental displacement of third molar into the sublingual space: a case report. J Oral Maxillofac Res. 2014 Oct 1;5(3): e5. [DOI:10.5037/jomr.2014.5305] [PMID] [PMCID]
8. Scrivani SJ, Moses M, Donoff RB, Kaban LB. Taste perception after lingual nerve repair. J Oral Maxillofac Surg. 2000 Jan;58(1):3-5; discussion 5-6. [DOI:10.1016/S0278-2391(00)80003-8] [PMID]
9. Hamed MS, Prasad P. Displacement of lower third molar to Submandibular fossa during extraction. Indian J Multidiscip Dent. 2016;6(2):107-10. [DOI:10.4103/2229-6360.197769]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |