Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 2 (4-2023)
J Res Dent Maxillofac Sci 2023, 8(2): 95-101 |
Back to browse issues page


Ethics code: IR.IAU.DENTAL.REC.1398.31
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Soleimani M, Amini N, Askarizadeh N. Association of Body Mass Index and DMFT/dmft in Children Aged 6-12 Years. J Res Dent Maxillofac Sci 2023; 8 (2) :95-101
URL: http://jrdms.dentaliau.ac.ir/article-1-378-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-378-en.html



1- Private Dentistry Practice, Mazandaran, Iran
2- Community Dental Health Department, Faculty of dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Pediatric Department, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
2- Community Dental Health Department, Faculty of dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Pediatric Department, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
Full-Text [PDF 666 kb]
(1466 Downloads)
| Abstract (HTML) (4350 Views)
Introduction
Considering the importance of oral health in children, it is important to find factors affecting it. Eating habits, body mass index (BMI), and educational level and socioeconomic status of the parents have been suggested as factors affecting oral health [1,2]. Dental caries is the most common oral infectious disease in children with a prevalence 5 times higher than asthma and 7 times higher than typhoid [3]. Based on the results of a national oral health developmental program for primary school students, the dmft (decayed, missing, and filled primary teeth) score of under 6-year-old children was 5.84 in 2016 [4]. Vargas and colleagues reported the prevalence of dental caries to be 27.4% in pre-school children, and 61% in 6-12-year-old children, and reported that dental caries caused problems in eating, sleeping and learning of children [5]. Neglect in treatment of dental caries leads to severe toothache and can result in further problems such as missing school days, family stress, and missing work days by the parents [3,6].
Obesity in children and adolescents is a serious dilemma in the 21st century and a critical general health problem worldwide. According to a report by the World Health Organization, the global prevalence of obesity and overweight in children increased from 2.4% in 1990 to 7.6% in 2010 (60% rise). In 2004, the national prevalence of obesity in 6-18-year-old males and females was 3.34 (range 3%-3.69%) and 3.50 (range 3.15%-3.87%), respectively. In 2010, these values increased to 13.58 (range 12.59%-14.63%), and 7.68 (range 6.71%-8.72%), respectively. In 2012, these values further increased to 13.58 (range 12.59%- 14.63%), and 10.15 (9.27%-11.09%), respectively [7].
The relationship of dental caries and BMI has been assessed in different countries with contradictory results. In some developed countries, various meals and high consumption of carbohydrates are known as the main causes of obesity and dental caries, and the reverse is true in some developing countries [1,6 ,8 ,9]. Dental caries is known as an etiologic factor for malnutrition [6]. Evidence shows that most obese children consume foods rich in fat and carbohydrates instead of fruits and vegetables [6,8,10]. Therefore, diet of obese children might be a risk factor for obesity and dental caries [11]. On the other hand, unhealthy nutrition leads to weight loss, short height, and eventual reduction of BMI [6]. Evidence shows that underweight children usually have malnutrition such as vitamin A, vitamin D, calcium and phosphorous deficiency which can adversely impact their tooth eruption and morphology, and increase the risk of dental caries [9]. Based on the existing controversy regarding the relationship of dental caries and BMI [1,6,8,9], and less attention paid to the relationship of underweight and caries, this study aimed to assess the correlation of BMI and dmft/DMFT in children aged 6-12 years.
Materials and Methods
This analytical descriptive study was carried out on 300 children aged 6-12 years who were selected among those referred to the Pediatric Dentistry and Orthodontics Departments of Tehran Islamic Azad University by simple random sampling. This study was approved by the Ethics committee of Tehran Medical Sciences, Islamic Azad University (IR.IAU.DENTAL.REC.1398.031).
After explaining the purpose of the study, written consent was obtained from the parents, and a questionnaire was filled out by the parents which included information regarding age, level of education, and occupation of the parents, number of family members, medical history, frequency of dental visits, oral and dental health status, diet of child during infancy period, and frequency of daily consumption of sugary foods and drinks. The inclusion criteria were minimum of 6 years of age and lack of any systemic disease affecting the child's growth such as diabetes mellitus, hyperthyroidism, hypothyroidism, and renal disorders [11]. Oral and dental examination was performed after a light breakfast consisting of a piece of bread and cheese and a glass of milk.
The children’s height was measured with a 2-meter wall mounted meter (Top Roll, China) without shoes. Children’s weight was measured in kilograms with one decimal using a calibrated digital scale (Ophogh, Iran) with light clothes and without shoes. BMI was calculated as weight in kilograms divided by height in square meters [12]. The scale was calibrated at the beginning of each working day. According to the percentile chart by gender presented by the Center for Disease Control and Prevention [13], age is identified on the longitudinal axis and BMI is identified on the vertical axis. The intersection of these two axes indicates the child’s position in the chart. Accordingly, the children were assigned to four groups. The percentile above 95 indicated obesity, between 85 to 95 indicated overweight, between 5 to 85 indicated normal weight, and the percentile below 5 indicated underweight. In this study, in order to increase the accuracy of the procedure, the BMI calculator presented by the Center for Disease Control and Prevention was used [14].
World Health Organization (WHO) instructions [15]. Accordingly, children rinsed their mouth with water and sat on dental chair. Examination was done by using a dental mirror, an explorer, disposable gloves, and sterile gauze to dry teeth. Based on the criteria presented by the WHO [16] current caries was defined as soft surfaces or lost enamel at the pits and fissures or smooth surfaces. Teeth with restorations are also included in this classification [13].
Decayed teeth, missing and filled primary (dmft) and permanent teeth (DMFT) were recorded and calculated [6].
To evaluate the association between dmft/DMFT index and parents’ educational level and income, oral health behavior, and diet, the Pearson’s correlation coefficient was used. To assess the variables of caries index and BMI, linear regression analysis with 95% confidence interval was applied. P<0.05 was considered significant. Data were analyzed by SPSS version 25 (SPSS Inc., IL, USA).
Results
In this study, 168 (56%) girls and 132 (44%) boys were assessed. The results showed that 71.3% of children brushed their teeth at least once a day and 22% used dental floss. Nearly half of children consumed sugary snacks (chocolate, candy, etc.) twice a day and a high percentage (77%) was breastfed during infancy. About half of the parents had academic education and most mothers (76.6%) were housewives; 62% of fathers were categorized as low-income.
Of all children, 60.67% were normal weight, 11.34% were underweight, 15.33% were overweight, and 12.66% were obese. The mean dmft was 4.66±3.39 and the mean DMFT was 1.44±1.57.
As shown in Table 1, the association between BMI and dmft (P=0.383) and DMFT (P=0.414) was not significant. A significant correlation was only found between BMI and the rate of caries in permanent teeth (P=0.046).
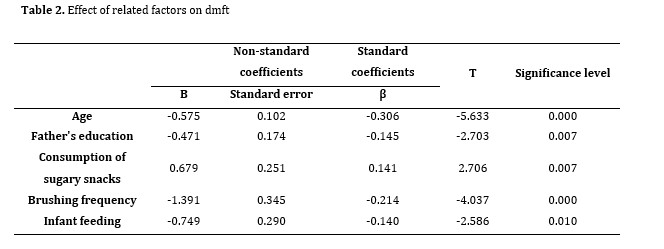
By an increase in age and in late mixed dentition period, dmft significantly decreased (P=0.000). Moreover, in children of the same age, as the educational level of fathers increased, dmft decreased (P=0.007). Higher consumption of sugary snacks increased dmft while increased frequency of toothbrushing decreased dmft (P=0.000). Children who were breastfed during infancy had lower dmft (P=0.010). Contrary to the impact of age on dmft, by increasing age, DMFT significantly increased (P=0.000). Low income, unemployed father (P=0.015), and higher number of children increased DMFT. By improved oral hygiene and increased frequency of toothbrushing and dental visits, DMFT significantly decreased (P=0.012, Tables 2 and 3).
Table 1. Correlation coefficient of DMFT and dmft indices with BMI
Full-Text: (1467 Views)
| Abstract
Background and Aim: Considering the importance of oral health in children, it is important to find factors affecting it. Eating habits, body mass index (BMI), and educational level and socioeconomic status of the parents have been suggested as factors affecting oral health. Two important indices for evaluation of general and oral health of children are the BMI and DMFT/dmft, respectively. The purpose of this study was to assess the relationship between these two indices in children aged 6-12 years. Materials and Methods: In this descriptive analytical study, 300 children aged 6-12 years were selected among those referred to the Dental Branch of Tehran Islamic Azad University of Medical Science in 2019-2020 by simple random sampling. The BMI and dmft/DMFT were calculated, and the relationship between them and the effect of influential factors on dental caries score were evaluated. Data were analyzed by the linear regression model at a confidence interval of 95% and 0.05 level of statistical significance. Results: The study sample consisted of 168 girls and 132 boys. The mean dmft was 4.66±3.39 and the mean DMFT was 1.44±1.57 Only 11.34% of the children were underweight and 12.66% were obese; while, 60.67% had a normal weight. Oral health and nutritional behaviors of children showed that 71.3% of them brushed their teeth at least once a day and only 22% used dental floss. A correlation was found between BMI and the rate of caries in permanent teeth (P=0.046). Conclusion: No statistically significant association was observed between dmft/DMFT and BMI of children aged 6-12 years. Key Words: Body Mass Index; Dental caries; Child; DMF Index |
Introduction
Considering the importance of oral health in children, it is important to find factors affecting it. Eating habits, body mass index (BMI), and educational level and socioeconomic status of the parents have been suggested as factors affecting oral health [1,2]. Dental caries is the most common oral infectious disease in children with a prevalence 5 times higher than asthma and 7 times higher than typhoid [3]. Based on the results of a national oral health developmental program for primary school students, the dmft (decayed, missing, and filled primary teeth) score of under 6-year-old children was 5.84 in 2016 [4]. Vargas and colleagues reported the prevalence of dental caries to be 27.4% in pre-school children, and 61% in 6-12-year-old children, and reported that dental caries caused problems in eating, sleeping and learning of children [5]. Neglect in treatment of dental caries leads to severe toothache and can result in further problems such as missing school days, family stress, and missing work days by the parents [3,6].
Obesity in children and adolescents is a serious dilemma in the 21st century and a critical general health problem worldwide. According to a report by the World Health Organization, the global prevalence of obesity and overweight in children increased from 2.4% in 1990 to 7.6% in 2010 (60% rise). In 2004, the national prevalence of obesity in 6-18-year-old males and females was 3.34 (range 3%-3.69%) and 3.50 (range 3.15%-3.87%), respectively. In 2010, these values increased to 13.58 (range 12.59%-14.63%), and 7.68 (range 6.71%-8.72%), respectively. In 2012, these values further increased to 13.58 (range 12.59%- 14.63%), and 10.15 (9.27%-11.09%), respectively [7].
The relationship of dental caries and BMI has been assessed in different countries with contradictory results. In some developed countries, various meals and high consumption of carbohydrates are known as the main causes of obesity and dental caries, and the reverse is true in some developing countries [1,6 ,8 ,9]. Dental caries is known as an etiologic factor for malnutrition [6]. Evidence shows that most obese children consume foods rich in fat and carbohydrates instead of fruits and vegetables [6,8,10]. Therefore, diet of obese children might be a risk factor for obesity and dental caries [11]. On the other hand, unhealthy nutrition leads to weight loss, short height, and eventual reduction of BMI [6]. Evidence shows that underweight children usually have malnutrition such as vitamin A, vitamin D, calcium and phosphorous deficiency which can adversely impact their tooth eruption and morphology, and increase the risk of dental caries [9]. Based on the existing controversy regarding the relationship of dental caries and BMI [1,6,8,9], and less attention paid to the relationship of underweight and caries, this study aimed to assess the correlation of BMI and dmft/DMFT in children aged 6-12 years.
Materials and Methods
This analytical descriptive study was carried out on 300 children aged 6-12 years who were selected among those referred to the Pediatric Dentistry and Orthodontics Departments of Tehran Islamic Azad University by simple random sampling. This study was approved by the Ethics committee of Tehran Medical Sciences, Islamic Azad University (IR.IAU.DENTAL.REC.1398.031).
After explaining the purpose of the study, written consent was obtained from the parents, and a questionnaire was filled out by the parents which included information regarding age, level of education, and occupation of the parents, number of family members, medical history, frequency of dental visits, oral and dental health status, diet of child during infancy period, and frequency of daily consumption of sugary foods and drinks. The inclusion criteria were minimum of 6 years of age and lack of any systemic disease affecting the child's growth such as diabetes mellitus, hyperthyroidism, hypothyroidism, and renal disorders [11]. Oral and dental examination was performed after a light breakfast consisting of a piece of bread and cheese and a glass of milk.
The children’s height was measured with a 2-meter wall mounted meter (Top Roll, China) without shoes. Children’s weight was measured in kilograms with one decimal using a calibrated digital scale (Ophogh, Iran) with light clothes and without shoes. BMI was calculated as weight in kilograms divided by height in square meters [12]. The scale was calibrated at the beginning of each working day. According to the percentile chart by gender presented by the Center for Disease Control and Prevention [13], age is identified on the longitudinal axis and BMI is identified on the vertical axis. The intersection of these two axes indicates the child’s position in the chart. Accordingly, the children were assigned to four groups. The percentile above 95 indicated obesity, between 85 to 95 indicated overweight, between 5 to 85 indicated normal weight, and the percentile below 5 indicated underweight. In this study, in order to increase the accuracy of the procedure, the BMI calculator presented by the Center for Disease Control and Prevention was used [14].
World Health Organization (WHO) instructions [15]. Accordingly, children rinsed their mouth with water and sat on dental chair. Examination was done by using a dental mirror, an explorer, disposable gloves, and sterile gauze to dry teeth. Based on the criteria presented by the WHO [16] current caries was defined as soft surfaces or lost enamel at the pits and fissures or smooth surfaces. Teeth with restorations are also included in this classification [13].
Decayed teeth, missing and filled primary (dmft) and permanent teeth (DMFT) were recorded and calculated [6].
To evaluate the association between dmft/DMFT index and parents’ educational level and income, oral health behavior, and diet, the Pearson’s correlation coefficient was used. To assess the variables of caries index and BMI, linear regression analysis with 95% confidence interval was applied. P<0.05 was considered significant. Data were analyzed by SPSS version 25 (SPSS Inc., IL, USA).
Results
In this study, 168 (56%) girls and 132 (44%) boys were assessed. The results showed that 71.3% of children brushed their teeth at least once a day and 22% used dental floss. Nearly half of children consumed sugary snacks (chocolate, candy, etc.) twice a day and a high percentage (77%) was breastfed during infancy. About half of the parents had academic education and most mothers (76.6%) were housewives; 62% of fathers were categorized as low-income.
Of all children, 60.67% were normal weight, 11.34% were underweight, 15.33% were overweight, and 12.66% were obese. The mean dmft was 4.66±3.39 and the mean DMFT was 1.44±1.57.
As shown in Table 1, the association between BMI and dmft (P=0.383) and DMFT (P=0.414) was not significant. A significant correlation was only found between BMI and the rate of caries in permanent teeth (P=0.046).
By an increase in age and in late mixed dentition period, dmft significantly decreased (P=0.000). Moreover, in children of the same age, as the educational level of fathers increased, dmft decreased (P=0.007). Higher consumption of sugary snacks increased dmft while increased frequency of toothbrushing decreased dmft (P=0.000). Children who were breastfed during infancy had lower dmft (P=0.010). Contrary to the impact of age on dmft, by increasing age, DMFT significantly increased (P=0.000). Low income, unemployed father (P=0.015), and higher number of children increased DMFT. By improved oral hygiene and increased frequency of toothbrushing and dental visits, DMFT significantly decreased (P=0.012, Tables 2 and 3).
Table 1. Correlation coefficient of DMFT and dmft indices with BMI
{kind=link}
{kind=link}
Table 3. Effect of related factors on DMFT
Discussion
Several factors are related to dental caries such as genetic factors, type of diet, toothbrushing, socioeconomic status of the family, and overweight and obesity [17]. In this study, a significant correlation between dmft/DMFT index and BMI was not observed (P=0.414 and P=0.383, respectively). However, factors like age, educational level, father’s income, frequency of toothbrushing, sugary snack consumption, and frequency of dental visits affected the rate of caries. Accordingly, the relationship of dental caries and BMI was declined in this study.
By an increase in age and in late mixed dentition period, dmft significantly decreased but unlike the effect of age on dmft, DMFT significantly increased with age. In this study, the mean dmft was 4.66±3.39 which was in agreement with the reported dmft in studies by Edalat and colleagues (dmft=4.13±3.48) [2] and Malek Mohammadi et al. (dmft=4.70±3.4) [6], in other parts of Iran. Likewise, the mean DMFT in the present study was 1.44±1.57, which was similar to a study by Goodarzi et al., (1.03) in 2019 in Tehran [18].
In the current study, most children were normal weight (60.67%) which was in harmony with the results of previous studies in other parts of Iran. As in studies by Sadeghi and Roberts [19], Malek Mohammadi et al., [6] Bafti et al., [11] and Bahrololoomi and colleagues [17] the majority of children had a normal weight.
In this study, children who were breastfed during infancy had a lower dmft. The results of a cross-sectional study by Porhashemi et al. also indicated that type of nutrition during the first 2 years of life and technique of breastfeeding or bottle feeding affected the occurrence of early childhood caries [9].
Based on the findings of the present study, by increased consumption of sugary snacks, dmft increased while higher frequency of toothbrushing decreased dmft/DMFT. A cross-sectional study by Bahroloolomi and colleagues showed that consumption of cariogenic snacks and frequency of toothbrushing had significant effects on dental caries index [17].
In line with the present findings, de Jong-Lenters and colleagues assessed the relationship of dental carries and BMI in 230 children aged 5 to 8 years in Noordwijk (Netherlands). They did not find any significant difference in dmft between the 2 groups of overweight and non-overweight children [1]. Porhashemi and colleagues [9] in a case-control study on the relationship of childhood caries and BMI reported results similar to the present findings and found no significant difference in BMI between healthy children and those with early childhood caries. Almerich-Torres and colleagues did not indicate any link between obesity and carries index [8]. Edalat et al. in their descriptive-cross-sectional study in 2014 on 202 children did not find a significant relationship between dmft and height, weight, or BMI [2]. In contrast, some studies found a relationship between caries and BMI. Goodarzi and colleagues evaluated 416 students aged 10-12 years in Tehran, and found a significant association between dental caries and BMI [18]. Malek Mohammadi and colleagues also found a significant correlation between BMI and dental caries in 400 children aged 7 to 11 years in Kerman, Iran [6]. The results of a cross-sectional study by Bahrololoomi et al. on 400 children aged 7 to 11 years in Yazd indicated that 18% of children were overweight or at risk of weight gain, and the rate of dental caries index was significantly higher in them than in other children [17].
Some studies showed the inverse correlation of BMI and dental caries which was not in line with the present results. Bafti and colleagues evaluated 1,482 children in Kerman and showed that BMI had an inverse correlation with dmft index; whereas, in children with normal weight, the mean dmft was higher than that in overweight children [11]. A recent study by Cheng and colleagues in 2019, on more than one million Chinese students with a mean age of 10.5 years showed that children with weight lower than normal, had higher frequency of dental caries [20]. In 2016, Liang and colleagues in China evaluated 32,461 children, and indicated that higher BMI was correlated with lower risk of dental caries, such that obese children in their study had fewer carious teeth [21]. Norberg et al. in Sweden found similar results. However, obese or overweight children did not have higher frequency of dental caries compared with others, but dental caries was more prevalent in underweight children compared with normal weight children [22].
Variations in the reported literature could be due to differences in study designs and populations. The population of the present study comprised of children aged 6-12 years referred to two departments of a dental school, and due to restrictions caused by COVID-19, it was not possible to assess children in other regions of Tehran. In this study, equal number of boys and girls were recruited to eliminate the effect of gender. Moreover, in this study, in addition to the effect of obesity on dental caries, the effect of underweight was assessed as well. Application of WHO and Center for Disease Control criteria increased the accuracy of the present results. The difference between the present results and previous investigations could be due to the diversity of age, geographical location and also investigation of primary or mixed dentition period in different studies [6,11 ,17,21 ,22].
The results of studies that reported a significant correlation between obesity and dental caries should be carefully interpreted since most of them have a cross-sectional design, and a cause-and-effect relationship cannot be established in a cross-sectional design. In other words, there is a chance that consumption of sugar and sugary products increases both obesity and risk of dental caries, and by a change to a low-sugar diet, the BMI may return to normal, but dental caries remains. There is also a possibility that low values of DMFT are associated with high values of BMI, depending on when the examinations are performed [9]. This may particularly occur in young age groups, because growth and development and weight changes in children happen quickly and overweight and obesity can also be observed in them following diet changes. For this reason, it is necessary to control the diet and frequency of intake of carbohydrates in children to reduce the risk of dental caries in them [2]. Also, the role of confounding variables such as diet, socioeconomic status, age, oral hygiene status, and use of fluoride cannot be ignored.
Cross-sectional design was a limitation of this study, which does not allow to find a cause-and-effect relationship. Moreover, collected information was based on reports by parents. Future studies are required to assess the effect of weight loss on dental caries in children and adolescents. Also, further studies are recommended to assess the relationship of BMI and dental caries in a prospective (cohort) design.
Conclusion
A correlation between dmft/DMFT and BMI in children was not observed in the present study. Age, father’s income and educational level, frequency of tooth brushing, frequency of intake of sugary snacks, and also frequency of dental visits affected the prevalence of dental caries.
Acknowledgement
We would like to express our gratitude to the staff of the pediatric dentistry Department of Tehran Islamic Azad University and to all patients participating in this study.
{kind=link}
Discussion
Several factors are related to dental caries such as genetic factors, type of diet, toothbrushing, socioeconomic status of the family, and overweight and obesity [17]. In this study, a significant correlation between dmft/DMFT index and BMI was not observed (P=0.414 and P=0.383, respectively). However, factors like age, educational level, father’s income, frequency of toothbrushing, sugary snack consumption, and frequency of dental visits affected the rate of caries. Accordingly, the relationship of dental caries and BMI was declined in this study.
By an increase in age and in late mixed dentition period, dmft significantly decreased but unlike the effect of age on dmft, DMFT significantly increased with age. In this study, the mean dmft was 4.66±3.39 which was in agreement with the reported dmft in studies by Edalat and colleagues (dmft=4.13±3.48) [2] and Malek Mohammadi et al. (dmft=4.70±3.4) [6], in other parts of Iran. Likewise, the mean DMFT in the present study was 1.44±1.57, which was similar to a study by Goodarzi et al., (1.03) in 2019 in Tehran [18].
In the current study, most children were normal weight (60.67%) which was in harmony with the results of previous studies in other parts of Iran. As in studies by Sadeghi and Roberts [19], Malek Mohammadi et al., [6] Bafti et al., [11] and Bahrololoomi and colleagues [17] the majority of children had a normal weight.
In this study, children who were breastfed during infancy had a lower dmft. The results of a cross-sectional study by Porhashemi et al. also indicated that type of nutrition during the first 2 years of life and technique of breastfeeding or bottle feeding affected the occurrence of early childhood caries [9].
Based on the findings of the present study, by increased consumption of sugary snacks, dmft increased while higher frequency of toothbrushing decreased dmft/DMFT. A cross-sectional study by Bahroloolomi and colleagues showed that consumption of cariogenic snacks and frequency of toothbrushing had significant effects on dental caries index [17].
In line with the present findings, de Jong-Lenters and colleagues assessed the relationship of dental carries and BMI in 230 children aged 5 to 8 years in Noordwijk (Netherlands). They did not find any significant difference in dmft between the 2 groups of overweight and non-overweight children [1]. Porhashemi and colleagues [9] in a case-control study on the relationship of childhood caries and BMI reported results similar to the present findings and found no significant difference in BMI between healthy children and those with early childhood caries. Almerich-Torres and colleagues did not indicate any link between obesity and carries index [8]. Edalat et al. in their descriptive-cross-sectional study in 2014 on 202 children did not find a significant relationship between dmft and height, weight, or BMI [2]. In contrast, some studies found a relationship between caries and BMI. Goodarzi and colleagues evaluated 416 students aged 10-12 years in Tehran, and found a significant association between dental caries and BMI [18]. Malek Mohammadi and colleagues also found a significant correlation between BMI and dental caries in 400 children aged 7 to 11 years in Kerman, Iran [6]. The results of a cross-sectional study by Bahrololoomi et al. on 400 children aged 7 to 11 years in Yazd indicated that 18% of children were overweight or at risk of weight gain, and the rate of dental caries index was significantly higher in them than in other children [17].
Some studies showed the inverse correlation of BMI and dental caries which was not in line with the present results. Bafti and colleagues evaluated 1,482 children in Kerman and showed that BMI had an inverse correlation with dmft index; whereas, in children with normal weight, the mean dmft was higher than that in overweight children [11]. A recent study by Cheng and colleagues in 2019, on more than one million Chinese students with a mean age of 10.5 years showed that children with weight lower than normal, had higher frequency of dental caries [20]. In 2016, Liang and colleagues in China evaluated 32,461 children, and indicated that higher BMI was correlated with lower risk of dental caries, such that obese children in their study had fewer carious teeth [21]. Norberg et al. in Sweden found similar results. However, obese or overweight children did not have higher frequency of dental caries compared with others, but dental caries was more prevalent in underweight children compared with normal weight children [22].
Variations in the reported literature could be due to differences in study designs and populations. The population of the present study comprised of children aged 6-12 years referred to two departments of a dental school, and due to restrictions caused by COVID-19, it was not possible to assess children in other regions of Tehran. In this study, equal number of boys and girls were recruited to eliminate the effect of gender. Moreover, in this study, in addition to the effect of obesity on dental caries, the effect of underweight was assessed as well. Application of WHO and Center for Disease Control criteria increased the accuracy of the present results. The difference between the present results and previous investigations could be due to the diversity of age, geographical location and also investigation of primary or mixed dentition period in different studies [6,11 ,17,21 ,22].
The results of studies that reported a significant correlation between obesity and dental caries should be carefully interpreted since most of them have a cross-sectional design, and a cause-and-effect relationship cannot be established in a cross-sectional design. In other words, there is a chance that consumption of sugar and sugary products increases both obesity and risk of dental caries, and by a change to a low-sugar diet, the BMI may return to normal, but dental caries remains. There is also a possibility that low values of DMFT are associated with high values of BMI, depending on when the examinations are performed [9]. This may particularly occur in young age groups, because growth and development and weight changes in children happen quickly and overweight and obesity can also be observed in them following diet changes. For this reason, it is necessary to control the diet and frequency of intake of carbohydrates in children to reduce the risk of dental caries in them [2]. Also, the role of confounding variables such as diet, socioeconomic status, age, oral hygiene status, and use of fluoride cannot be ignored.
Cross-sectional design was a limitation of this study, which does not allow to find a cause-and-effect relationship. Moreover, collected information was based on reports by parents. Future studies are required to assess the effect of weight loss on dental caries in children and adolescents. Also, further studies are recommended to assess the relationship of BMI and dental caries in a prospective (cohort) design.
Conclusion
A correlation between dmft/DMFT and BMI in children was not observed in the present study. Age, father’s income and educational level, frequency of tooth brushing, frequency of intake of sugary snacks, and also frequency of dental visits affected the prevalence of dental caries.
Acknowledgement
We would like to express our gratitude to the staff of the pediatric dentistry Department of Tehran Islamic Azad University and to all patients participating in this study.
Type of Study: Original article |
Subject:
pediatric
References
1. de Jong-Lenters M, van Dommelen P, Schuller AA, Verrips EH. Body mass index and dental caries in children aged 5 to 8 years attending a dental paediatric referral practice in the Nether-lands. BMC Res Notes. 2015 Dec 1;8:738. [DOI:10.1186/s13104-015-1715-6] [PMID] [PMCID]
2. Edalat A, Abbaszadeh M, Eesvandi M, Heidari A. The Relationship of Severe Early Childhood Caries and Body Mass Index in a Group of 3- to 6-year-old Children in Shiraz. J Dent (Shiraz). 2014 Jun;15(2):68-73.
3. JA Dean, JE Jones, LA Walker Vinson, RE McDonald. Dentistry for the child and adolescent. 10th ed. St. Louis: Mosby Elsevier; 2016. pp.155.
4. Ministry of Health. Treatment and Medical Training, Results of Oral and Dental Surveys. Available from: https://www.skums.ac.ir/pageBehdasht/fa/19/form/pId21714.
5. Vargas CM, Crall JJ, Schneider DA. Sociodemographic distribution of pediatric dental caries: NHANES III, 1988-1994. J Am Dent Assoc. 1998;129:1229-1238. [DOI:10.14219/jada.archive.1998.0420] [PMID]
6. Malek Mohammadi T, Hossienian Z, Bakhteyar M. The associ-ation of body mass index with dental caries in an Iranian sample of children. Journal of Oral Health and Oral Epi-demiology. 2012;1(1): 29-35.
7. Djalalinia S , Kelishadi R , Qorbani M, Peykari N, Kasaeian A, Nasli-Esfahani E , et al. A Systematic Review on the Prevalence of Overweight and Obesity, in Iranian Children and Adolescents. Iran J Pediatr. 2016 May; 26(3):e2599. [DOI:10.5812/ijp.2599] [PMID] [PMCID]
8. Almerich-Torres T, Montiel-Company JM, Bellot-Arcís C, Almerich-Silla JM. Relationship between caries, body mass index and social class in Spanish children. Gac Sanit. 2017 Nov-Dec;31(6):499-504. [DOI:10.1016/j.gaceta.2016.09.005] [PMID]
9. Porhashemi J, Garshasby K G, Nahvi A. Relationship between Sever Early Childhood Caries and BMI in 2-4-Year-Old Children in Tehran Kindergartens. J Mazandaran Univ Med Sci. 2016; 26(140) :197-201.
10. Khazaei P, Hamedani-Golshan M, Hessari H.The caries pat-tern of primary teeth and its determinants among 5-7-year-old children in Tehran, Iran. Journal of Babol University of Medical Sciences. 2018; 7(3):118-25.
11. Bafti LS, Hashemipour MA, Poureslami H, Hoseinian Z. Rela-tionship between Body Mass Index and Tooth Decay in a Popu-lation of 3-6-Year-Old Children in Iran. Int J Dent. 2015;2015:126530. [DOI:10.1155/2015/126530] [PMID] [PMCID]
12. Khodadadi E, Khafri S. Epidemiological Evaluation of DMFT of first permanent Molar in 12 Year Old Student of Babol City Iran (2011-2012). Journal of Babol University of Medical Scienc-es.2013;15(5):102-6.
13. Centers for Disease Control and Prevention. BMI for children and teens. Available from: http://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.htmll.
14. Centers for Disease Control and Prevention. BMI Percentile Calculator for Child and Teen. Available from: https://www.cdc.gov/healthyweight/bmi/calculator.html.
15. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004 Jan 10;363(9403):157-63. [DOI:10.1016/S0140-6736(03)15268-3] [PMID]
16. World Health Organization. Oral Health Surveys, Basic Methods-5th edition. Available from: https://www.who. int/ publications/i/item/9789241548649.
17. Bahrololoomi Z, Soruri M, Rekabi M. Ravaei S. The Relationship between BMI and DMFT/dmft among 7-11 Year-old Children Yazd. J Shahid Sadoughi Univ Med Sci. 2014; 21(6): 751-8.
18. Goodarzi A, Heidarnia A, Tavafian SS, Eslami M. Association between Dental Caries and Body Mass Index-for-Age among 10-12-Year-Old Female Students in Tehran. Int J Prev Med. 2019 Mar 5;10:28. [DOI:10.4103/ijpvm.IJPVM_528_18] [PMID] [PMCID]
19. Sadeghi M, Roberts M. The Relationship between BMI-For-Age (BMI-%) and DMFT Index of 6-Year-Old Children in Rafsanjan, Iran. Int J Dent Oral Health. 2018; 2(2):175-191.
20. Cheng YH, Liao Y, Chen DY,Wang Y,Wu Y. Prevalence of dental caries and its association with body mass index among school-age children in Shenzhen, China. BMC Oral Health.2019; 19(1):270-9. [DOI:10.1186/s12903-019-0950-y] [PMID] [PMCID]
21. Liang JJ, Zhang ZQ, Chen YJ, et al. Dental caries is negatively correlated with body mass index among 7-9 years old children in Guangzhou, China. BMC public health.2016; 16(1): 638-45. [DOI:10.1186/s12889-016-3295-3] [PMID] [PMCID]
22. Norberg C, Hallström Stalin U, Matsson L, Thorngren-Jerneck K, Klingberg G. Body mass index (BMI) and dental caries in 5-year-old children from southern Sweden.Community Dent Oral Epidemiol. 2012 Aug;40(4):315-22. [DOI:10.1111/j.1600-0528.2012.00686.x] [PMID]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |