|
Abstract
Background and Aim: This study aimed to assess the bone thickness at the interradicular spaces in the anterior mandible on cone-beam computed tomography (CBCT) scans of patients to find appropriate sites for mini-implant and miniscrew placement.
Materials and Methods: This analytical cross-sectional study was conducted on 161 CBCT scans of patients (98 females and 63 males) between 18 to 50 years old presenting to the School of Dentistry of Islamic Azad University in 2020. Cross-sectional images with 1 mm slice thickness were evaluated to measure the bone thickness at the interradicular areas at 3, 6, 9, 12, 15, and 18 mm distance from the mandibular alveolar crest. The measurements made from the distal surface of right canine to the distal surface of left canine teeth were recorded. The CBCT scans had been taken by Rotograph Evo 3D CBCT scanner, and were analyzed by OnDemand3D software. Data were statistically analyzed by t-test.
Results: Bone thickness at 11 sites in the anterior mandible was significantly higher in males (P<0.05). By an increase in depth in both males and females, the mean thickness of bone increased (P<0.05). The maximum mean bone thickness in males and females was at 18 mm depth between the central incisors.
Conclusion: To find a correct site for mini-implant and miniscrew placement, it should be noted that bone thickness would be greater at deeper areas, and by moving from the premolar site towards the incisors.
Key Words: Mandible; Bone Screws; Cone-Beam Computed; Tomography
Introduction
Considering the increasing application of miniscrews for correction of dentoskeletal deformities, finding the most suitable place for their insertion is a challenge. If adequate attention is not paid to this topic, it may even lead to treatment failure. Ardani et al. [1] and Liu et al. [2] pointed to the important role of implant length, optimal bone density, and not invading the adjacent structures such as the periodontal ligament in miniscrew placement. Also, Woods et al. [3] discussed that success of implant and miniscrew placement depends not only on their correct positioning in bone, but also, on the time of placement and the magnitude of load applied during insertion. Thus, finding an appropriate site with optimal bone properties for miniscrew placement is imperative, and is a research priority.
Although many previous studies on this topic used cone-beam computed tomography (CBCT), they have differences regarding the type of variable studied to find the most appropriate site for miniscrew placement.[4-9] Chhatwani et al. [4], and Sugumaran et al. [6] evaluated the vertical bone height at different sites. Nucera et al. [7] evaluated the properties of mandibular cortical bone for miniscrew placement. Murugesan and Sivakumar [8] measured the bone thickness at different angulations and reported that it is an important factor for selection of an appropriate site for miniscrew insertion. Becker et al. [9] assessed the angle and location of miniscrew placement, irrespective of bone quality.
Interradicular space is another parameter to evaluate on CBCT scans to find a proper location for miniscrew placement. da Costa Sabec et al. [10] pointed to the significance of this topic. Although this topic has been the focus of many investigations, the results have been controversial in this regard. For instance, some studies suggested the anterior region of the arch for miniscrew placement for patients requiring exposure of impacted canines and intrusion of lower anterior teeth.[11,12] Some others suggested the inter-premolar and inter-molar spaces (between the first and second molars) for this purpose.[10] However, another study suggested miniscrew placement between premolars and in the subapical space in the anterior region.[13] Considering the existing controversies and the fact that most available studies on this topic focused on the posterior region [5,7] as well as the role of race in bone properties such as the thickness and dimensions of bone [14,15], this study aimed to assess the bone thickness in interradicular spaces in the anterior mandible on CBCT scans of patients presenting to Islamic Azad University, School of Dentistry, Tehran in 2020.
Materials and Methods
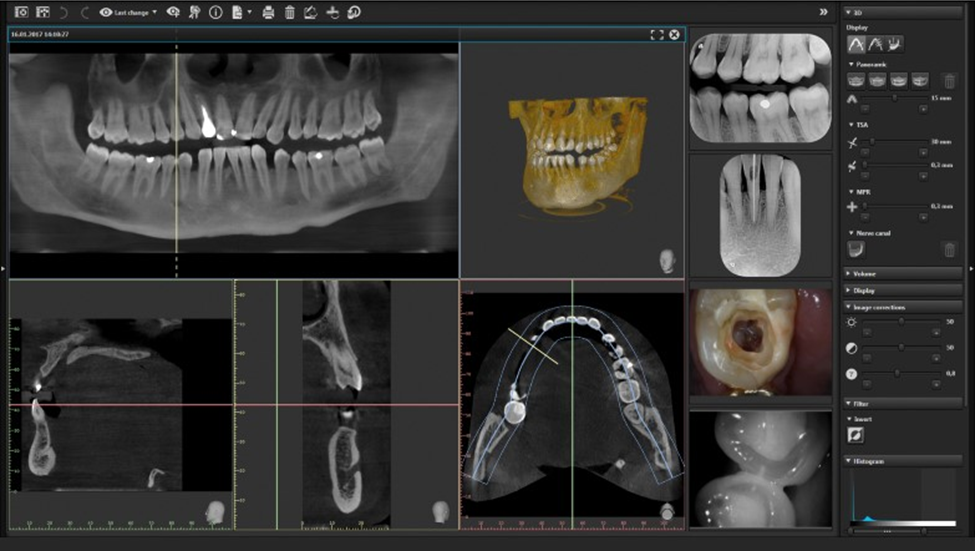
This analytical cross-sectional study was conducted on 161 patients (98 females, 63 males) between 18 to 50 years, presenting to the Radiology Department of Islamic Azad University, School of Dentistry, Tehran in 2020. The CBCT scans of patients were retrieved from the archives. The CBCT scans had been taken for purposes not related to this study. It should be noted that this number corresponded to almost all patients presenting to this department in 2020 (only a few were excluded since they did not meet the eligibility criteria). The inclusion criteria were no history of previous orthodontic treatment, and absence of maxillofacial defects visible on radiographs that would cause macroscopic deformity or asymmetry. CBCT scans of patients with no bone loss in the anterior mandible, normal root morphology, and presence of all six anterior teeth from the right to the left mandibular canine teeth were selected. The exclusion criteria were severe rotation of teeth, root deformity or resorption at the site, poor-quality and blurred scans, presence of alveolar bone defects at the site, and history of metabolic bone diseases (Figure 1).
The study was approved by the ethics committee of the university (IR.IAU.TMU.REC.1399.218). The CBCT scans had all been taken by Rotograph Evo 3D CBCT scanner (Villa Sistemi Medicali, Buccinasco MI, Italy) with the exposure settings of 85 kVp, 8 x 8 cm field of view, 9 mA, and 185 µm voxel size in standing position. The exposure parameters were the same for all patients, and CBCT scans had no artifacts. The measurements were made by one examiner using OnDemand 3D software (CyberMed Inc., Seoul, South Korea).[16-19] For this purpose, first the mandible was adjusted parallel to the horizontal axis in the software environment. To start sectioning, the arch line of each patient was drawn in the software and then cross-sectional slices were made with 1 mm slice interval.[17] The bone thickness at the interradicular areas was measured at 3, 6, 9, 12, 15, and 18 mm distances from the mandibular alveolar ridge crest.[5] (Figures 1 and 2) The values measured at the distal surface of the right canine, between the right canine and lateral incisor, between the right central and lateral incisors, between the two central incisors, between the left central and lateral incisors, between the left lateral incisor and canine, and at the distal of left canine were all recorded.[18] To assess the reliability of the measurements, 10% of the measurements were repeated by the same examiner again after 2 weeks.[16] Data were statistically analyzed using t-test and the Pearson’s correlation coefficient.
Figure 1. OnDemand 3D software environment
Figure 2. Measuring the bone thickness at 18 mm depth of interradicular space
Results
This study assessed the bone thickness in the anterior mandible at 3, 6, 9, 12, 15, and 18 mm distance from the ridge crest to find the best location for placement of miniscrews in 161 patients including 98 females and 63 males.
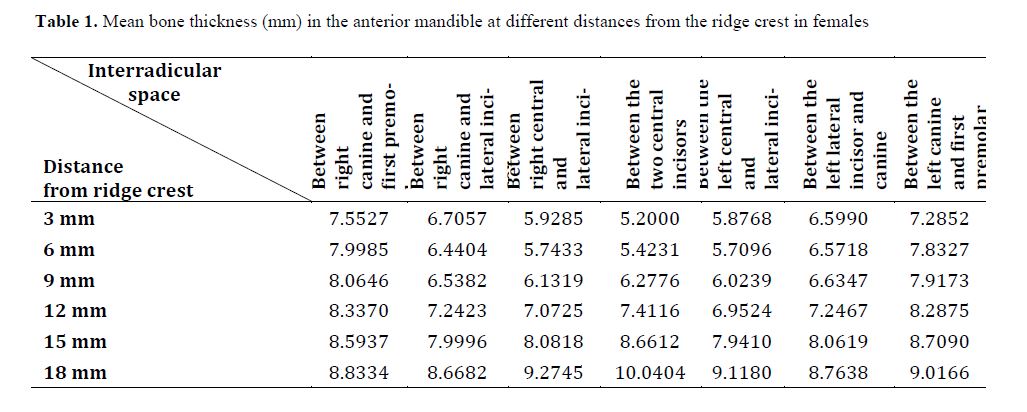
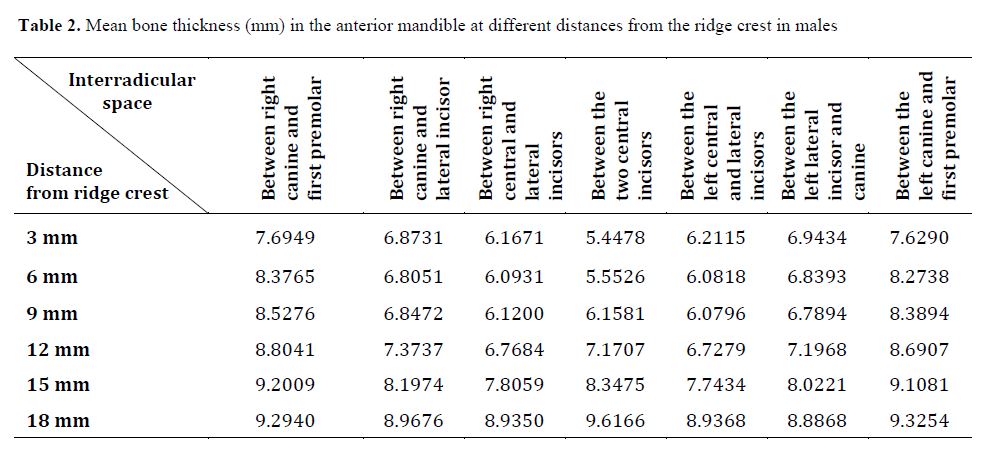
The results showed that some areas were significantly superior in terms of bone thickness for miniscrew placement, which are presented in Tables 1 and 2 based on gender.
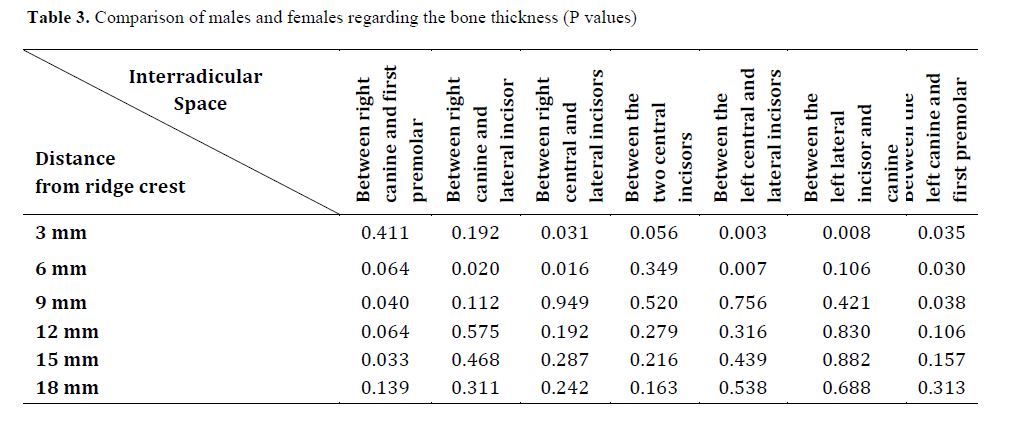
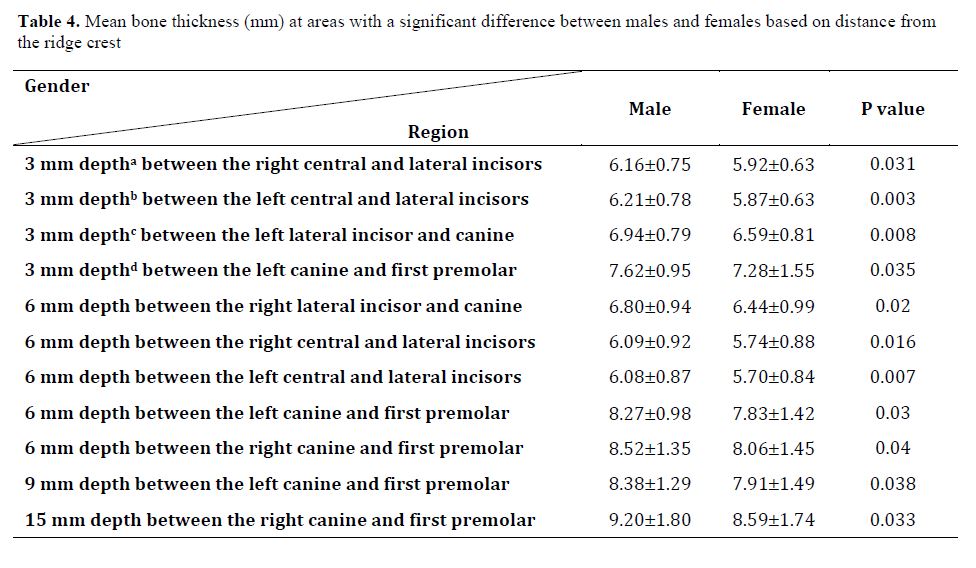
As shown in Table 3, bone thickness was significantly different in males and females (P<0.05) such that the bone thickness at some certain areas in the anterior mandible was significantly greater in males as shown in Table 4 (P<0.05). The difference was not significant in other areas (P>0.05).
The results of t-test showed that maximum thickness was at 18 mm depth between the central incisors in both females (9.61±1.94 mm) and males (10.04±1.82 mm).
With respect to age, only at 3 mm depth between the right lateral incisor and canine, significant changes were noted in bone thickness with age in both males and females (P=0.006). The Pearson’s correlation coefficient was found to be +0.217 for this correlation, indicating a significant direct correlation between age and alveolar bone width, which means that at 3 mm depth between the right lateral incisor and canine, by an increase in age, the bone thickness significantly increased (P=0.006).
Discussion
The current results showed that age and gender can affect the bone thickness in the anterior mandible at different depths. The thickest bone was found at the deepest measurement point. In other words, mandibular bone thickness had a direct correlation with depth. Lee et al. [13] aimed to find the most suitable point for mini-implant placement in the mandible, and showed that maximum bone
Table 1. Mean bone thickness (mm) in the anterior mandible at different distances from the ridge crest in females
Table 2. Mean bone thickness (mm) in the anterior mandible at different distances from the ridge crest in males
thickness was found at the deepest point evaluated. The results of Rossi et al, [15] also confirmed this finding. Moreover, Wang et al. [19] concluded that maximum bone thickness in the anterior mandible was found at the deepest point. However, they reported that bone thickness in the anterior mandible was minimum between the two central incisors, which was different from the present findings. It should be noted that Wang et al. [19] measured the bone thickness between the two central incisors at the periapical region, and reported it to be minimum while we found that the bone thickness was maximum at the deepest point measured between the two central incisors (and not in the apical region).
The present results showed maximum bone thickness in the anterior mandible compared with the site of canine and premolar teeth. However, Lim et al. [16] found that the most posterior area of the mandible had a higher bone thickness compared with the most anterior region, irrespective of depth, which was different from the present findings. This difference may be due to the fact that the most posterior area in the present study was the site of canine and first premolar while they assessed the posterior region of the mandible (last tooth in dental arch) and compared it with the anterior region. Park et al. [17] assessed the bone thickness based on the mesiodistal region and concluded that the mandibular bone thickness at the site of canine and premolar teeth was lower than the bone thickness in the mandibular symphysis and posterior region of the mandible. Although premolars were not evaluated in the present study, the premolar region is often a safe place for miniscrew placement considering the adequate interradicular space at the site of premolars.[13] However, the bone thickness was minimum at the site of canine and first premolar teeth in the present study.
Table 3. Comparison of males and females regarding the bone thickness (P values)
Table 4. Mean bone thickness (mm) at areas with a significant difference between males and females based on distance from the ridge crest
The present results also showed higher bone thickness in males at all areas with a significant difference with that in females.
Yagci et al. [18] confirmed the present results. In the present study, mandibular bone thickness at one site increased with age. Another study reported a direct correlation [19]
between age and bone thickness in some parts of the mandible. Although the present study found a significant correlation between age and bone thickness in only one region, a larger sample size would probably yield more significant correlations in other areas as well. Mallick et al. [19] reported a similar significant correlation in multiple areas.
Adequate sample size, and use of appropriate statistical tests were the strengths of this study. The present findings can aid in finding the most appropriate points for miniscrew insertion. Also, by detecting areas with low bone thickness, we may decide on the use of bone substitute prior to dental implant placement.
Small number of CBCT scans of young patients was a limitation of this study. Future studies should assess the effect of bone density on miniscrew insertion.
Conclusion
The results indicated that males generally had a higher bone thickness than females in the anterior mandible. Also, the bone thickness increased from the distal of canine towards the midline. Thickness also increased by an increase in depth, and maximum thickness was noted at 18 mm depth. Moreover, by an increase in age, the bone thickness significantly increased at 3 mm depth between the right canine and lateral incisor.
|





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
