Journal of Research in Dental
and Maxillofacial Sciences
Volume 8, Issue 4 (11-2023)
J Res Dent Maxillofac Sci 2023, 8(4): 280-285 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Parivar M, Rezaie A, Babapor Kheiroddin J. Effects of Emotional Self-Regulation Strategies and Regular Desensitization on Anxiety and Fear of Adult Dental Patients: A Clinical Trial. J Res Dent Maxillofac Sci 2023; 8 (4) :280-285
URL: http://jrdms.dentaliau.ac.ir/article-1-317-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-317-en.html



1- Department of Psychology, Faculty of Psychology, Tabriz branch, Islamic Azad University, Tabriz, Iran
2- Department of Psychology, Faculty of Psychology, Payame Noor University (PNU), Tehran, Iran ,Parivar90@yahoo.com
3- Department of Psychology, Faculty of Psychology, University of Tabriz, Tabriz, Iran
2- Department of Psychology, Faculty of Psychology, Payame Noor University (PNU), Tehran, Iran ,
3- Department of Psychology, Faculty of Psychology, University of Tabriz, Tabriz, Iran
Full-Text [PDF 316 kb]
(734 Downloads)
| Abstract (HTML) (2846 Views)
Introduction
Dental fear is a serious problem that has been extensively studied in the recent years [1-3]. It is often transmitted through social learning from friends and family members. Dental anxiety has long been recognized as a problem in children that can persist into adulthood and lead to avoidance of dental care [4]. This anxiety is typically a reaction to the unknown and can be triggered by encountering new experiences in a dental setting, such as observing a dental syringe and dental instruments, or smelling unpleasant odors [5]. Patients with high levels of dental fear and anxiety often experience significant behavioral and emotional problems [6]. The unfamiliar environment, combined with a lack of empathy from the dentist, can exacerbate these fears and lead to refusal of treatment. This, in turn, can result in severe anxiety, fear, and pain, which may manifest as aggressive behaviors [7-8].
Various methods have been explored to reduce negative emotions related to dental procedures, including mental imagery and behavioral-cognitive therapy [9,10]. Studies have shown that behavioral interventions can effectively reduce dental anxiety and increase treatment acceptance by both children and adults [1,3].
Emotional self-regulation is a crucial aspect of psychological health and well-being, involving both conscious and unconscious processes that allow individuals to manage their emotional responses [11,12]. This includes understanding and accepting negative emotions, actively changing their intensity or quality, and facing distressing situations with self-support [13]. Age and treatment factors, including pain, have been found to contribute to fear and anxiety related to dental procedures [14].
Regular desensitization is another approach which involves identifying responses that contradict fear through counterconditioning. The individuals are asked to exhibit these opposing responses in situations that elicit fear. Research has shown that individuals who undergo regular desensitization are better able to cope with anxious scenarios, and the benefits can transfer to real-life situations.
Peter and Weinstein proposed that caries removal by bur and anesthetic injection are among the most fear-inducing experiences, but regular desensitization can significantly reduce anxiety levels associated with these procedures[15].
Research suggests that dental fear and anxiety often develop during childhood, leading to a significant number of individuals in developing countries to avoid dental care, thus compromising their oral health [16,17]. Although anesthesia and medications can be used to alleviate pain and fear during dental procedures, these methods can be costly and may have side effects. As a result, behavioral-cognitive interventions have become increasingly important in reducing the negative behavioral outcomes associated with dental treatments.
Thus, this study aimed to compare the effectiveness of emotional self-regulation and regular desensitization techniques for reducing fear and anxiety of adult dental patients.
Materials and Methods
This clinical trial was conducted to evaluate the efficacy of two methods - emotional self-regulation and regular desensitization - in managing dental fear and anxiety. The study received ethical approval from the Ethics Committee of the Faculty of Dentistry at Islamic Azad University (IR.IAU.TABRIZ.REC.1401.044), and registered in the Iranian Registry of Clinical Trials (IRCT20220717055481N2).
The study population comprised of adults who had dental problems and were referred to Parivar Dentistry in 2019 (N=500). The sample consisted of 40 patients who reported experiencing fear and anxiety related to dental procedures. A purposeful sampling method was used to select the sample, and the selected patients were asked to complete a fear and anxiety questionnaire. Those with scores above the mean were chosen for the study. The
sample was then divided into two groups (n=20) of emotional self-regulation (group 1) and regular desensitization (group 2).
Two questionnaires were utilized in this study to assess dental fear and anxiety. The first questionnaire was the Dental Fear Scale, which addresses 19 different dental items that may elicit fear or anxiety in patients, such as seeing a dental syringe or hearing the sound of a dental drill. Patients were asked to rate their fear level for each item using a visual analog scale. A 10-cm line with specified grading was presented to the patient, with the left side indicating no fear at all and the right side indicating the highest level of fear. Patients marked their level of fear on the line, and values between 0 to 3 cm indicated less fear than average [18]. The fear level for each item was recorded as a number on the same scale, and the mean of all 19 obtained numbers was calculated for each participant to determine their overall level of dental fear. The reliability of this scale was confirmed in a previous study [19] and was further assessed in this study with a Cronbach alpha of 0.82. Content and face validity were also confirmed by the opinion of experts in psychology and education.
The Dental Anxiety Inventory (DAI) was developed by Stouthard et al. [20] in 1993 as a self-reporting tool to measure the anxiety related to dental procedures. The scale consists of 36 items and uses a five-point Likert scale ranging from strongly incorrect to strongly correct, with scores ranging from 1 to 5. The DAI is a one-factor scale and does not have any sub-scales. The highest possible score is 180, indicating the highest level of anxiety, while the lowest possible score is 36, indicating the lowest level of anxiety. The reliability of the DAI has been assessed by several studies. Stouthard et al. [20] reported an internal consistency of 0.96 to 0.98 using Cronbach alpha. Yousefi and Piri [21] found a reliability of 0.94 using both Cronbach alpha and test-retest methods. Our own analysis yielded a reliability of 0.88 using Cronbach alpha.
Overall, the DAI is a reliable tool for measuring dental anxiety and can be used in clinical and research settings to assess patient anxiety levels and monitor changes over time.
An introductory session was conducted for both groups to familiarize the participants with the program's objectives, methodology, and work process. The sessions for desensitization and emotional self-regulation were conducted in a group setting to facilitate social interactions and feedback among the participants. Each group received eight intervention sessions, with each session lasting 1.5 hours once a week for 2 months [22].
The comparison between the two experimental groups was made by t-test, while paired t-test was used to analyze the before and after results in each group.
Results
Full-Text: (990 Views)
| Abstract
Background and Aim: Dental anxiety and fear are prevalent among adult patients, necessitating behavioral interventions. This study aimed to assess the effectiveness of emotional self-regulation strategies and regular desensitization for alleviation of anxiety and fear of adult dental patients. Materials and Methods: This clinical trial study was conducted on 40 adult dental patients selected by purposeful sampling, who were divided into two groups. Group 1 (n=20) received emotional self-regulation strategies, and group 2 (n=20) underwent regular desensitization. Data were collected using the Dental Fear Survey and Dental Anxiety Inventory (DAI). Group 1 patients participated in 8 sessions of emotional self-regulation, each lasting 1.30 hours, while group 2 were engaged in an 8-session regular desensitization program of the same duration. Data analysis was performed using t-test and paired t-test. Results: Both emotional self-regulation strategies and regular desensitization significantly decreased the fear and anxiety of adult dental patients (P<0.01). Additionally, there was no statistically significant difference in the impact of emotional self-regulation strategies and regular desensitization on fear and anxiety of dental patients (P>0.05). Conclusion: Emotional self-regulation strategies and regular desensitization yield comparable effects on the anxiety and fear of adult dental patients. Key Words: Fear; Anxiety; Emotional Regulation; Desensitization, Psychologic; Dentistry |
Introduction
Dental fear is a serious problem that has been extensively studied in the recent years [1-3]. It is often transmitted through social learning from friends and family members. Dental anxiety has long been recognized as a problem in children that can persist into adulthood and lead to avoidance of dental care [4]. This anxiety is typically a reaction to the unknown and can be triggered by encountering new experiences in a dental setting, such as observing a dental syringe and dental instruments, or smelling unpleasant odors [5]. Patients with high levels of dental fear and anxiety often experience significant behavioral and emotional problems [6]. The unfamiliar environment, combined with a lack of empathy from the dentist, can exacerbate these fears and lead to refusal of treatment. This, in turn, can result in severe anxiety, fear, and pain, which may manifest as aggressive behaviors [7-8].
Various methods have been explored to reduce negative emotions related to dental procedures, including mental imagery and behavioral-cognitive therapy [9,10]. Studies have shown that behavioral interventions can effectively reduce dental anxiety and increase treatment acceptance by both children and adults [1,3].
Emotional self-regulation is a crucial aspect of psychological health and well-being, involving both conscious and unconscious processes that allow individuals to manage their emotional responses [11,12]. This includes understanding and accepting negative emotions, actively changing their intensity or quality, and facing distressing situations with self-support [13]. Age and treatment factors, including pain, have been found to contribute to fear and anxiety related to dental procedures [14].
Regular desensitization is another approach which involves identifying responses that contradict fear through counterconditioning. The individuals are asked to exhibit these opposing responses in situations that elicit fear. Research has shown that individuals who undergo regular desensitization are better able to cope with anxious scenarios, and the benefits can transfer to real-life situations.
Peter and Weinstein proposed that caries removal by bur and anesthetic injection are among the most fear-inducing experiences, but regular desensitization can significantly reduce anxiety levels associated with these procedures[15].
Research suggests that dental fear and anxiety often develop during childhood, leading to a significant number of individuals in developing countries to avoid dental care, thus compromising their oral health [16,17]. Although anesthesia and medications can be used to alleviate pain and fear during dental procedures, these methods can be costly and may have side effects. As a result, behavioral-cognitive interventions have become increasingly important in reducing the negative behavioral outcomes associated with dental treatments.
Thus, this study aimed to compare the effectiveness of emotional self-regulation and regular desensitization techniques for reducing fear and anxiety of adult dental patients.
Materials and Methods
This clinical trial was conducted to evaluate the efficacy of two methods - emotional self-regulation and regular desensitization - in managing dental fear and anxiety. The study received ethical approval from the Ethics Committee of the Faculty of Dentistry at Islamic Azad University (IR.IAU.TABRIZ.REC.1401.044), and registered in the Iranian Registry of Clinical Trials (IRCT20220717055481N2).
The study population comprised of adults who had dental problems and were referred to Parivar Dentistry in 2019 (N=500). The sample consisted of 40 patients who reported experiencing fear and anxiety related to dental procedures. A purposeful sampling method was used to select the sample, and the selected patients were asked to complete a fear and anxiety questionnaire. Those with scores above the mean were chosen for the study. The
sample was then divided into two groups (n=20) of emotional self-regulation (group 1) and regular desensitization (group 2).
Two questionnaires were utilized in this study to assess dental fear and anxiety. The first questionnaire was the Dental Fear Scale, which addresses 19 different dental items that may elicit fear or anxiety in patients, such as seeing a dental syringe or hearing the sound of a dental drill. Patients were asked to rate their fear level for each item using a visual analog scale. A 10-cm line with specified grading was presented to the patient, with the left side indicating no fear at all and the right side indicating the highest level of fear. Patients marked their level of fear on the line, and values between 0 to 3 cm indicated less fear than average [18]. The fear level for each item was recorded as a number on the same scale, and the mean of all 19 obtained numbers was calculated for each participant to determine their overall level of dental fear. The reliability of this scale was confirmed in a previous study [19] and was further assessed in this study with a Cronbach alpha of 0.82. Content and face validity were also confirmed by the opinion of experts in psychology and education.
The Dental Anxiety Inventory (DAI) was developed by Stouthard et al. [20] in 1993 as a self-reporting tool to measure the anxiety related to dental procedures. The scale consists of 36 items and uses a five-point Likert scale ranging from strongly incorrect to strongly correct, with scores ranging from 1 to 5. The DAI is a one-factor scale and does not have any sub-scales. The highest possible score is 180, indicating the highest level of anxiety, while the lowest possible score is 36, indicating the lowest level of anxiety. The reliability of the DAI has been assessed by several studies. Stouthard et al. [20] reported an internal consistency of 0.96 to 0.98 using Cronbach alpha. Yousefi and Piri [21] found a reliability of 0.94 using both Cronbach alpha and test-retest methods. Our own analysis yielded a reliability of 0.88 using Cronbach alpha.
Overall, the DAI is a reliable tool for measuring dental anxiety and can be used in clinical and research settings to assess patient anxiety levels and monitor changes over time.
An introductory session was conducted for both groups to familiarize the participants with the program's objectives, methodology, and work process. The sessions for desensitization and emotional self-regulation were conducted in a group setting to facilitate social interactions and feedback among the participants. Each group received eight intervention sessions, with each session lasting 1.5 hours once a week for 2 months [22].
The comparison between the two experimental groups was made by t-test, while paired t-test was used to analyze the before and after results in each group.
Results
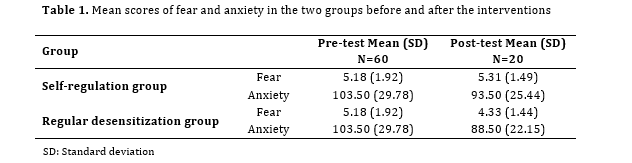
Descriptive results showed that 51.7% of the patients were females and 48.3% were males. The mean fear score of the sample in the pretest was 5.18 ±1.92, which decreased in the post-test of emotional self-regulation and desensitization groups to 5.31±1.49 and 4.33±1.44, respectively. Furthermore, the mean anxiety score of the sample was 103.50±29.78 in the pre-test, which decreased in the emotional self-regulation and desensitization groups to 93.50±25.48 and 88.50±22.15, respectively (Table 1).
The study found that there was a significant difference in fear and anxiety levels between the pre-test and post-test of the two groups (P<0.05). Emotional self-regulation strategies had a significant impact on reducing fear and anxiety of dental patients, with the highest impact seen on anxiety. Desensitization also had a significant impact on fear and anxiety reduction of patients. Specifically, emotional self-regulation strategies caused 24% and 61% reduction in fear and anxiety, respectively; while desensitization caused 47% and 52% reduction in fear and anxiety, respectively.
Independent t-test indicated that there was no significant difference between theeffectiveness of emotional self-regulation strategies and desensitization in dental patients (P>0.05).
Table 1. Mean scores of fear and anxiety in the two groups before and after the interventions
Discussion
The study found that there was a significant difference in fear and anxiety levels between the pre-test and post-test of the two groups (P<0.05). Emotional self-regulation strategies had a significant impact on reducing fear and anxiety of dental patients, with the highest impact seen on anxiety. Desensitization also had a significant impact on fear and anxiety reduction of patients. Specifically, emotional self-regulation strategies caused 24% and 61% reduction in fear and anxiety, respectively; while desensitization caused 47% and 52% reduction in fear and anxiety, respectively.
Independent t-test indicated that there was no significant difference between theeffectiveness of emotional self-regulation strategies and desensitization in dental patients (P>0.05).
Table 1. Mean scores of fear and anxiety in the two groups before and after the interventions
{kind=link}
Discussion
The present study compared the effectiveness of two instructional methods, emotional self-regulation, and regular desensitization, for reducing dental fear and anxiety of adult dental patients.
The results indicated that instruction of emotional self-regulation strategies was effective in reducing fear and anxiety, which was consistent with the results of previous studies by Gross [23], Campbell-Sills and Barlow [24], Claesson et al. [25] Daubenmier et al. [26], and Kuntz [27]. Salovey and Mayer [28] suggested that regulating emotions leads to conscious growth, the ability to control emotions appropriately, and the ability to convert negative emotions into positive ones. Additionally, Boyatzis et al. [29] suggested that regulating emotions increases self-awareness, helps individuals control themselves better, and reduces fear and anxiety. By harmonizing biological and motivational processes, regulating emotions can help individuals adapt to their environment, cope with anxieties and fears, and experience greater mental balance. Overall, these findings suggest that emotional self-regulation may be an effective strategy for reducing fear and anxiety in dental patients.
The present study found that regular desensitization was effective in reducing fear and anxiety of adult dental patients by addressing both cognitive and physiological aspects. This finding is consistent with previous studies that showed that desensitization can lead to a reduction in avoidance behavior and an increase in compliance with dental treatment [30,31].
This is achieved by teaching individuals to visualize anxiogenic scenes while simultaneously practicing muscle relaxation techniques in a therapeutic setting. The new responses to conditioned anxiogenic stimuli are then transferred to real-life stressful situations through generalization. Muscle relaxation helps to reduce tension, pain, panic, distress, paleness, tremble, heart rate, hypertension, and heart contractions, resulting in a decreased level of fear and anxiety in individuals with dental fear. Additionally, virtual reality desensitization was found to be equally effective in reducing fear and anxiety by allowing individuals to experience simulated dental procedures in a controlled environment, which can help them develop coping mechanisms and reduce their fear of real-life dental procedures.
The present study found that emotional self-regulation strategies and regular desensitization had a comparable impact on reducing fear and anxiety in individuals seeking dental treatment. Regular desensitization has the added benefit of addressing both cognitive and physiological aspects of fear and anxiety, leading to long-term improvements in dental health outcomes and quality of life. Patients undergoing emotional self-regulation may have greater awareness and agency over their treatment, potentially leading to quicker reductions in fear and anxiety. Overall, both strategies can be valuabletools for dental professionals to improve patient experiences and outcomes.
One of the main limitations of the present study was that the sample was selected by purposeful sampling method. As a result, it is important to exercise caution when generalizing the findings. Dentists should prioritize spending more time calming patients and building trust by being aware of the parameters that aggravate the fear and anxiety of dental patients. Future studies are required on different populations to obtain a more comprehensive understanding of societal realities.
Conclusion
In this study, both emotional self-regulation strategies and regular desensitization techniques were found to be equally effective in significantly reducing the anxiety and fear of adult dental patients. This study demonstrated that both approaches may offer viable options for improving the overall dental experience of adult dental patients.
The results indicated that instruction of emotional self-regulation strategies was effective in reducing fear and anxiety, which was consistent with the results of previous studies by Gross [23], Campbell-Sills and Barlow [24], Claesson et al. [25] Daubenmier et al. [26], and Kuntz [27]. Salovey and Mayer [28] suggested that regulating emotions leads to conscious growth, the ability to control emotions appropriately, and the ability to convert negative emotions into positive ones. Additionally, Boyatzis et al. [29] suggested that regulating emotions increases self-awareness, helps individuals control themselves better, and reduces fear and anxiety. By harmonizing biological and motivational processes, regulating emotions can help individuals adapt to their environment, cope with anxieties and fears, and experience greater mental balance. Overall, these findings suggest that emotional self-regulation may be an effective strategy for reducing fear and anxiety in dental patients.
The present study found that regular desensitization was effective in reducing fear and anxiety of adult dental patients by addressing both cognitive and physiological aspects. This finding is consistent with previous studies that showed that desensitization can lead to a reduction in avoidance behavior and an increase in compliance with dental treatment [30,31].
This is achieved by teaching individuals to visualize anxiogenic scenes while simultaneously practicing muscle relaxation techniques in a therapeutic setting. The new responses to conditioned anxiogenic stimuli are then transferred to real-life stressful situations through generalization. Muscle relaxation helps to reduce tension, pain, panic, distress, paleness, tremble, heart rate, hypertension, and heart contractions, resulting in a decreased level of fear and anxiety in individuals with dental fear. Additionally, virtual reality desensitization was found to be equally effective in reducing fear and anxiety by allowing individuals to experience simulated dental procedures in a controlled environment, which can help them develop coping mechanisms and reduce their fear of real-life dental procedures.
The present study found that emotional self-regulation strategies and regular desensitization had a comparable impact on reducing fear and anxiety in individuals seeking dental treatment. Regular desensitization has the added benefit of addressing both cognitive and physiological aspects of fear and anxiety, leading to long-term improvements in dental health outcomes and quality of life. Patients undergoing emotional self-regulation may have greater awareness and agency over their treatment, potentially leading to quicker reductions in fear and anxiety. Overall, both strategies can be valuabletools for dental professionals to improve patient experiences and outcomes.
One of the main limitations of the present study was that the sample was selected by purposeful sampling method. As a result, it is important to exercise caution when generalizing the findings. Dentists should prioritize spending more time calming patients and building trust by being aware of the parameters that aggravate the fear and anxiety of dental patients. Future studies are required on different populations to obtain a more comprehensive understanding of societal realities.
Conclusion
In this study, both emotional self-regulation strategies and regular desensitization techniques were found to be equally effective in significantly reducing the anxiety and fear of adult dental patients. This study demonstrated that both approaches may offer viable options for improving the overall dental experience of adult dental patients.
Type of Study: Original article |
Subject:
Dental implant
References
1. Heaton LJ. Behavioral interventions may reduce dental anxie-ty and increase acceptance of dental treatment in dentally fearful adults. J Evid Based Dent Pract. 2013 Dec; 13 (4):160-2. [DOI:10.1016/j.jebdp.2013.10.008] [PMID] []
2. Neacsu V, Sfeatcu IR, Maru N, Dumitrache MA. Relaxation and Systematic Desensitization in Reducing Dental Anxiety. Procedia - Social and Behavioral Sciences. 2014; 127(22): 474-8. [DOI:10.1016/j.sbspro.2014.03.293]
3. Nilsson S, Renning AC. Pain management during wound dress-ing in children. Nurs Stand. 2012 Apr 11-17;26(32):50-5. [DOI:10.7748/ns.26.32.50.s50] [PMID]
4. Fallah M, Basharpoor S, Bagheri A. Comparing the Effectiveness of Systematic Desensitization and Distraction on Pain and Fear in Children with Dental Problems. J Ardabil Univ Med Sci. 2016; 16 (1) :74-84.
5. Bracha HS, Vega EM, Vega CB. Posttraumatic dental-care anxi-ety (PTDA): Is "dental phobia" a misnomer? Hawaii Dent J. 2006 Sep-Oct;37(5):17-9.
6. Klingberg G, Berggren U, Carlsson SG, Noren JG. Child dental fear: cause-related factors and clinical effects. Eur J Oral Sci. 1995 Dec;103(6):405-12. [DOI:10.1111/j.1600-0722.1995.tb01865.x] [PMID]
7. Appukuttan DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. Clin Cosmet Inves-tig Dent. 2016 Mar 10;8:35-50. [DOI:10.2147/CCIDE.S63626] [PMID] []
8. Trowbridge HO. Review of dental pain--histology and physiology. J Endod. 1986 Oct;12(10):445-52. [DOI:10.1016/S0099-2399(86)80197-2] [PMID]
9. Maier A, Schaitz C, Kröner J, Connemann B, Sosic-Vasic Z. Im-agery Rescripting: Exploratory Evaluation of a Short Intervention to Reduce Test Anxiety in University Students. Front Psychiatry. 2020 Feb 28;11:84. [DOI:10.3389/fpsyt.2020.00084] [PMID] []
10. P BJ. Dental subscale of children's fear survey schedule and dental caries prevalence. Eur J Dent. 2013 Apr;7(2):181-5. [DOI:10.4103/1305-7456.110166] [PMID] []
11. Nolen-HoeKsema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Psychol Sci. 2008 Sep;3(5):400-24. [DOI:10.1111/j.1745-6924.2008.00088.x] [PMID]
12. Eftekhari A, Zoellner LA, Vigil SA. Patterns of emotion regula-tion and psychopathology. Anxiety Stress Coping. 2009 Oct;22(5):571-86. [DOI:10.1080/10615800802179860] [PMID] []
13. Hughes EK, Gullone E. Emotion regulation moderates rela-tionships between body image concerns and psychological symptomatology. Body Image. 2011 Jun ;8(3): 224-31. [DOI:10.1016/j.bodyim.2011.04.001] [PMID]
14. Majstorovic M, Veerkamp JS. Relationship between needle phobia and dental anxiety. J Dent Child (Chic). 2004 Sep-Dec;71(3):201-5.
15. Peter K, Weinstein P. Results of a dental fear survey in Japan: Implication for dental public health in Asia. Dent Oral Epidemiol. 2017;16(4):199-207. [DOI:10.1111/j.1600-0528.1988.tb01753.x] [PMID]
16. Morowatisharifabad M, Razavinia M, Haerian-Ardakani A, Fallahzadeh H. Study of Dental Anxiety among Patients Referred to Private Offices in Mashhad. TB 2012; 11(2): 119-30.
17. Melnick, J, Russell R, W. Hypnosis versus systematic desen-sitization in the treatment of test anxiety. Journal of Counseling Psychology;23(4):291-5. [DOI:10.1037/0022-0167.23.4.291]
18. Tabrizizadeh M, Agham Alizadeh F. Assessment of the rate of fear in different dental situations in Yazd Dental School. Journal of Dental School, Shahid Beheshti University of Medical Sciences. 2003; 21(4): 464-73.
19. Shojaeipour R, Behrouzpour K. Assessment of the rate of fear in different dental processes in Kerman dental school, 2007. Journal of Dental School, Shahid Beheshti University of Medical Sciences. 2008;26(2):163-70.
20. Stouthard ME, Mellenbergh GJ, Hoogstraten J. Assessment of dental anxiety: A facet approach. Anxiety, Stress & Coping: An International Journal. 1993;6(2):89-105. [DOI:10.1080/10615809308248372]
21. Yousefi R, Piri F. Psychometric Properties of Dental Anxiety Inventory. Journal of Mashhad Dental School. 2017; 41(1):69-78.
22. Parivar M, Rezaei A, Babapour Kheiroddin J. Effect of Emotional Self-Regulation Strategies and Systematic Desensitization on Stress Level of Adult Dental Patients: A Clinical Trial. J Res Dent Maxillofac Sci. 2023; 8(1):43-48. [DOI:10.52547/jrdms.8.1.43]
23. Gross JJ. The Emerging Field of Emotion Regulation: An Inte-grative Review. Review of General Psychology.1998 2(3), 271-99. [DOI:10.1037/1089-2680.2.3.271]
24. Campbell-Sills L, Barlow DH. Incorporating Emotion Regula-tion into Conceptualization and Treatment of Anxiety and Mood Disorders. In: Gress JJ, editor. Handbook of emotion regulation. New York: Guilford Press; 2007. p. 542-559.
25. Claesson M, Birgander LS, Lindahl B, Nasic S, Aström M, Asplund K, Burell G. Women's hearts--stress management for women with ischemic heart disease: explanatory analyses of a randomized controlled trial. J Cardiopulm Rehabil. 2005 Mar-Apr;25(2):93-102. [DOI:10.1097/00008483-200503000-00009] [PMID]
26. Daubenmier JJ, Weidner G, Sumner MD, Mendell N, Merritt-Worden T, Studley J, Ornish D. The contribution of changes in diet, exercise, and stress management to changes in coronary risk in women and men in the multisite cardiac life-style intervention program. Ann Behav Med. 2007 Feb; 33(1):57-68. [DOI:10.1207/s15324796abm3301_7] [PMID]
27. Kuntz KK. Social support and quality of life in women with congestive heart failure [dissertation]. United States: Ohio State University; 2006. 110 p.
28. Salovey P, Mayer JD. Emotional Intelligence. Imagination, Cognition and Personality. 1990;9(3):185-211. [DOI:10.2190/DUGG-P24E-52WK-6CDG]
29. Boyatzis R, Goleman D, Rhee K. Clustering competence in emotional intelligence: insights from the emotional competence inventory (ECI). In: Bar-On R, editor. Handbook of emotional intelligence. San Francisco: Jossey-Bass; 2000. P. 343-62.
30. Kaazemian Moghadam K, Mehrabizadeh Honarmand M, Soodani M. The impact of systematic desensitization on test anxiety and school performance among female Behbahaani jun-ior high school students. The Journal of New Thoughts on Edu-cation. 2008; 4(3): 55-78.
31. Harris MM. Meta-analyses of test anxiety among college students. US: ProQuest Information & Learning; 1988.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |