
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-291-en.html



2- Assistant Professor, Oral and Maxillofacial Pathology Dept, Dental Research Center, Mazandaran University of Medical Sciences, Sari, Iran ,
3- Dentist
Abstract
Background and Aim: Pregnancy refers to a physiological process associated with body changes, including changes in the oral cavity. Therefore, dental treatments are an integral part of healthcare for pregnant women. The purpose of this study was to evaluate the knowledge and practice of dentists in Bandar Abbas, Iran, regarding the required measures during pregnancy in 2018.
Materials and Methods: The present descriptive cross-sectional study was conducted on 93 dentists in Bandar Abbas by completing a twenty-item questionnaire about the required measures during pregnancy. Data were analyzed using SPSS16. Chi-square test and t-test were used to statistically analyze the data at the significance level of 0.05.
Results: The mean score of dentists' knowledge index was 43.86±8.66 (moderate). The level of knowledge was moderate for 59 dentists (63.4%), and only one had a low level of knowledge. In addition, 39 dentists (41.9%) had low, 49 (52.7%) had moderate, and only 5 (5.4%) had a high practice score. None of the demographic factors had a significant relationship with dentists' knowledge.
Conclusion: Workshops and continuous educational programs are recommended to increase the knowledge of dentists regarding the required measures during pregnancy.
Keywords: Dentist, Knowledge, Oral Health, Pregnancy
Introduction
Pregnancy is a physiological process associated with body changes, including changes in the oral cavity. During this period, the oral environment is more susceptible to caries because of morning sickness and vomiting, resulting in acidification of the mouth, increased tendency to consume sweets, and less attention to oral hygiene. (1,2)
Oral changes during pregnancy occur primarily in the periodontium and are linked to factors such as nutritional deficiencies, high levels of hormones, like estrogen and progesterone, and the presence of dental plaque. Gingivitis is common in this period and occurs in 30% to 100% of pregnant women. Elevated progesterone levels during pregnancy cause conditions for gingivitis. (3-5)
There are also changes in saliva and oral flora, increasing the acidity of the mouth and promoting bacterial growth.
Despite this evidence, many dentists are reluctant to care for pregnant women due to the lack of preparation and knowledge required, which can worsen patients’ oral condition and harm both mother and baby. This reluctance is in part attributed to gaps in the training of undergraduate dentists.
Some studies have been conducted in this field, and different results have been reported.
The mean awareness score of dentists in Mashhad was moderate with no difference between men and women. (6) The mean knowledge score of dentists was 62% in Isfahan, which indicates an appropriate and acceptable level of knowledge. (2) This rate was 51.84% in a study conducted by Molania et al in Sari. (1)
Considering the importance of maintaining good oral health in pregnant women and due to the lack of studies on the knowledge of Iranian dentists in this regard, the present study aimed to evaluate the knowledge and practice of general dentists in the city of Bandar Abbas regarding the required measures during pregnancy.
Materials and Methods
The current descriptive cross-sectional study (ethical approval code: IR.HUMS.REC.1397.099, Hormozgan University of Medical Sciences) was conducted on general dentists working in the city of Bandar Abbas in 2018. Of the 125 general dentists, 32 were excluded because of failure to cooperate with the project, and 93 dentists were recruited.
We used the questionnaire that Salehi et al adopted to evaluate the knowledge and practice of dentists about the necessary measures during pregnancy in the city of Isfahan (with confirmed validity and reliability). (2) The questionnaire contains 20 questions in two parts. The first part (14 questions) deals with the dentists' knowledge on the necessary measures during pregnancy, and the second part (6 questions) deals with the dentists' practice on pregnant women. (2)
The dentists' knowledge evaluation part contains 14 questions, each of which yielding a score of 5 if it is answered correctly and zero if the answer is incorrect. A score of 5 is calculated for questions with more than one correct answer. Therefore, the minimum score for the knowledge index is zero, and the maximum score is 70, indicating a score of ≤23 as a low level of knowledge, a score between 24 and 47 as a moderate level of knowledge, and a score ≥48 as a high level of knowledge.
The dentists' practice evaluation part contains 6 questions, each of which yielding a score of 5 if it is answered correctly and zero if the answer is incorrect. A score of 5 is calculated for questions with more than one correct answer. Therefore, the minimum score for the practice index is zero, and the maximum score is 30, indicating a score of ≤10 as a low level of practice, a score between 11 and 20 as a moderate level of practice, and a score ≥21 as a high level of practice.
The data were analyzed using SPSS (Version 16, SPSS Inc., Chicago, IL, USA). The indices of central tendency, such as mean, as well as dispersion indices, such as standard deviation (SD), were applied to describe the data. Chi-square test and t-test were used to statistically analyze the data. The significance level was considered 0.05.
Results
Of the 93 general dentists participating in the current study, 48 were male (51.6%) and 45 were female (48.4%).
The mean age of the participants was 33.05±7.28 years (ranging from 23 to 57 years). The majority of the subjects were in the age group lower than 30 years (41.9%), and few subjects were over the age of 50 years (4.3%).
The mean dental experience of dentists was 8.35±6.27 years (ranging from 6 months to 25 years).
Moreover, 84 dentists (90.3%) had a history of participating in relevant retraining classes, and only 9 (9.7%) had no history of taking part in retraining classes.
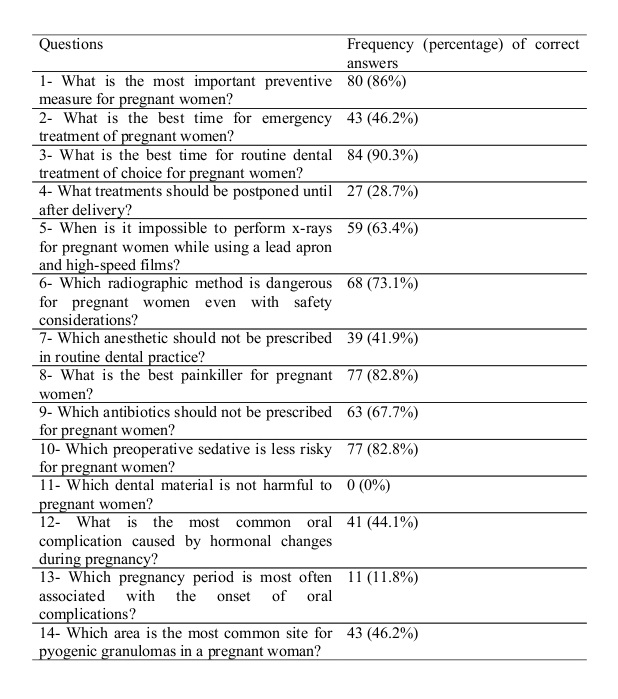
Table 1 shows the frequency of correct answers given by dentists in the city of Bandar Abbas to questions about knowledge of the necessary measures during pregnancy.
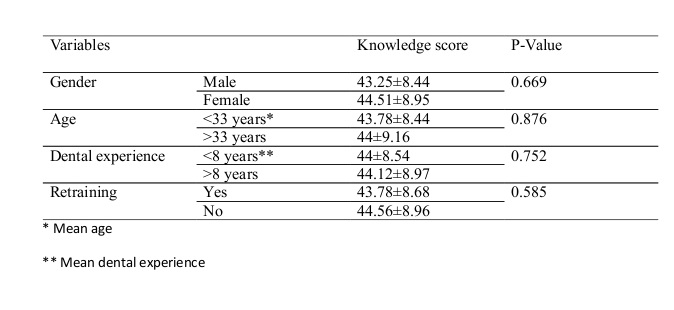
Table 2 shows the relationship between demographic factors and the knowledge level of dentists. The results of the statistical tests showed that none of the demographic factors had a significant relationship with dentists' knowledge (P>0.05).
Table 1. Frequency distribution and percentage of correct answers given by dentists in the city of Bandar Abbas to questions about knowledge of the required measures during pregnancy
Table 2. Relationship between demographic profiles of dentists in the city of Bandar Abbas and their knowledge about the required measures during pregnancy
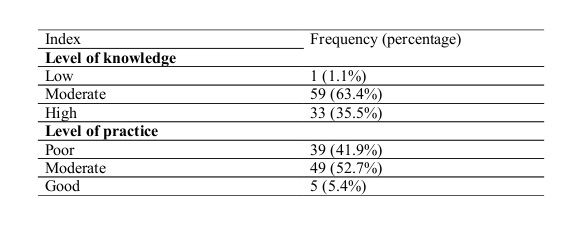
The mean knowledge score of dentists in the city of Bandar Abbas was 43.86±8.66, which varied from at least 22 points to a maximum of 63 points. Only one dentist (1.1%) had a low level of knowledge. In addition, 59 dentists (63.4%) had a moderate level of knowledge, and only 33 (35.5%) had a high level of knowledge.
The mean practice score for dentists in the city of Bandar Abbas was 14.31±5.5, ranging from at least 5 points to a maximum of 30 points. Table 3 shows the level of knowledge and practice of dentists in the city of Bandar Abbas.
Table 3. Evaluation of the knowledge and practice of dentists in the city of Bandar Abbas about the required measures during pregnancy
Discussion
{kind=link}
{kind=link}
{kind=link}
The present study evaluated the knowledge and practice of 93 dentists in Bandar Abbas. The mean knowledge score of the dentists was 43.86±8.66 (moderate). In Mashhad, Mossanan Mozafari et al reported an average knowledge score of dentists similar to ours. (6) The mean knowledge score reported by Salehi et al was 62% in Isfahan, which indicated an appropriate and acceptable level of knowledge for the dentists. (2) This rate was 51.84% in the study conducted by Molania et al in Sari. (1) Mehdipoor et al, in 2017, evaluated the knowledge of dentists and gynecologists regarding oral care during pregnancy in Qom. (7) Based on their results, dentists (higher scores) and gynecologists gained satisfactory mean knowledge, attitude, and practice scores. (7)
In a study conducted by George et al in Australia, the majority of the dentists (99%) stated that pregnant women should receive a dental check. (8) The dentists were aware of safe dental practices during pregnancy but they had limited knowledge of the relationship between periodontal disease and adverse pregnancy outcome. (8) Similar results were seen among dentists in North Carolina, Florida, and Oregon in the United States, where nearly 40% of the dentists were unsure of the oral-systemic association during pregnancy. (9,10)
In the present study, there was no statistically significant difference between the knowledge levels of men and women, which is similar to the result reported by Mossanan Mozafari et al in Mashhad, where there was no correlation between the level of knowledge and gender. (6) However, in studies conducted by Salehi et al in Isfahan and Molania et al in Sari, women had higher knowledge scores. (1,2)
In the present study, the age and the experience of the dentists showed no significant correlation with their knowledge. On the contrary, in the study by Molania et al, dentists' knowledge decreased with age and work experience. (1) In the study by Mossanan Mozafari et al, age and work experience showed no significant correlation with knowledge, which was stated as a possible reason for the effectiveness of continuing education programs in promoting knowledge. (6) In 2015, in a review of the last 10 years' publications, Vieira et al concluded that dentists are doubtful about the care of pregnant women, especially with x-rays, prescriptions, and the best gestational period for treatment. (11,12) Their outcomes advocate the necessity of improving dentists’ knowledge regarding dental care of pregnant women because they may develop new habits that might affect the oral health of their children. (11)
In the present study, the highest number of correct answers given by the dentists was about the best time for treatment of pregnant women. Routine dental procedures are recommended in the second trimester; most of the participants responded correctly to this question. In the study conducted by Salehi et al, 81.9% of the participants answered this question correctly, indicating that dentists are aware of the proper treatment. (2) However, in case of emergencies, we are allowed to perform dental treatment throughout pregnancy; 43% of the dentists responded to this question correctly.
Plaque control is also one of the most important preventive measures that guarantee oral health during pregnancy. In this study, dentists showed a good level of knowledge of the most important preventive measures for pregnant women; 86% of the dentists chose “plaque control” as the correct option. In the study by Salehi et al, 78.2% of the participants answered this question correctly. (2)
The very high rate of incorrect responses to the question regarding dental materials was very noticeable in the current study. None of the materials used in dentistry cause complications for pregnant women. None of the dentists participating in this study gave the correct answer (no dental material is harmful). The highest incorrect response rate was related to glass ionomer followed by amalgam and impression-taking materials, which were harmful to pregnant women from the dentists’ viewpoints. In the study by Salehi et al, 49% of the dentists answered this question correctly. (2) Since none of the dentists answered this question correctly in the present study, there is a need for knowledge gain regarding the use of restorative materials when treating pregnant women.
Conclusion
Dentists in Bandar Abbas showed a moderate level of knowledge and practice regarding the management of pregnant women. Workshops and continuous educational programs are recommended to increase the knowledge of dentists regarding the required measures during pregnancy.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |