

Volume 7, Issue 4 (10-2022)
J Res Dent Maxillofac Sci 2022, 7(4): 226-232 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salimzade S, Sadat Mansouri S, Etemadi A. Effect of Platelet-Rich Fibrin Application on the Maxillary Sinus Schneiderian Membrane Thickness Following Sinus Floor Augmentation: A Clinical Trial. J Res Dent Maxillofac Sci 2022; 7 (4) :226-232
URL: http://jrdms.dentaliau.ac.ir/article-1-290-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-290-en.html



1- Department of Periodontology, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran , dr.ssalimzade@gmail.com
2- Department of Periodontology, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
2- Department of Periodontology, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
Full-Text [PDF 753 kb]
(928 Downloads)
| Abstract (HTML) (1865 Views)
Introduction
Reconstruction of an edentulous posterior maxilla by dental implants has always been a challenge due to the presence of low-density bone and sinus pneumatization [1-3]. In case of no augmentation, progressive bone loss continues, and treatment with implant-supported restorations will be problematic and associated with high risk of failure [3,4]. Several techniques have been proposed to augment bone with optimal quality and quantity for implant placement; among which, sinus floor augmentation is a more predictable method, which was first performed by Boyne and James [4]. It is still commonly performed due to its high success rate. In sinus floor augmentation procedures, the sinus membrane status and preserving its integrity are highly important. High variations have been reported in sinus membrane thickness [5]. Makary et al. [6] reported a significant increase in sinus membrane thickness after sinus floor augmentation by the lateral approach. This increase in thickness may be due to a physiological inflammatory reaction to surgical trauma, including bleeding and inflammation in primary phases of healing [6]. Although reaction of nasal and paranasal mucosa to different factors such as infection, allergy, and surgical trauma has been well documented, sinus membrane response to sinus floor elevation by the lateral approach has been less commonly assessed [6].
Watelet et al. [7] clearly described the wound healing process in nasal and paranasal mucosa. They divided this process into four overlapping phases of inflammation, cell proliferation, matrix deposition, and tissue remodeling. Healing phases in sinus floor augmentation including the lateral window approach have also been described [7].
Platelet products were first used for prevention and treatment of hemorrhage due to severe thrombocytopenia. Standard platelet concentrate was first referred to as platelet-rich plasma (PRP), which classically included 0.5 x 1011 platelets per each unit. Platelet products are used to enhance bone regeneration by release of growth factors. Platelets contain a high volume of key growth factors such as platelet-derived growth factors, B1 and B2 transforming growth factors, and vascular endothelial growth factor that can induce and enhance cell proliferation and angiogenesis. To date, several techniques for the use of autologous platelet concentrates have been developed [8].
Considering the role of PRF in enhancement of healing by release of growth factors, this study aimed to assess the effect of PRF as a protective barrier beneath the sinus membrane on the Schneiderian membrane thickness following sinus floor augmentation surgery.
Materials and Methods
In this randomized controlled split-mouth clinical trial, cone-beam computed tomography (CBCT) scans were used to assess the Schneiderian membrane thickness at the deepest point of the maxillary sinus. Eighteen patients (36 maxillary sinuses) who required bilateral sinus floor augmentation due to sinus pneumatization and bone resorption according to clinical and radiographic examinations were selected. The inclusion criteria were residual crestal bone thickness between the sinus floor and bone crest to be maximally 3 mm and O’Leary’s plaque index < 20%. The exclusion criteria were acute sinus infection, chronic sinusitis, allergy, cigarette smoking, treatment with bisphosphonates, uncontrolled diabetes mellitus, and pregnancy. Two patients (4 sinuses) were excluded due to chronic sinusitis, and one patient was excluded due to perioperative sinus membrane perforation. Finally, 15 patients (30 sinuses) were studied, and underwent CBCT. The study was approved by the ethics committee of the university (IR.IAU.DENTAL.REC.1397.051) and registered in the Iranian Registry of Clinical Trials IRCT22710201972016).
After phase I periodontal therapy (if required) and oral hygiene instruction, the O’Leary’s plaque index of patients was calculated to ensure it is below 20%. Next, the patients were asked to rinse their mouth with 0.2% chlorhexidine gluconate (Iran Behdasht, Iran) for 30 seconds prior to the surgical procedure. Local anesthesia was induced with 2% lidocaine plus 1:100,000 epinephrine (Darupakhsh, Iran). A crestal incision was made along with two vertical releasing incision at the mesial and distal to elevate a full-thickness flap and expose the buccal (lateral) wall of the maxillary sinus. The lateral window was opened by using the Dask kit (Dentium, Seoul, South Korea). The sinus membrane was elevated and a PRF membrane was placed beneath the Schneiderian membrane at the test side. PRF membrane was not used for the control side. Allocation of each side to the test or control group in each patient was performed randomly by flipping a dice. As mentioned earlier, sinus membrane perforation occurred during retraction of tissue in one patient, and this patient was excluded from the study.
PRF was prepared as follows: right before the surgical procedure, 9 mL of venous blood was obtained from the patients according to the Choukroun protocol [9], and collected in dry capped glass or plastic tubes coated with anticoagulant agent, and centrifuged in L-PRF centrifuge machine (Intra-Lock; Intrapsin, USA). Centrifugation resulted in formation of three layers: a red blood cell layer at the bottom, a cell-free plasma layer on the top, and PRF clot in the middle. PRF layer was collected by sterile hemostat and was cut from the red blood cell layer by scissors. Sinus floor augmentation was then performed using 1000-2000 μm xenograft granules (Cerabone, Botiss, Germany). A xenograft membrane (Jason, Botiss, Germany) was placed over the lateral window, the flap was returned, and sutured with 4-0 silk sutures (Surgical Silk; Supa, Iran).
Postoperative instructions:
All patients were prescribed 400 mg ibuprofen (Arya, Iran) every 6 hours for 1 week. Co-amoxiclav (625 mg; Farabi, Iran) was prescribed prophylactically to be taken daily for 7 to 10 days. Allergic patients were prescribed 600 mg clindamycin instead. Also, the patients were instructed to rinse 0.2% chlorhexidine mouthwash (Iran Behdasht, Iran) for 15 days after surgery. The sutures were removed after 7 days, and the patients were clinically and radiographically examined at 1 week and 2 months, postoperatively, and underwent CBCT of the surgical site.
Imaging:
CBCT scans were taken using 3D Mid Planmeca CBCT scanner (Finland) with 0.2 mm voxel size, 8 mA amperage, and 90 kV voltage with 12.05 s exposure time. All CBCT images were obtained with 4 x 4, 6 x 6, and 8 x 8 cm fields of view. Images were reconstructed with 0.5 mm slice intervals.
Image assessment:
CBCT images were assessed by an experienced radiologist who was not directly involved in the process of treatment and follow-up of patients. To ensure optimal calibration and intra-examiner reliability, each measurement was repeated, and the mean value was calculated; when the difference between the two measurements was 0.2 mm or higher, measurement was repeated for the third time. CBCT images were analyzed on a 22-inch monitor (Samsung; Korea) with 1024 x 1224-pixel resolution. Measurements were made using Planmeca Romexis version 5.1.0 software.
Measuring the Schneiderian membrane thickness:
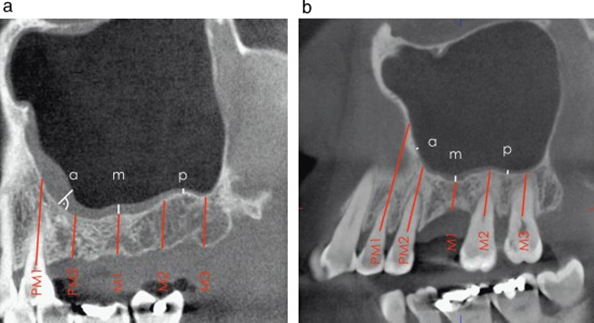
CBCT sections were reformatted such that the posterior segment of the maxilla (from the first premolar to the second molar) on axial sections was oriented vertically while the floor of the nose and palate on coronal sections was oriented horizontally. Next, three standard measurements were made from the Schneiderian membrane dimensions in millimeters using coronal CBCT sections of the anterior part of the maxillary sinus in lateral (alat) dimension followed by mid-sagittal (amid) and medial (amed) dimensions. The selected anterior section from the maxillary sinus floor matched the area between the apices of maxillary premolars in a dentate patient (Figure 1).
Figure 1. Measurements made on sagittal CBCT sections: (a) anterior section (PM1: first premolar, PM2: second premolar), (m) middle section (M1: first molar), and (p) posterior section (M2: second molar, M3: third molar).
(a)Patient with free-end maxillary edentulous ridge; (b) patient with single tooth loss in the left posterior maxilla.
The following anatomical landmarks were measured on coronal CBCT sections for standard measurements (Figure 2a-c):
(I) Initiation point of the zygomatic process for lateral measurements (alat)
(II)Deepest point of the sinus floor on coronal CBCT sections for mid-sagittal measurement (amid)
(III)Skeletal floor of the nasal cavity of the same side for medial measurement (amed)
In cases where the sinus floor had a higher (more cranial) position relative to the zygomatic process or skeletal floor of the nasal cavity, the lateral (lat) and medial (med)
measurements were made at the level of initiation of inferior nasal concha of the same side. The three measurements were repeated in the middle part (Figure 1, m) corresponding to the maxillary first molar apex (mmed, mmid, mlat) and in the posterior region corresponding to the area between the apices of maxillary second and third molars in a dentate patient (pmed, pmid, and plat). In the edentulous posterior regions, the distance between the premolar roots was adjusted to be 7 mm, and the distance between the molar roots was adjusted to be 8 mm. Thus, radiographic assessments included 9 separate measurements for each maxillary sinus (Figure 3, 4) [8]. All measurements related to the mucosal thickness were performed perpendicular to the underlying bone (initiating from the underlying bone plate and terminating at the mucosal surface).
Statistical analysis:
The two groups were compared regarding the Schneiderian membrane thickness by paired t-test.
Figure 2. Anatomical landmarks for measurement of mucosal thickness on coronal CBCT sections in the anterior (a), middle (b) and posterior (c) areas.
Initiation point of zygomatic process for lateral
measurements (lat), deepest point of the sinus floor on coronal CBCT sections for mid-sagittal
measurement (mid), skeletal floor of the nasal cavity of the same side for medial measurement (med).
Dotted red line indicates the position of skeletal floor of the nasal cavity. Continuous red line indicates the inferior nasal concha
Figure 3. L-PRF clot was removed from the tube
Figure 4. Weight of the cap resulted in formation of a membrane from the L-PRF clot
Results
The Schneiderian membrane thickness was measured and compared in patients undergoing sinus floor augmentation with and without PRF membrane in a split-mouth design before and at 1 week and 2 months after surgery. A total of 15 patients including 8 females and 7 males between 42 to 68 years (mean age of 53.6± 0.18 years) were evaluated (30 sinuses). All patients were followed-up for 2 months, and surgical procedures of each patient were performed within one session. In the test side, L-PRF membrane was used beneath the Schneiderian membrane while the other side served as the control side and did not receive L-PRF membrane.
Table 1 presents the mean thickness of the Schneiderian membrane in 30 sinuses in
15 patients at the three time points in millimeters. The minimum and maximum thickness of the Schneiderian membrane preoperatively was 0.73 mm and 3.08 mm, respectively.
Within-group comparisons:
Control group: The mean thickness of the Schneiderian membrane was not significantly different at the three time points (P=0.06).
Test group: The mean thickness of the Schneiderian membrane was significantly different among the three time points (P<0.05). Post-hoc test applied for pairwise comparisons showed significant differences between each two time points, such that the thickness significantly increased at 1 week compared with baseline, and then
decreased by 55% at 2 months, compared with 7 days. The value at 2 months was also significantly lower than that at baseline (P<0.01).
Between-group comparisons:
The mean membrane thickness in the two groups was not significantly different at baseline (P=0.6), at 1 week (P=0.2) or 2 months (P=0.2), although the thickness at 2 months in the test group was 32% lower than that in the control group. In total, the difference between the two groups was not significant according to ANOVA (P=0.2). In power analysis, the power was 0.67 for 1 week, and 0.23 for 2 months.
Discussion
The results showed that the mean thickness of the Schneiderian membrane at one week in the test side was greater than that in the control side, although it was not significant. At 2 months, this trend was reverse, and the mean membrane thickness was slightly, but not significantly, lower in the test side.
Platelets have three types of granules:
lysosomes, alpha-granules, and dense granules. Alpha-granules contain significant amounts of growth factors. In addition to growth factors, alpha-granules contain adhesion molecules (such as P-selectin, vitronectin, fibronectin, platelet adhesion molecules, and endothelial cell adhesion molecule-1), coagulation factors (such as fibrinogen, plasminogen, and factors 5, 7, 11, and 13), and protease inhibitors [9]. Since alpha-granules of platelets contain considerable amounts of growth factors, PRP and PRF can serve as good and accessible autogenous sources of growth factors. In fact, PRP and PRF are composed of two parts of growth factors and cell adhesion molecules, which are all proteins [10].
In the present study, considering the possible role of PRF membrane in reduction of release of cytokines, reduction of inflammation, and subsequent enhancement of healing and regeneration [11], we expected lower thickness of membrane at 1 week at the test side, compared with the control side; however, the results showed higher thickness at the test side, although it was not significant. However, the results at 2 months were in line with our expectations, and the mean membrane thickness decreased at the test side;
although the difference was not significant. According to the results of study, it appears that small sample size was the reason for insignificant results; future studies with a larger sample size are required to obtain more accurate results.
In interpretation of the present results, it should be mentioned that although PRF can decrease inflammation by decreasing the release of cytokines, it increased cell adhesion [12] and subsequently the thickness of the Schneiderian membrane at 1 week in the test side due to having adhesion molecules such as P-selectin, vitronectin, fibronectin, and endothelial cell adhesion molecule-1. At 2 months, it enhanced healing of membrane due to having growth factors and reduction of pro-inflammatory cytokines [13]. This effect appeared as reduction of inflammation and subsequent reduction of membrane thickness at 2 months, compared with the control side, which can be translated to faster healing [14].
Conclusion
The present results regarding the effect of PRF on Schneiderian membrane thickness following sinus floor augmentation revealed no significant difference in the Schneiderian membrane thickness between the two sides with and without the application of PRF beneath the Schneiderian membrane thickness.
Full-Text: (633 Views)
| Abstract Background and Aim: Considering the efficacy of platelet-rich fibrin (PRF) in enhancement of healing by releasing growth factors, this study aimed to assess the efficacy of PRF application as a protective barrier right beneath the sinus membrane on the Schneiderian membrane thickness following sinus floor augmentation. Materials and Methods: This randomized controlled split-mouth clinical trial was conducted on 18 patients (36 sinuses) who required bilateral sinus floor augmentation. Two patients (n=4 sinuses) were excluded due to chronic sinusitis, and one patient due to perioperative sinus membrane perforation. Fifteen patients (n=30 sinuses) were finally assessed. In the test side, PRF membrane was placed beneath the Schneiderian membrane while augmentation was performed without a PRF membrane in the control side. Cone-beam computed tomography (CBCT) scans were taken preoperatively, and at 1 week and 2 months postoperatively, and the Schneiderian membrane thickness was compared at the two sides using ANOVA and a post-hoc test. Results: The mean membrane thickness was 1.85±0.85 mm in the control and 2.17±0.87 mm in the test group before the intervention (P=0.6). At 1 week, the mean thickness was 2.45±1.22 in the control and 3.77±1.42 mm in the case group (P=0.2). At 2 months, the mean thickness was 2.54±1.66 mm in the control and 1.71±1.31 mm in the test group (P=0.2). ANOVA showed no significant difference between the two groups at any time point (P>0.05). Conclusion: Application of PRF under the Schneiderian membrane in sinus floor augmentation had no significant effect on the Schneiderian membrane thickness. Key Words: Sinus Floor Augmentation; Maxillary Sinus; Bone Regeneration; Platelet-Rich Fibrin |
Introduction
Reconstruction of an edentulous posterior maxilla by dental implants has always been a challenge due to the presence of low-density bone and sinus pneumatization [1-3]. In case of no augmentation, progressive bone loss continues, and treatment with implant-supported restorations will be problematic and associated with high risk of failure [3,4]. Several techniques have been proposed to augment bone with optimal quality and quantity for implant placement; among which, sinus floor augmentation is a more predictable method, which was first performed by Boyne and James [4]. It is still commonly performed due to its high success rate. In sinus floor augmentation procedures, the sinus membrane status and preserving its integrity are highly important. High variations have been reported in sinus membrane thickness [5]. Makary et al. [6] reported a significant increase in sinus membrane thickness after sinus floor augmentation by the lateral approach. This increase in thickness may be due to a physiological inflammatory reaction to surgical trauma, including bleeding and inflammation in primary phases of healing [6]. Although reaction of nasal and paranasal mucosa to different factors such as infection, allergy, and surgical trauma has been well documented, sinus membrane response to sinus floor elevation by the lateral approach has been less commonly assessed [6].
Watelet et al. [7] clearly described the wound healing process in nasal and paranasal mucosa. They divided this process into four overlapping phases of inflammation, cell proliferation, matrix deposition, and tissue remodeling. Healing phases in sinus floor augmentation including the lateral window approach have also been described [7].
Platelet products were first used for prevention and treatment of hemorrhage due to severe thrombocytopenia. Standard platelet concentrate was first referred to as platelet-rich plasma (PRP), which classically included 0.5 x 1011 platelets per each unit. Platelet products are used to enhance bone regeneration by release of growth factors. Platelets contain a high volume of key growth factors such as platelet-derived growth factors, B1 and B2 transforming growth factors, and vascular endothelial growth factor that can induce and enhance cell proliferation and angiogenesis. To date, several techniques for the use of autologous platelet concentrates have been developed [8].
Considering the role of PRF in enhancement of healing by release of growth factors, this study aimed to assess the effect of PRF as a protective barrier beneath the sinus membrane on the Schneiderian membrane thickness following sinus floor augmentation surgery.
Materials and Methods
In this randomized controlled split-mouth clinical trial, cone-beam computed tomography (CBCT) scans were used to assess the Schneiderian membrane thickness at the deepest point of the maxillary sinus. Eighteen patients (36 maxillary sinuses) who required bilateral sinus floor augmentation due to sinus pneumatization and bone resorption according to clinical and radiographic examinations were selected. The inclusion criteria were residual crestal bone thickness between the sinus floor and bone crest to be maximally 3 mm and O’Leary’s plaque index < 20%. The exclusion criteria were acute sinus infection, chronic sinusitis, allergy, cigarette smoking, treatment with bisphosphonates, uncontrolled diabetes mellitus, and pregnancy. Two patients (4 sinuses) were excluded due to chronic sinusitis, and one patient was excluded due to perioperative sinus membrane perforation. Finally, 15 patients (30 sinuses) were studied, and underwent CBCT. The study was approved by the ethics committee of the university (IR.IAU.DENTAL.REC.1397.051) and registered in the Iranian Registry of Clinical Trials IRCT22710201972016).
After phase I periodontal therapy (if required) and oral hygiene instruction, the O’Leary’s plaque index of patients was calculated to ensure it is below 20%. Next, the patients were asked to rinse their mouth with 0.2% chlorhexidine gluconate (Iran Behdasht, Iran) for 30 seconds prior to the surgical procedure. Local anesthesia was induced with 2% lidocaine plus 1:100,000 epinephrine (Darupakhsh, Iran). A crestal incision was made along with two vertical releasing incision at the mesial and distal to elevate a full-thickness flap and expose the buccal (lateral) wall of the maxillary sinus. The lateral window was opened by using the Dask kit (Dentium, Seoul, South Korea). The sinus membrane was elevated and a PRF membrane was placed beneath the Schneiderian membrane at the test side. PRF membrane was not used for the control side. Allocation of each side to the test or control group in each patient was performed randomly by flipping a dice. As mentioned earlier, sinus membrane perforation occurred during retraction of tissue in one patient, and this patient was excluded from the study.
PRF was prepared as follows: right before the surgical procedure, 9 mL of venous blood was obtained from the patients according to the Choukroun protocol [9], and collected in dry capped glass or plastic tubes coated with anticoagulant agent, and centrifuged in L-PRF centrifuge machine (Intra-Lock; Intrapsin, USA). Centrifugation resulted in formation of three layers: a red blood cell layer at the bottom, a cell-free plasma layer on the top, and PRF clot in the middle. PRF layer was collected by sterile hemostat and was cut from the red blood cell layer by scissors. Sinus floor augmentation was then performed using 1000-2000 μm xenograft granules (Cerabone, Botiss, Germany). A xenograft membrane (Jason, Botiss, Germany) was placed over the lateral window, the flap was returned, and sutured with 4-0 silk sutures (Surgical Silk; Supa, Iran).
Postoperative instructions:
All patients were prescribed 400 mg ibuprofen (Arya, Iran) every 6 hours for 1 week. Co-amoxiclav (625 mg; Farabi, Iran) was prescribed prophylactically to be taken daily for 7 to 10 days. Allergic patients were prescribed 600 mg clindamycin instead. Also, the patients were instructed to rinse 0.2% chlorhexidine mouthwash (Iran Behdasht, Iran) for 15 days after surgery. The sutures were removed after 7 days, and the patients were clinically and radiographically examined at 1 week and 2 months, postoperatively, and underwent CBCT of the surgical site.
Imaging:
CBCT scans were taken using 3D Mid Planmeca CBCT scanner (Finland) with 0.2 mm voxel size, 8 mA amperage, and 90 kV voltage with 12.05 s exposure time. All CBCT images were obtained with 4 x 4, 6 x 6, and 8 x 8 cm fields of view. Images were reconstructed with 0.5 mm slice intervals.
Image assessment:
CBCT images were assessed by an experienced radiologist who was not directly involved in the process of treatment and follow-up of patients. To ensure optimal calibration and intra-examiner reliability, each measurement was repeated, and the mean value was calculated; when the difference between the two measurements was 0.2 mm or higher, measurement was repeated for the third time. CBCT images were analyzed on a 22-inch monitor (Samsung; Korea) with 1024 x 1224-pixel resolution. Measurements were made using Planmeca Romexis version 5.1.0 software.
Measuring the Schneiderian membrane thickness:
CBCT sections were reformatted such that the posterior segment of the maxilla (from the first premolar to the second molar) on axial sections was oriented vertically while the floor of the nose and palate on coronal sections was oriented horizontally. Next, three standard measurements were made from the Schneiderian membrane dimensions in millimeters using coronal CBCT sections of the anterior part of the maxillary sinus in lateral (alat) dimension followed by mid-sagittal (amid) and medial (amed) dimensions. The selected anterior section from the maxillary sinus floor matched the area between the apices of maxillary premolars in a dentate patient (Figure 1).
Figure 1. Measurements made on sagittal CBCT sections: (a) anterior section (PM1: first premolar, PM2: second premolar), (m) middle section (M1: first molar), and (p) posterior section (M2: second molar, M3: third molar).
{kind=link}
(a)Patient with free-end maxillary edentulous ridge; (b) patient with single tooth loss in the left posterior maxilla.
The following anatomical landmarks were measured on coronal CBCT sections for standard measurements (Figure 2a-c):
(I) Initiation point of the zygomatic process for lateral measurements (alat)
(II)Deepest point of the sinus floor on coronal CBCT sections for mid-sagittal measurement (amid)
(III)Skeletal floor of the nasal cavity of the same side for medial measurement (amed)
In cases where the sinus floor had a higher (more cranial) position relative to the zygomatic process or skeletal floor of the nasal cavity, the lateral (lat) and medial (med)
measurements were made at the level of initiation of inferior nasal concha of the same side. The three measurements were repeated in the middle part (Figure 1, m) corresponding to the maxillary first molar apex (mmed, mmid, mlat) and in the posterior region corresponding to the area between the apices of maxillary second and third molars in a dentate patient (pmed, pmid, and plat). In the edentulous posterior regions, the distance between the premolar roots was adjusted to be 7 mm, and the distance between the molar roots was adjusted to be 8 mm. Thus, radiographic assessments included 9 separate measurements for each maxillary sinus (Figure 3, 4) [8]. All measurements related to the mucosal thickness were performed perpendicular to the underlying bone (initiating from the underlying bone plate and terminating at the mucosal surface).
Statistical analysis:
The two groups were compared regarding the Schneiderian membrane thickness by paired t-test.
Figure 2. Anatomical landmarks for measurement of mucosal thickness on coronal CBCT sections in the anterior (a), middle (b) and posterior (c) areas.
{kind=link}
Initiation point of zygomatic process for lateral
measurements (lat), deepest point of the sinus floor on coronal CBCT sections for mid-sagittal
measurement (mid), skeletal floor of the nasal cavity of the same side for medial measurement (med).
Dotted red line indicates the position of skeletal floor of the nasal cavity. Continuous red line indicates the inferior nasal concha
Figure 3. L-PRF clot was removed from the tube
{kind=link}
Figure 4. Weight of the cap resulted in formation of a membrane from the L-PRF clot
{kind=link}
Results
The Schneiderian membrane thickness was measured and compared in patients undergoing sinus floor augmentation with and without PRF membrane in a split-mouth design before and at 1 week and 2 months after surgery. A total of 15 patients including 8 females and 7 males between 42 to 68 years (mean age of 53.6± 0.18 years) were evaluated (30 sinuses). All patients were followed-up for 2 months, and surgical procedures of each patient were performed within one session. In the test side, L-PRF membrane was used beneath the Schneiderian membrane while the other side served as the control side and did not receive L-PRF membrane.
Table 1 presents the mean thickness of the Schneiderian membrane in 30 sinuses in
{kind=link}
15 patients at the three time points in millimeters. The minimum and maximum thickness of the Schneiderian membrane preoperatively was 0.73 mm and 3.08 mm, respectively.
Within-group comparisons:
Control group: The mean thickness of the Schneiderian membrane was not significantly different at the three time points (P=0.06).
Test group: The mean thickness of the Schneiderian membrane was significantly different among the three time points (P<0.05). Post-hoc test applied for pairwise comparisons showed significant differences between each two time points, such that the thickness significantly increased at 1 week compared with baseline, and then
decreased by 55% at 2 months, compared with 7 days. The value at 2 months was also significantly lower than that at baseline (P<0.01).
Between-group comparisons:
The mean membrane thickness in the two groups was not significantly different at baseline (P=0.6), at 1 week (P=0.2) or 2 months (P=0.2), although the thickness at 2 months in the test group was 32% lower than that in the control group. In total, the difference between the two groups was not significant according to ANOVA (P=0.2). In power analysis, the power was 0.67 for 1 week, and 0.23 for 2 months.
Discussion
The results showed that the mean thickness of the Schneiderian membrane at one week in the test side was greater than that in the control side, although it was not significant. At 2 months, this trend was reverse, and the mean membrane thickness was slightly, but not significantly, lower in the test side.
Platelets have three types of granules:
lysosomes, alpha-granules, and dense granules. Alpha-granules contain significant amounts of growth factors. In addition to growth factors, alpha-granules contain adhesion molecules (such as P-selectin, vitronectin, fibronectin, platelet adhesion molecules, and endothelial cell adhesion molecule-1), coagulation factors (such as fibrinogen, plasminogen, and factors 5, 7, 11, and 13), and protease inhibitors [9]. Since alpha-granules of platelets contain considerable amounts of growth factors, PRP and PRF can serve as good and accessible autogenous sources of growth factors. In fact, PRP and PRF are composed of two parts of growth factors and cell adhesion molecules, which are all proteins [10].
In the present study, considering the possible role of PRF membrane in reduction of release of cytokines, reduction of inflammation, and subsequent enhancement of healing and regeneration [11], we expected lower thickness of membrane at 1 week at the test side, compared with the control side; however, the results showed higher thickness at the test side, although it was not significant. However, the results at 2 months were in line with our expectations, and the mean membrane thickness decreased at the test side;
although the difference was not significant. According to the results of study, it appears that small sample size was the reason for insignificant results; future studies with a larger sample size are required to obtain more accurate results.
In interpretation of the present results, it should be mentioned that although PRF can decrease inflammation by decreasing the release of cytokines, it increased cell adhesion [12] and subsequently the thickness of the Schneiderian membrane at 1 week in the test side due to having adhesion molecules such as P-selectin, vitronectin, fibronectin, and endothelial cell adhesion molecule-1. At 2 months, it enhanced healing of membrane due to having growth factors and reduction of pro-inflammatory cytokines [13]. This effect appeared as reduction of inflammation and subsequent reduction of membrane thickness at 2 months, compared with the control side, which can be translated to faster healing [14].
Conclusion
The present results regarding the effect of PRF on Schneiderian membrane thickness following sinus floor augmentation revealed no significant difference in the Schneiderian membrane thickness between the two sides with and without the application of PRF beneath the Schneiderian membrane thickness.
Type of Study: Original article |
Subject:
Periodontology
References
1. Ali S, Bakry SA, Abd-Elhakam H. Platelet-Rich Fibrin in Maxillary Sinus Augmentation: A Systematic Review. J Oral Implantol. 2015 Dec;41(6):746-53. [DOI:10.1563/AAID-JOI-D-14-00167] [PMID]
2. Chiapasco M, Zaniboni M, Rimondini L. Dental implants placed in grafted maxillary sinuses: a retrospective analysis of clinical outcome according to the initial clinical situation and a proposal of defect classification. Clin Oral Implants Res. 2008 Apr;19(4):416-28. [DOI:10.1111/j.1600-0501.2007.01489.x] [PMID]
3. Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008 Feb;19(2):119-30. [DOI:10.1111/j.1600-0501.2007.01453.x] [PMID]
4. Aguirre Zorzano LA, Rodríguez Tojo MJ, Aguirre Urizar JM. Maxillary sinus lift with intraoral autologous bone and B--tricalcium phosphate: histological and histomorphometric clinical study. Med Oral Patol Oral Cir Bucal. 2007 Nov 1;12(7):E532-6.
5. Janner SF, Caversaccio MD, Dubach P, Sendi P, Buser D, Bornstein MM. Characteristics and dimensions of the Schneiderian membrane: a radiographic analysis using cone beam computed tomography in patients referred for dental implant surgery in the posterior maxilla. Clin Oral Implants Res. 2011 Dec;22(12):1446-53. [DOI:10.1111/j.1600-0501.2010.02140.x] [PMID]
6. Makary C, Rebaudi A, Menhall A, Naaman N. Changes in Sinus Membrane Thickness After Lateral Sinus Floor Elevation: A Radiographic Study. Int J Oral Maxillofac Implants. 2016 Mar-Apr;31(2):331-7. [DOI:10.11607/jomi.4108] [PMID]
7. Watelet JB, Bachert C, Gevaert P, Van Cauwenberge P. Wound healing of the nasal and paranasal mucosa: a review. Am J Rhinol. 2002 Mar-Apr;16(2):77-84. [DOI:10.1177/194589240201600202] [PMID]
8. Elbaradie R, Ossman S, Eldibany R: Evaluation of platelet rich fibrin in sinus lifting with simultaneous implant placement. Alexandria Dent J 2015 July ;40(1):72-8. [DOI:10.21608/adjalexu.2015.58739]
9. Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunité en paro-implantologie: Le PRF. Implantodontie2001;42:55-62.
10. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998 Jun;85(6):638-46. [DOI:10.1016/S1079-2104(98)90029-4]
11. El-Sharkawy H, Kantarci A, Deady J, Hasturk H, Liu H, Alshahat M, Van Dyke TE. Platelet-rich plasma: growth factors and pro- and anti-inflammatory properties. J Periodontol. 2007 Apr;78(4):661-9. [DOI:10.1902/jop.2007.060302] [PMID]
12. Chandrun P, Sivadas A. Platelet-rich fibrin: Its role in periodontal regeneration. The Saudi Journal for Dental Research: 2014 ; 5(2):177-22. [DOI:10.1016/j.ksujds.2013.09.001]
13. Kumar YR, Mohanty S, Verma M, Kaur RR, Bhatia P, Kumar VR, Chaudhary Z. Platelet-rich fibrin: the benefits. Br J Oral Maxillofac Surg. 2016 Jan;54(1):57-61. [DOI:10.1016/j.bjoms.2015.10.015] [PMID]
14. Temmerman A, Cleeren GJ, Castro AB, Teughels W, Quirynen M. L-PRF for increasing the width of keratinized mucosa around implants: A split-mouth, randomized, controlled pilot clinical trial. J Periodontal Res. 2018 Oct; 53 (5):793-800. [DOI:10.1111/jre.12568] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
