

Volume 4, Issue 3 (9-2019)
J Res Dent Maxillofac Sci 2019, 4(3): 21-29 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Salimzadeh S, SHeykhNezhad H, Zohri Z, Salimzadeh P. Comparison of the Frequency of Temporomandibular Disorders Between β-Thalassemia Major Patients and High School and Guidance School Students. J Res Dent Maxillofac Sci 2019; 4 (3) :21-29
URL: http://jrdms.dentaliau.ac.ir/article-1-223-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-223-en.html


1- Periodontal Dept, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran , dr.ssalimzade@gmail.com
2- Assistant Professor, Department of Prothesis, Guilan University of Medical Sciences, Rasht, Iran
3- Periodontist, department of periodontology,school of dentistry, Guilan University of Medical Sciences,
4- Dentist
2- Assistant Professor, Department of Prothesis, Guilan University of Medical Sciences, Rasht, Iran
3- Periodontist, department of periodontology,school of dentistry, Guilan University of Medical Sciences,
4- Dentist
Full-Text [PDF 292 kb]
(1321 Downloads)
| Abstract (HTML) (2703 Views)
Abstract
Background and Aim: Patients affected by thalassemia major show great skeletal changes in the head and neck area in addition to malocclusion. It seems that examination of malocclusion in these patients and evaluation of the frequency of temporomandibular disorders (TMD) can help identify people with a high risk of illness in the society. The current study aimed to compare the frequency of TMD between β-thalassemia major patients and high school and guidance school students.
Materials and Methods: In this descriptive-analytical study, 51 patients affected by thalassemia major (23 girls and 28 boys) and 78 normal (43 girls and 35 boys) guidance and high school students between 12 and 18 years old were evaluated. The presence of TMD and malocclusion and their relationship were determined. After examination and completion of the related questionnaire, data were analyzed by chi-square test and t-test using SPSS software.
Results: According to the data, there was no significant difference in spacing, occlusion, crowding, open bite, headache, bruxism, crepitation, clicking, TMD, subluxation, locking, cleaning, deviation, deep bite, and crossbite between the control and thalassemia students (P>0.05). However, significant differences were observed regarding overjet and pain (P<0.05).
Conclusion: These results suggest that TMD and occlusion type have no significant correlation with thalassemia.
Keywords: Thalassemia, Temporomandibular Joint Disorders, Malocclusion
Introduction
Thalassemia is a hereditary disease that occurs because of mutations in the synthesis of hemoglobin α- and β-chains, leading to chronic and severe anemia. (1) Thalassemia has two main forms: heterozygous, known as mild (minor), and homozygous or β-thalassemia (thalassemia major, also known as Cooley’s anemia and Mediterranean anemia). The latter shows the most severe symptoms. (2) β-thalassemia causes severe anemia that begins after birth and leads to serious complications. (3) These patients show severe cardiac failure, chronic anemia, and hypoxia. (3) Thalassemia is a widespread disease distributed in Africa, the Middle East, the Mediterranean area, Southeast Asia, and the Pacific islands. (1)
The articular eminence is a part of the temporal bone that forms the joint. It is located on the anterior part of the articular cavity; the condyle slips on it during mandibular movement. (4) The morphologic changes and asymmetry observed in the temporomandibular joint (TMJ) are influenced by several factors including abrasion, premature contacts, avascular necrosis, unilateral crossbite, and dentoskeletal asymmetries. (5) When the slope of the articular eminence is more than normal, the condyle is forced towards more lateral movements rather than anterior movements, which result in more vertical displacement of the condyle and the mandible during mandibular opening and may cause the loosening of the ligaments that connect the disc to the condyle. (6) Normal variations in condylar morphology occur with age, gender, face shape, occlusal force, functional load, and malocclusion between the left and right sides. The higher prevalence of morphological changes in the TMJ in older people is due to the onset of joint degeneration. (7) These patients also show bone deformities, growth abnormalities, and hepatosplenomegaly. (8) Craniofacial manifestations are common features of β-thalassemia patients and include bony changes due to ineffective erythropoiesis. (9) These changes include vertical growth of the mandible, short mandibular body, prominent malar bone, depressed nasal bridge, partially obliterated maxillary sinus, delayed pneumatization of the maxillary sinuses, upper lip retraction, and altered ramus length, leading to Class II malocclusions. (10) These changes cause osteoporosis and marrow space expansion in long bones, the skull, and facial bones. Also, rodent face appearance is common in these patients. (11)
In the evaluation of the craniofacial morphology of Iranian children with β-thalassemia, Amini et al reported that anemia produces overgrowth of the maxilla, the condyle, and the ramus of the mandible, leading to Class II malocclusions and a soft-tissue profile for orthodontic or orthognathic management. (3)
The current study aimed to compare the frequency of TMD between β-thalassemia major patients and high and guidance school students.
Materials and Methods
In this descriptive-analytical study, 51 patients affected by thalassemia major, referring to the 17th Shahrivar Hospital (Rasht, Iran) and 78 normal 12-18-year-old guidance and high school students in Rasht city (Iran) were evaluated. This study received approval from the Research Ethics Committee of Gilan University of Medical Sciences, Rasht, Iran.
After the exclusion of subjects who had a history of orthodontic therapy, surgery or trauma in the craniofacial area, the samples were allocated as 51 β-thalassemia major patients (23 girls and 28 boys) and 78 normal (43 girls and 35 boys) guidance and high school students between 12 and 18 years old. The presence of TMD and malocclusion and their relationship were determined. Clicking, crepitation, spacing, crowding, deviation and deflection, crossbite, open bite, overbite, overjet, bruxism, clenching, trauma, subluxation, locking, headache, pain, TMD, and malocclusion were evaluated, and occlusion types (I, II, III) were determined.
The clinical examination began by directly palpating over the joint while the subject opened and closed the mandible, and the extent of the condylar movement was assessed. The joint was auscultated during the mandibular motion to examine crepitus, grinding, and clicking or popping sounds. The degree of mandibular opening was measured using the distance between the incisal edges of the upper and lower incisors; the opening of less than 35 mm was considered abnormal. Mandibular deviation was also assessed.(5,7)
After examination and completion of the related questionnaire, data were analyzed by chi-square test and t-test using SPSS software (SPSS Inc., Chicago, IL, USA). P-values lower than 0.05 were considered statistically significant.
Results
As seen in Table 1, 51 participants had thalassemia and 78 participants were normal.
Table 1. Distribution of the participants
Also, no significant differences were observed regarding crepitation, clicking, TMD, subluxation, locking, and cleaning between the control and thalassemia groups (P>0.05).
Table 4. Frequency of temporomandibular disorders (TMD) among the participants
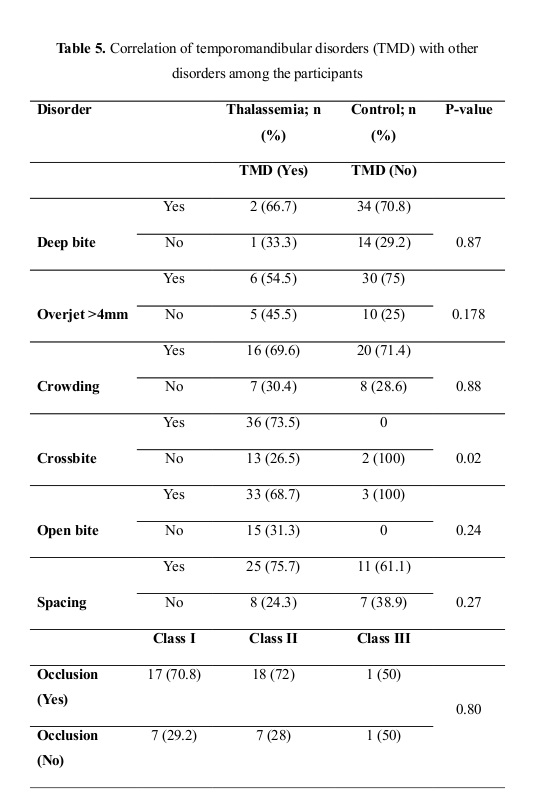
The results of the comparison of TMD frequency among the participants is presented in Table 5. As seen, there was no significant difference in deep bite, overjet, crowding, open bite, spacing, and occlusion classes between the control and thalassemia groups (P>0.05). However, significant differences were observed regarding crossbite between the control and thalassemia groups (P<0.05).
Discussion
Patients affected by thalassemia major show great skeletal changes in the craniofacial area in addition to malocclusion. It seems that examination of malocclusion in these patients and evaluation of the frequency of TMD can help identify people with a high risk of illness in the society. In this study, we determined the frequency of TMD in β-thalassemia major patients and normal high and guidance school students. There are no reports on the craniofacial characteristics of the Iranians suffering from thalassemia.
According to the data, there was no significant difference in spacing, occlusion, crowding, crossbite, open bite, headache, bruxism, crepitation, clicking, TMD, subluxation, locking, cleaning, deviation, deep bite, and occlusion classes between the control and thalassemia groups. However, significant differences were observed regarding overjet and pain.
TMD is a generic term describing any clinical problem in the TMJ associated with orofacial pain and mandibular dysfunction. (12) In patients with TMD, the deterioration of articular cartilage, bone remodeling, and inflammatory changes occur in the TMJ. Although the diagnosis of TMD is usually based on the clinical symptoms and signs, a variety of imaging techniques, including skeletal radiography, computed tomography (CT), magnetic resonance imaging (MRI), and bone scintigraphy, provide valuable information for TMD diagnosis in clinical practice. Various physical, radiographic, and nuclear medicine examinations are used to diagnose TMD. (13)
Erosion, condylar hyperplasia, concavity, bifid condyle, condylar hypoplasia, and sclerosis are the most common manifestations, respectively. However, researchers have reported no significant differences in the prevalence of abnormal findings with the patient’s gender, dental status, and occlusion. (14) Nonetheless, they reported that the prevalence of abnormal radiographic findings increases in older patients. (14) In the current study, a significant correlation was observed between locking-right and limitation-right, crepitus-left and crepitus-right, locking-left and limitation-right, subluxation-right and click-right and subluxation-right, and subluxation-left and subluxation-right. Perhaps, the age of the case group was low, which may have affected our results; further research on older patients is recommended.
Brooks et al reported flattening in 35% of the participants. (15) Katzberg et al reported flattening in 52% of patients between the ages of 20 and 69 years. (16) It has been reported that flattening is the most frequent finding in the condyles of young people under orthodontic treatments. (14) Also, Katzberg et al reported that sclerosis, concavity, osteophyte, erosion, and cysts were respectively the most common mandibular disorders after flattening. Additionally, flattening, osteophyte, sclerosis, concavity, erosion, and cysts are the most common complications. (17) Other joint disorders such as erosion, condylar hyperplasia, concavity, bifid condyle, condylar hypoplasia, sclerosis, osteophyte, and subcortical cysts have also been reported. (14)
The retarding effect of thalassemia on general skeletal growth has been reported. (18) In thalassemia patients, premature fusion of the epiphysis of long bones leads to shortening of the proximal humerus. (19) β-thalassemia patients have reduced craniofacial dimensions. (20) In β-thalassemia patients, the main craniofacial manifestation is Class II skeletal malocclusion associated with a strong vertical growth pattern. (19) The vertical growth of the mandible in these patients was in agreement with the findings reported in Qatar and Syria. (20,21) The bones become thinner, and pathological fractures may occur. (8) Overexpansion of the bone marrow leads to changes in typical facial and cranial bones. (8) The subperiosteal growth of the ramus and the mandibular cartilage leads to subsequent complications including severe chronic anemia, endocrine dysfunction, and growth hormone insensitivity. (1) In agreement with previous reports, the facial appearance of thalassemia patients follows their substantial skeletal discrepancy. (1) Prominent lips accompany a small chin. (3) Thalassemia patients exhibit severe facial disfigurements with reduced posterior facial height and increased anterior facial proportions. (20)
β-thalassemia is a transfusion-dependent disease. (8) Treatment of β-thalassemia includes regular blood transfusions to prevent anemia-induced heart failure. (8) Regular red blood cell transfusion is the recommended treatment for β-thalassemia, which is usually administered every 2-5 weeks to maintain the pre-transfusion hemoglobin level (9-10.5 g/dl). (22) A blood transfusion regimen induces normal growth and inhibits excess bone marrow activity. (23)
Conclusion
In conclusion, these results suggest that TMD and occlusion type have no significant correlation with thalassemia.
Full-Text: (801 Views)
Abstract
Background and Aim: Patients affected by thalassemia major show great skeletal changes in the head and neck area in addition to malocclusion. It seems that examination of malocclusion in these patients and evaluation of the frequency of temporomandibular disorders (TMD) can help identify people with a high risk of illness in the society. The current study aimed to compare the frequency of TMD between β-thalassemia major patients and high school and guidance school students.
Materials and Methods: In this descriptive-analytical study, 51 patients affected by thalassemia major (23 girls and 28 boys) and 78 normal (43 girls and 35 boys) guidance and high school students between 12 and 18 years old were evaluated. The presence of TMD and malocclusion and their relationship were determined. After examination and completion of the related questionnaire, data were analyzed by chi-square test and t-test using SPSS software.
Results: According to the data, there was no significant difference in spacing, occlusion, crowding, open bite, headache, bruxism, crepitation, clicking, TMD, subluxation, locking, cleaning, deviation, deep bite, and crossbite between the control and thalassemia students (P>0.05). However, significant differences were observed regarding overjet and pain (P<0.05).
Conclusion: These results suggest that TMD and occlusion type have no significant correlation with thalassemia.
Keywords: Thalassemia, Temporomandibular Joint Disorders, Malocclusion
Introduction
Thalassemia is a hereditary disease that occurs because of mutations in the synthesis of hemoglobin α- and β-chains, leading to chronic and severe anemia. (1) Thalassemia has two main forms: heterozygous, known as mild (minor), and homozygous or β-thalassemia (thalassemia major, also known as Cooley’s anemia and Mediterranean anemia). The latter shows the most severe symptoms. (2) β-thalassemia causes severe anemia that begins after birth and leads to serious complications. (3) These patients show severe cardiac failure, chronic anemia, and hypoxia. (3) Thalassemia is a widespread disease distributed in Africa, the Middle East, the Mediterranean area, Southeast Asia, and the Pacific islands. (1)
The articular eminence is a part of the temporal bone that forms the joint. It is located on the anterior part of the articular cavity; the condyle slips on it during mandibular movement. (4) The morphologic changes and asymmetry observed in the temporomandibular joint (TMJ) are influenced by several factors including abrasion, premature contacts, avascular necrosis, unilateral crossbite, and dentoskeletal asymmetries. (5) When the slope of the articular eminence is more than normal, the condyle is forced towards more lateral movements rather than anterior movements, which result in more vertical displacement of the condyle and the mandible during mandibular opening and may cause the loosening of the ligaments that connect the disc to the condyle. (6) Normal variations in condylar morphology occur with age, gender, face shape, occlusal force, functional load, and malocclusion between the left and right sides. The higher prevalence of morphological changes in the TMJ in older people is due to the onset of joint degeneration. (7) These patients also show bone deformities, growth abnormalities, and hepatosplenomegaly. (8) Craniofacial manifestations are common features of β-thalassemia patients and include bony changes due to ineffective erythropoiesis. (9) These changes include vertical growth of the mandible, short mandibular body, prominent malar bone, depressed nasal bridge, partially obliterated maxillary sinus, delayed pneumatization of the maxillary sinuses, upper lip retraction, and altered ramus length, leading to Class II malocclusions. (10) These changes cause osteoporosis and marrow space expansion in long bones, the skull, and facial bones. Also, rodent face appearance is common in these patients. (11)
In the evaluation of the craniofacial morphology of Iranian children with β-thalassemia, Amini et al reported that anemia produces overgrowth of the maxilla, the condyle, and the ramus of the mandible, leading to Class II malocclusions and a soft-tissue profile for orthodontic or orthognathic management. (3)
The current study aimed to compare the frequency of TMD between β-thalassemia major patients and high and guidance school students.
Materials and Methods
In this descriptive-analytical study, 51 patients affected by thalassemia major, referring to the 17th Shahrivar Hospital (Rasht, Iran) and 78 normal 12-18-year-old guidance and high school students in Rasht city (Iran) were evaluated. This study received approval from the Research Ethics Committee of Gilan University of Medical Sciences, Rasht, Iran.
After the exclusion of subjects who had a history of orthodontic therapy, surgery or trauma in the craniofacial area, the samples were allocated as 51 β-thalassemia major patients (23 girls and 28 boys) and 78 normal (43 girls and 35 boys) guidance and high school students between 12 and 18 years old. The presence of TMD and malocclusion and their relationship were determined. Clicking, crepitation, spacing, crowding, deviation and deflection, crossbite, open bite, overbite, overjet, bruxism, clenching, trauma, subluxation, locking, headache, pain, TMD, and malocclusion were evaluated, and occlusion types (I, II, III) were determined.
The clinical examination began by directly palpating over the joint while the subject opened and closed the mandible, and the extent of the condylar movement was assessed. The joint was auscultated during the mandibular motion to examine crepitus, grinding, and clicking or popping sounds. The degree of mandibular opening was measured using the distance between the incisal edges of the upper and lower incisors; the opening of less than 35 mm was considered abnormal. Mandibular deviation was also assessed.(5,7)
After examination and completion of the related questionnaire, data were analyzed by chi-square test and t-test using SPSS software (SPSS Inc., Chicago, IL, USA). P-values lower than 0.05 were considered statistically significant.
Results
As seen in Table 1, 51 participants had thalassemia and 78 participants were normal.
Table 1. Distribution of the participants
{kind=link}
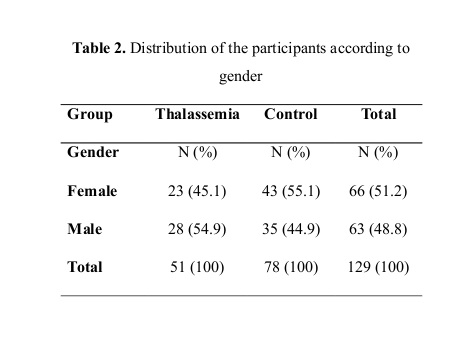
There was no significant difference between the two groups regarding gender (P=0.265; Table 2).
Table 2. Distribution of the participants according to gender
Table 2. Distribution of the participants according to gender
{kind=link}
The frequency of TMD in the participants is presented in Tables 3 and 4. According to the data, there was no significant difference in spacing, occlusion, crowding, crossbite, open bite, headache, bruxism, and deviation between the control and thalassemia groups (P>0.05). However, significant differences were observed regarding overjet and pain (P<0.05).
Table 3. Frequency of temporomandibular disorders (TMD) among the participants
Table 3. Frequency of temporomandibular disorders (TMD) among the participants
{kind=link}
Also, no significant differences were observed regarding crepitation, clicking, TMD, subluxation, locking, and cleaning between the control and thalassemia groups (P>0.05).
Table 4. Frequency of temporomandibular disorders (TMD) among the participants
{kind=link}
The results of the comparison of TMD frequency among the participants is presented in Table 5. As seen, there was no significant difference in deep bite, overjet, crowding, open bite, spacing, and occlusion classes between the control and thalassemia groups (P>0.05). However, significant differences were observed regarding crossbite between the control and thalassemia groups (P<0.05).
{kind=link}
Discussion
Patients affected by thalassemia major show great skeletal changes in the craniofacial area in addition to malocclusion. It seems that examination of malocclusion in these patients and evaluation of the frequency of TMD can help identify people with a high risk of illness in the society. In this study, we determined the frequency of TMD in β-thalassemia major patients and normal high and guidance school students. There are no reports on the craniofacial characteristics of the Iranians suffering from thalassemia.
According to the data, there was no significant difference in spacing, occlusion, crowding, crossbite, open bite, headache, bruxism, crepitation, clicking, TMD, subluxation, locking, cleaning, deviation, deep bite, and occlusion classes between the control and thalassemia groups. However, significant differences were observed regarding overjet and pain.
TMD is a generic term describing any clinical problem in the TMJ associated with orofacial pain and mandibular dysfunction. (12) In patients with TMD, the deterioration of articular cartilage, bone remodeling, and inflammatory changes occur in the TMJ. Although the diagnosis of TMD is usually based on the clinical symptoms and signs, a variety of imaging techniques, including skeletal radiography, computed tomography (CT), magnetic resonance imaging (MRI), and bone scintigraphy, provide valuable information for TMD diagnosis in clinical practice. Various physical, radiographic, and nuclear medicine examinations are used to diagnose TMD. (13)
Erosion, condylar hyperplasia, concavity, bifid condyle, condylar hypoplasia, and sclerosis are the most common manifestations, respectively. However, researchers have reported no significant differences in the prevalence of abnormal findings with the patient’s gender, dental status, and occlusion. (14) Nonetheless, they reported that the prevalence of abnormal radiographic findings increases in older patients. (14) In the current study, a significant correlation was observed between locking-right and limitation-right, crepitus-left and crepitus-right, locking-left and limitation-right, subluxation-right and click-right and subluxation-right, and subluxation-left and subluxation-right. Perhaps, the age of the case group was low, which may have affected our results; further research on older patients is recommended.
Brooks et al reported flattening in 35% of the participants. (15) Katzberg et al reported flattening in 52% of patients between the ages of 20 and 69 years. (16) It has been reported that flattening is the most frequent finding in the condyles of young people under orthodontic treatments. (14) Also, Katzberg et al reported that sclerosis, concavity, osteophyte, erosion, and cysts were respectively the most common mandibular disorders after flattening. Additionally, flattening, osteophyte, sclerosis, concavity, erosion, and cysts are the most common complications. (17) Other joint disorders such as erosion, condylar hyperplasia, concavity, bifid condyle, condylar hypoplasia, sclerosis, osteophyte, and subcortical cysts have also been reported. (14)
The retarding effect of thalassemia on general skeletal growth has been reported. (18) In thalassemia patients, premature fusion of the epiphysis of long bones leads to shortening of the proximal humerus. (19) β-thalassemia patients have reduced craniofacial dimensions. (20) In β-thalassemia patients, the main craniofacial manifestation is Class II skeletal malocclusion associated with a strong vertical growth pattern. (19) The vertical growth of the mandible in these patients was in agreement with the findings reported in Qatar and Syria. (20,21) The bones become thinner, and pathological fractures may occur. (8) Overexpansion of the bone marrow leads to changes in typical facial and cranial bones. (8) The subperiosteal growth of the ramus and the mandibular cartilage leads to subsequent complications including severe chronic anemia, endocrine dysfunction, and growth hormone insensitivity. (1) In agreement with previous reports, the facial appearance of thalassemia patients follows their substantial skeletal discrepancy. (1) Prominent lips accompany a small chin. (3) Thalassemia patients exhibit severe facial disfigurements with reduced posterior facial height and increased anterior facial proportions. (20)
β-thalassemia is a transfusion-dependent disease. (8) Treatment of β-thalassemia includes regular blood transfusions to prevent anemia-induced heart failure. (8) Regular red blood cell transfusion is the recommended treatment for β-thalassemia, which is usually administered every 2-5 weeks to maintain the pre-transfusion hemoglobin level (9-10.5 g/dl). (22) A blood transfusion regimen induces normal growth and inhibits excess bone marrow activity. (23)
Conclusion
In conclusion, these results suggest that TMD and occlusion type have no significant correlation with thalassemia.
Type of Study: Original article |
Subject:
Oral pathology
References
1. 1. Amini F, Borzabadi-Farahani A, Mashayekhi Z, Pousti M, Amirtouri M. Soft-tissue profile characteristics in children with beta thalassaemia major. Acta Odontol Scand. 2013 Sep;71(5):1071-6. [DOI:10.3109/00016357.2012.741707] [PMID]
2. Galanello R, Origa R. Beta-thalassemia. Orphanet J Rare Dis. 2010 May 21;5:11. [DOI:10.1186/1750-1172-5-11] [PMID] [PMCID]
3. Amini F, Jafari A, Eslamian L, Sharifzadeh S. A cephalometric study on craniofacial morphology of Iranian children with beta‐thalassemia major. Orthod Craniofac Res. 2007 Feb;10(1):36-44. [DOI:10.1111/j.1601-6343.2007.00380.x] [PMID]
4. Sümbüllü MA, Cağlayan F, Akgül HM, Yilmaz AB. Radiological examination of the articular eminence morphology using cone beam CT. Dentomaxillofac Radiol. 2012 Mar;41(3):234-40 [DOI:10.1259/dmfr/24780643] [PMID] [PMCID]
5. Hemke R, van Veenendaal M, van den Berg JM, Dolman KM, van Rossum MA, Maas M, et al. One-year followup study on clinical findings and changes in magnetic resonance imaging-based disease activity scores in juvenile idiopathic arthritis. J Rheumatol. 2014 Jan;41(1):119-27. [DOI:10.3899/jrheum.130235] [PMID]
6. Ozkan A, Altug HA, Sencimen M, Senel B. Evaluation of articular eminence morphology and inclination in TMJ internal derangement patients with MRI. Int J Morphol. 2012;30(2):740-4. [DOI:10.4067/S0717-95022012000200064]
7. Hegde S, Praveen B, Shetty S. Morphological and radiological variations of mandibular condyles in health and diseases: a systematic review. Dentistry. 2013;3(1):154. [DOI:10.4172/2161-1122.1000154]
8. Karakas S, Tellioglu AM, Bilgin M, Omurlu IK, Caliskan S, Coskun S. Craniofacial Characteristics of Thalassemia Major Patients. Eur J Med. 2016 Oct;48(3):204-8. [DOI:10.5152/eurasianjmed.2016.150013] [PMID] [PMCID]
9. Girinath P, Vahanwala SP, Krishnamurthy V, Pagare SS. Evaluation of Orofacial Manifestations in 50 Thalassemic Patients: A Clinical Study. J Indian Acad Oral Med Radiol. 2010;22(3):126-32. [DOI:10.5005/jp-journals-10011-1030]
10. Toman HA, Nasir A, Hassan R, Hassan R. Skeletal, dentoalveolar, and soft tissue cephalometric measurements of Malay transfusion-dependent thalassaemia patients. Eur J Orthod. 2011;33(6):700-4. [DOI:10.1093/ejo/cjq147] [PMID]
11. Uysal A, Genc A, Taşyürek N, Türkyilmaz B. Prevalence of β-thalassemia trait and abnormal hemoglobin in premarital screening in the Province of Izmir, Turkey. Pediatr Hematol Oncol. 2013 Feb;30(1):46-50. [DOI:10.3109/08880018.2012.742604] [PMID]
12. Kim JH, Kim YK, Kim SG, Yun PY, Kim JD, Min JH. Effectiveness of bone scans in the diagnosis of osteoarthritis of the temporomandibular joint. Dentomaxillofac Radiol. 2012 Mar;41(3):224-9. [DOI:10.1259/dmfr/83814366] [PMID] [PMCID]
13. Choi BH, Yoon SH, Song SI, Yoon JK, Lee SJ, An YS. Comparison of diagnostic performance between visual and quantitative assessment of bone scintigraphy results in patients with painful temporomandibular disorder. Medicine (Baltimore). 2016 Jan;95(2):e2485. [DOI:10.1097/MD.0000000000002485] [PMID] [PMCID]
14. Moshfeghi M, Amin Tavakoli M, Razaghi Kashani Z, Rafieian N. Abnormal Temporomandibular Joint radiographic findings in patients referred to Department of Oral and Maxillofacial Radiology, Dental School, Shahid Beheshti University of Medical Sciences. J Dent Sch. 2012;29(5):381-9.
15. Brooks SL, Westesson PL, Eriksson L, Hansson LG, Barsotti JB. Prevalence of osseous changes in the temporomandibular joint of asymptomatic persons without internal derangement. Oral Surg Oral Med Oral Pathol Oral Radiol. 1992 Jan;73(1):118-22. [DOI:10.1016/0030-4220(92)90168-P]
16. Katzberg RW, Westesson PL, Tallents RH, Drake CM. Anatomic disorders of the temporomandibular joint disc in asymptomatic subjects. J Oral Maxillofac Surg. 1996 Feb;54(2):147-53. [DOI:10.1016/S0278-2391(96)90435-8]
17. Padala S, Padmanabhan S, Chithranjan AB. Comparative evaluation of condylar position in symptomatic (TMJ dysfunction) and asymptomatic individuals. Indian J Dent Res. 2012 Jan-Feb;23(1):122. [DOI:10.4103/0970-9290.99060] [PMID]
18. Caffey J. Cooley's anemia: a review of the roentgenographic findings in the skeleton: Hickey lecture, 1957. Am J Roentgenol Radium Ther Nucl Med. 1957 Sep;78(3):381-91.
19. Drew SJ, Sachs SA. Management of the thalassemia-induced skeletal facial deformity: case reports and review of the literature. J Oral Maxillofac Surg. 1 1997 Nov;55(11):1331-9. [DOI:10.1016/S0278-2391(97)90197-X]
20. Abu Alhaija ES, Hattab FN, al-Omari MA. Cephalometric measurements and facial deformities in subjects with β‐thalassaemia major. Eur J Orthod. 2002 Feb;24(1):9-19. [DOI:10.1093/ejo/24.1.9] [PMID]
21. Takriti M, Dashash M. Craniofacial parameters of Syrian children with β‐thalassemia major. J Investig Clin Dent. 2011 May;2(2):135-43. [DOI:10.1111/j.2041-1626.2010.00042.x] [PMID]
22. Langhi D Jr, Ubiali EM, Marques JF Jr, Verissimo MA, Loggetto SR, Silvinato A, et al. Guidelines on Beta-thalassemia major - regular blood transfusion therapy: Associação Brasileira de Hematologia, Hemoterapia e Terapia Celular: project guidelines: Associação Médica Brasileira - 2016. Rev Bras Hematol Hemoter. 2016 Oct-Dec;38(4):341-5. [DOI:10.1016/j.bjhh.2016.09.003] [PMID] [PMCID]
23. Cappellini MD, Cohen A, Porter J, Taher A, Viprakasit V. Guidelines for the Management of Transfusion Dependent Thalassaemia (TDT) [Internet]. 3rd edition. Nicosia (CY): Thalassaemia International Federation; 2014.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
