

Volume 2, Issue 4 (10-2017)
J Res Dent Maxillofac Sci 2017, 2(4): 14-19 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
MalekiGorji M, Banava S, Saghiri M. Enamel Erosion by 15% and 18% Hydrochloric Acid Gels after Different Application Times. J Res Dent Maxillofac Sci 2017; 2 (4) :14-19
URL: http://jrdms.dentaliau.ac.ir/article-1-185-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-185-en.html


1- Postgraduate Student, Oral & Maxillofacial surgery Dept, dental school, , mohsen_malekigorji@yahoo.com
2- Assistant Professor, Department of operative & Restorative Dentistry and Dental Materials,
3- Assistant Professor, Department of Ophthalmology & Visual Sciences,
2- Assistant Professor, Department of operative & Restorative Dentistry and Dental Materials,
3- Assistant Professor, Department of Ophthalmology & Visual Sciences,
Full-Text [PDF 351 kb]
(1802 Downloads)
| Abstract (HTML) (4670 Views)
Abstract
Background and Aim: Discolored teeth are among the most common reasons behind seeking esthetic dental treatments. Resin infiltration is a new technique for treatment of white spot lesions (WSLs). In this technique, 15% hydrochloric acid (HCl) is used to cause surface erosion. The aim of this study was to compare the enamel erosion caused by 15% and 18% HCl gels after different application times.
Materials and Methods: In this experimental study, sixty sound enamel surfaces were randomly divided into six groups of 10 (G1-G6). G1 specimens were subjected to 15% HCl gel for 75 seconds. G2 and G3 samples were subjected to 15% HCl for 90 and 120 seconds, respectively. G4, G5, and G6 specimens were subjected to 18% HCl for 75, 90, and 120 seconds, respectively. The specimens were then evaluated under a scanning electron microscope (SEM), and the depth of erosion was recorded. Data were analyzed by using one-way analysis of variance (ANOVA) and Tukey’s post-hoc test with a 95% confidence interval.
Results: The depth of erosion in 18% HCl groups was greater than that in 15% HCl groups after the same application times (P<0.05). The depth of erosion was not significantly different between G3 and G4 samples (P>0.05).
Conclusion: The results of this study showed that the application of 18% HCl for 75 seconds is a suitable alternative to the application of 15% HCl for 120 seconds in the resin infiltration technique.
Key words: Enamel Microabrasion, Hydrochloric Acid, Tooth Erosion, Scanning Electron Microscopy
Introduction
Esthetic dental treatments are among the most common reasons of dental visits. (1) Many patients seek esthetic dental treatments for discolored teeth since tooth discoloration may negatively affect their confidence and the quality of life. (1-3)
Enamel microabrasion is a commonly used technique for the complete resolution or improvement of superficial tooth discolorations. (4) McCloskey was the first to report the resolution of superficial discolorations due to fluorosis after rubbing 18% hydrochloric acid (HCl) on the tooth surface. (5) Ted Croll modified this technique and used a mixture of pumice powder and HCl, and called it microabrasion. (6) In enamel microabrasion, the enamel surface is dissolved by acid, and superficial stains and impurities are removed by abrasive pumice powder. Over time, Croll made some other modifications to this technique, and decreased the concentration of acid to 11%. He also increased the abrasiveness of pumice by adding silicon carbide particles. (7)
In 2005, the resin infiltration technique was introduced by Paris and Meyer to prevent the progression of white spot lesions (WSLs). In this technique, 15% HCl is used for 120 seconds to cause superficial erosion, and then, a hydrophobic infiltrant resin with a high penetration coefficient is applied to the surface in order to seal the eroded area. (8,9-17) Several studies have assessed the efficacy of this method for treatment of tooth discoloration. (10-12,16) Gugnani et al demonstrated the success of treatment of WSLs and fluorosed teeth with the resin infiltration technique. (10) Munoz et al also showed that the resin infiltration technique could be used as a minimally invasive technique for treatment of tooth discoloration due to mild-moderate fluorosis and hypoplasia. (11) Resin infiltration is a more effective treatment for masking WSLs in comparison with traditional fluoride treatments. The effect of masking of WSLs has certain correlations with the degree of demineralization and the activity of the lesion. (18)
Considering the high cost of 15% HCl (Icon-Etch®, DMG, USA) and its scarcity in Iran as well as the availability of 18% HCl (domestically manufactured by Kimia, Iran), we sought to compare the enamel erosion following the application of 15% and 18% HCl gels after different application times.
Materials and Methods
In this experimental study, 60 extracted human anterior teeth were collected and cleaned from debris and soft tissue residues by using gauze and #12 surgical scalpel (3M Health Care, Pakistan). The teeth were extracted because of severe periodontal diseases. The soundness of the enamel was ensured microscopically (Stemi SV 11; Carl Zeiss, Oberkochen, Germany), and the teeth were evaluated at ×30 magnification for the absence of cracks, caries, and hypocalcification. The teeth were immersed in 0.2% thymol solution for 48 hours, and were then transferred to distilled water. The roots were cut at the cementoenamel junction (CEJ) by using a diamond disc (D&Z, Germany) and a high-speed handpiece. Buccal surfaces of the teeth were evaluated in terms of smoothness, and 60 enamel surfaces measuring 3×3 mm were cut out. The specimens were coded and divided into six groups of 10 (G1-G6) by simple randomization:
G1: Buccal surfaces of the specimens were subjected to 15% HCl gel (Icon-Etch®, DMG, USA) for 75 seconds according to the manufacturer’s instructions. The specimens were then rinsed with water spray for 30 seconds and were air-dried by using an air spray.
G2: The enamel specimens in this group were subjected to 15% HCl gel for 90 seconds according to the manufacturer’s instructions.
G3: The enamel specimens in this group were subjected to 15% HCl gel for 120 seconds according to the manufacturer’s instructions.
G4: The enamel specimens in this group were subjected to 18% HCl gel (Kimia, Iran) for 75 seconds according to the manufacturer’s instructions.
G5: The enamel specimens in this group were subjected to 18% HCl gel for 90 seconds according to the manufacturer’s instructions.
G6: The enamel specimens in this group were subjected to 18% HCl gel for 120 seconds according to the manufacturer’s instructions.
The specimens in G2-G6 were washed and dried following the application of the acidic gels the same as in G1.
After the acid application process, the specimens were gold coated and were evaluated under a scanning electron microscope (SEM; VEGA II, TESCAN, 510-SEM-01, Czech Republic). The depth of enamel erosion was recorded in microns (μm), and the mean depth of enamel erosion in each group was calculated.
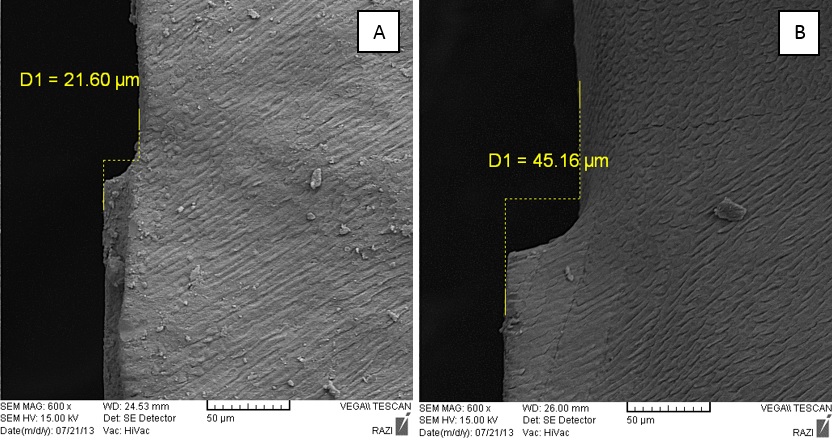
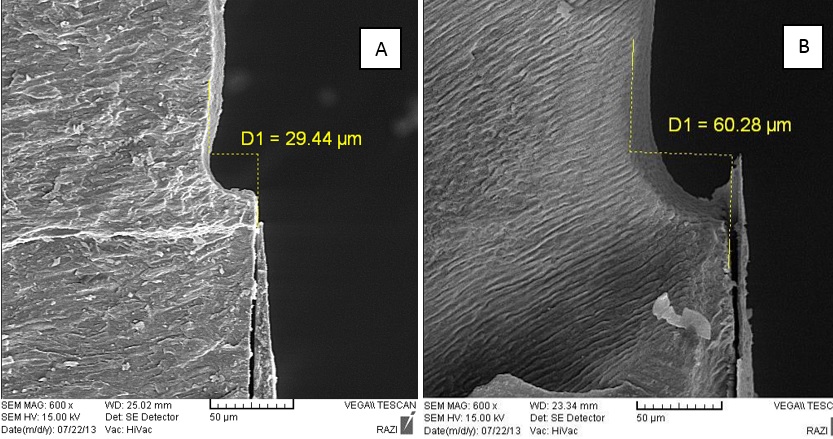
Figures 1 and 2 show the erosion depth following the application of the two acids for 90 and 120 seconds. The depth of erosion was measured by estimating the distance between two parallel lines, namely the sound enamel surface and the etched surface. The distance between the mentioned two parallel lines was measured by using a computer software (VEGA II, TESCAN, 510-SEM-01, Czech Republic).
Data were analyzed by using SPSS 23 software (IBM Co., Chicago, IL, USA) and by one-way analysis of variance (ANOVA) and Tukey’s post-hoc honest significant difference (HSD) test with a 95% confidence interval.
Figure 1: SEM micrographs showing the depth (µm) of erosion. (A): 15% HCl/90 seconds. (B): 18% HCl/90 seconds
Figure 2: SEM micrographs showing the depth (µm) of erosion. (A): 15% HCl/120 seconds. (B): 18% HCl/120 seconds
Results
The mean and standard deviation (SD) of the erosion depth in G1, G2, and G3 were 22.88±1.95µm, 27.01±4.35µm, and 33.65±7.94µm, respectively, while the mean and SD of the erosion depth in G4, G5, and G6 were 31.44±2.56µm, 49.49±17.83µm, and 54.17±11.31µm, respectively. The ANOVA showed that the depths of erosion in G1, G2, and G3 were significantly different (P=0.03); it also showed that the depths of erosion in G4, G5, and G6 were significantly different (P=0.03).
The Tukey’s post-hoc HSD test showed that the erosion depth in 18% HCl groups was greater than that in 15% HCl groups after the same application times (P=0.005). The greatest depth of erosion was 54.17µm, and it was seen in G6 (18% HCl, 120 seconds).
The erosion depths in the application of 15% HCl for 120 seconds (G3) and 18% HCl for 75 seconds (G4) had no significant difference (P=0.09; Table 1).
The application of 18% HCl for 75 seconds caused less erosion than the application of 18% HCl for 90 and 120 seconds (P=0.03). The application of 15% HCl for 75 seconds caused less erosion than the use of 15% HCl for 90 and 120 seconds (P=0.03).
Figure 3 shows the depth of enamel erosion in the six groups.
In the current study, the pattern of etching was also evaluated in addition to the measurement of the depth of erosion caused by the acids. Figure 4 shows the etching pattern caused by the two acids after 90 seconds of application. The etched pattern caused by 18% HCl was more prominent than that caused by 15% HCl with the same application times. Enamel removal by 15% HCl was more uniform and regular and resulted in less erosion, while 18% HCl caused a non-homogenous and irregular enamel etching, and the demineralization was greater around enamel rods, and consequently, the erosion was deeper.
Table 1: Mean and standard deviation (SD) of the depth (µm) of surface erosion in the six groups
Figure 3: Mean and standard deviation (SD) of the erosion depth (µm) in the six groups, CI=Confidence interval
Figure 4: SEM micrographs showing the pattern of erosion. (A): 15% HCl/90 seconds. (B): 18% HCl/90 seconds.
Discussion
This study assessed the enamel erosion caused by 15% and 18% HCl gels after different application times and showed that 18% HCl applied for 75 seconds had an effect similar to that of 15% HCl applied for 120 seconds, and that these two gels were not significantly different in terms of the efficacy for enamel erosion after the mentioned application periods. Thus, the application of domestically manufactured 18% HCl for 75 seconds is a suitable alternative to the application of 15% HCl in the resin infiltration technique.
Esthetic treatment of discolored teeth is among the most common reasons of dental visits. (1-3) The final goal of treatment of tooth discoloration is to yield an acceptable esthetic result by using a conservative method. (11) Enamel microabrasion is the most commonly used and the most conservative technique for treatment of tooth discoloration due to fluorosis, hypoplasia, hypocalcification, and post-orthodontic decalcifications. (19,20) This method was first used for removal of discoloration caused by fluorosis. This method is much more conservative than the use of composite veneers and ceramics. (5) Mechanical and chemical techniques are combined in enamel microabrasion. An abrasive acidic substance in the form of a thick paste is applied to the buccal surface of the discolored tooth. The removal of a thin layer of enamel by the dissolution of minerals is known as enamel erosion. Since it is sometimes necessary to place this paste on the tooth surface several times to completely remove the color change, It is not known for how many times this process can be repeated before causing dentin exposure, and no consensus has been reached in this regard. Many clinicians do not feel comfortable using this technique. (11) On the other hand, after microabrasion, the tooth surface is polished and left uncovered without applying any other substance; this can result in the development of WSLs which give an opaque appearance to the tooth. (7)
Many studies have evaluated the efficacy of the resin infiltration technique for ceasing incipient caries. (21-24) In this technique, a resin infiltrant with a high penetration capacity and a low viscosity is applied, which penetrates into the areas etched with 15% HCl. (13) One advantage of this technique is that the resin penetrates into enamel microporosities and fills them; consequently, the enamel surface would no longer have the chalky white appearance, and it resembles sound enamel. Thus, based on the literature, this technique can improve the appearance of WSLs on buccal surfaces. (10,11,14-15) It is still a matter of debate that whether or not large lesions are infiltrated completely. (21,23,25) Several factors can influence this matter, such as surface porosity, the porosity of the body of the lesion, dryness of the lesion, and capillary forces. (25)
Munoz et al and Kim et al showed that the resin infiltration technique was efficient for mildly and moderately fluorosed teeth as well as for tooth discolorations due to enamel hypoplasia. (11,15)
The current study was the first to use sound teeth for the measurement of the enamel erosion caused by acids. Due to the higher concentration of the domestically made acid, the enamel erosion caused by this acid was greater than that in 15% HCl groups. Also, the mean and SD of the depth of the enamel erosion caused by 15% HCl applied for 120 seconds in our study was less than that reported by Paris et al (33.65±7.94µm in our study versus 58±37µm in the study by Paris et al). (24) The greater depth of erosion due to the application of 15% HCl for 120 seconds in the study by Paris et al may be due to the use of carious teeth since they were already demineralized and had less mineral content. (24)
In the study by Paris et al in 2007, the penetration depth of an adhesive was measured to assess the depth of erosion caused by acids. (9) However, this method decreases the accuracy of measurement because the penetration depth of resin is influenced by factors such as the penetration ability of resin. In our study, the depth of erosion caused by the acidic gels was measured directly without the application of an adhesive, which is more accurate, since in this method, the measurement of the erosion depth is not affected by resin properties.
The methodology of our study was somehow similar to that of the study by Paris et al in 2007. (9) The only difference was that we used sound teeth, while they used carious teeth. Moreover, instead of confocal microscopy, we used SEM which can more accurately show the pattern of etching.
In our study, the erosion depth in 15% HCl groups had a significantly higher predictability and a limited distribution; 18% HCl yielded a more irregular etching pattern compared to 15% HCl. The composition of acid, the additives, and the pH may also play a role in this regard; thus, future studies are required in this respect. The results showed that for the treatment of discolorations of labial surfaces of anterior teeth by using the resin infiltration technique, 18% HCl for 75 seconds may be used instead of 15% HCl for 120 seconds. Consequently, the cost of treatment, which is the main factor limiting the application of this technique and negatively affecting the patient's acceptance, is reduced. The use of 18% HCl for 75 seconds is cost effective and timesaving. A shorter application time results in an easier handling while decreasing the risk of chemical burn of oral mucosa caused by acid. Comparing the effect of resins other than an infiltrant resin with that of the domestically made 18% HCl is recommended in future studies.
Conclusions
The results of this experimental study revealed that the application of 18% HCl for 75 seconds has the same effects as the application of 15% HCl for 120 seconds. Therefore, the use of 18% HCl for 75 seconds can be a good alternative to the use of 15% HCl in the resin infiltration technique.
Full-Text: (851 Views)
Abstract
Background and Aim: Discolored teeth are among the most common reasons behind seeking esthetic dental treatments. Resin infiltration is a new technique for treatment of white spot lesions (WSLs). In this technique, 15% hydrochloric acid (HCl) is used to cause surface erosion. The aim of this study was to compare the enamel erosion caused by 15% and 18% HCl gels after different application times.
Materials and Methods: In this experimental study, sixty sound enamel surfaces were randomly divided into six groups of 10 (G1-G6). G1 specimens were subjected to 15% HCl gel for 75 seconds. G2 and G3 samples were subjected to 15% HCl for 90 and 120 seconds, respectively. G4, G5, and G6 specimens were subjected to 18% HCl for 75, 90, and 120 seconds, respectively. The specimens were then evaluated under a scanning electron microscope (SEM), and the depth of erosion was recorded. Data were analyzed by using one-way analysis of variance (ANOVA) and Tukey’s post-hoc test with a 95% confidence interval.
Results: The depth of erosion in 18% HCl groups was greater than that in 15% HCl groups after the same application times (P<0.05). The depth of erosion was not significantly different between G3 and G4 samples (P>0.05).
Conclusion: The results of this study showed that the application of 18% HCl for 75 seconds is a suitable alternative to the application of 15% HCl for 120 seconds in the resin infiltration technique.
Key words: Enamel Microabrasion, Hydrochloric Acid, Tooth Erosion, Scanning Electron Microscopy
Introduction
Esthetic dental treatments are among the most common reasons of dental visits. (1) Many patients seek esthetic dental treatments for discolored teeth since tooth discoloration may negatively affect their confidence and the quality of life. (1-3)
Enamel microabrasion is a commonly used technique for the complete resolution or improvement of superficial tooth discolorations. (4) McCloskey was the first to report the resolution of superficial discolorations due to fluorosis after rubbing 18% hydrochloric acid (HCl) on the tooth surface. (5) Ted Croll modified this technique and used a mixture of pumice powder and HCl, and called it microabrasion. (6) In enamel microabrasion, the enamel surface is dissolved by acid, and superficial stains and impurities are removed by abrasive pumice powder. Over time, Croll made some other modifications to this technique, and decreased the concentration of acid to 11%. He also increased the abrasiveness of pumice by adding silicon carbide particles. (7)
In 2005, the resin infiltration technique was introduced by Paris and Meyer to prevent the progression of white spot lesions (WSLs). In this technique, 15% HCl is used for 120 seconds to cause superficial erosion, and then, a hydrophobic infiltrant resin with a high penetration coefficient is applied to the surface in order to seal the eroded area. (8,9-17) Several studies have assessed the efficacy of this method for treatment of tooth discoloration. (10-12,16) Gugnani et al demonstrated the success of treatment of WSLs and fluorosed teeth with the resin infiltration technique. (10) Munoz et al also showed that the resin infiltration technique could be used as a minimally invasive technique for treatment of tooth discoloration due to mild-moderate fluorosis and hypoplasia. (11) Resin infiltration is a more effective treatment for masking WSLs in comparison with traditional fluoride treatments. The effect of masking of WSLs has certain correlations with the degree of demineralization and the activity of the lesion. (18)
Considering the high cost of 15% HCl (Icon-Etch®, DMG, USA) and its scarcity in Iran as well as the availability of 18% HCl (domestically manufactured by Kimia, Iran), we sought to compare the enamel erosion following the application of 15% and 18% HCl gels after different application times.
Materials and Methods
In this experimental study, 60 extracted human anterior teeth were collected and cleaned from debris and soft tissue residues by using gauze and #12 surgical scalpel (3M Health Care, Pakistan). The teeth were extracted because of severe periodontal diseases. The soundness of the enamel was ensured microscopically (Stemi SV 11; Carl Zeiss, Oberkochen, Germany), and the teeth were evaluated at ×30 magnification for the absence of cracks, caries, and hypocalcification. The teeth were immersed in 0.2% thymol solution for 48 hours, and were then transferred to distilled water. The roots were cut at the cementoenamel junction (CEJ) by using a diamond disc (D&Z, Germany) and a high-speed handpiece. Buccal surfaces of the teeth were evaluated in terms of smoothness, and 60 enamel surfaces measuring 3×3 mm were cut out. The specimens were coded and divided into six groups of 10 (G1-G6) by simple randomization:
G1: Buccal surfaces of the specimens were subjected to 15% HCl gel (Icon-Etch®, DMG, USA) for 75 seconds according to the manufacturer’s instructions. The specimens were then rinsed with water spray for 30 seconds and were air-dried by using an air spray.
G2: The enamel specimens in this group were subjected to 15% HCl gel for 90 seconds according to the manufacturer’s instructions.
G3: The enamel specimens in this group were subjected to 15% HCl gel for 120 seconds according to the manufacturer’s instructions.
G4: The enamel specimens in this group were subjected to 18% HCl gel (Kimia, Iran) for 75 seconds according to the manufacturer’s instructions.
G5: The enamel specimens in this group were subjected to 18% HCl gel for 90 seconds according to the manufacturer’s instructions.
G6: The enamel specimens in this group were subjected to 18% HCl gel for 120 seconds according to the manufacturer’s instructions.
The specimens in G2-G6 were washed and dried following the application of the acidic gels the same as in G1.
After the acid application process, the specimens were gold coated and were evaluated under a scanning electron microscope (SEM; VEGA II, TESCAN, 510-SEM-01, Czech Republic). The depth of enamel erosion was recorded in microns (μm), and the mean depth of enamel erosion in each group was calculated.
Figures 1 and 2 show the erosion depth following the application of the two acids for 90 and 120 seconds. The depth of erosion was measured by estimating the distance between two parallel lines, namely the sound enamel surface and the etched surface. The distance between the mentioned two parallel lines was measured by using a computer software (VEGA II, TESCAN, 510-SEM-01, Czech Republic).
Data were analyzed by using SPSS 23 software (IBM Co., Chicago, IL, USA) and by one-way analysis of variance (ANOVA) and Tukey’s post-hoc honest significant difference (HSD) test with a 95% confidence interval.
Figure 1: SEM micrographs showing the depth (µm) of erosion. (A): 15% HCl/90 seconds. (B): 18% HCl/90 seconds
{kind=link}
Figure 2: SEM micrographs showing the depth (µm) of erosion. (A): 15% HCl/120 seconds. (B): 18% HCl/120 seconds
{kind=link}
Results
The mean and standard deviation (SD) of the erosion depth in G1, G2, and G3 were 22.88±1.95µm, 27.01±4.35µm, and 33.65±7.94µm, respectively, while the mean and SD of the erosion depth in G4, G5, and G6 were 31.44±2.56µm, 49.49±17.83µm, and 54.17±11.31µm, respectively. The ANOVA showed that the depths of erosion in G1, G2, and G3 were significantly different (P=0.03); it also showed that the depths of erosion in G4, G5, and G6 were significantly different (P=0.03).
The Tukey’s post-hoc HSD test showed that the erosion depth in 18% HCl groups was greater than that in 15% HCl groups after the same application times (P=0.005). The greatest depth of erosion was 54.17µm, and it was seen in G6 (18% HCl, 120 seconds).
The erosion depths in the application of 15% HCl for 120 seconds (G3) and 18% HCl for 75 seconds (G4) had no significant difference (P=0.09; Table 1).
The application of 18% HCl for 75 seconds caused less erosion than the application of 18% HCl for 90 and 120 seconds (P=0.03). The application of 15% HCl for 75 seconds caused less erosion than the use of 15% HCl for 90 and 120 seconds (P=0.03).
Figure 3 shows the depth of enamel erosion in the six groups.
In the current study, the pattern of etching was also evaluated in addition to the measurement of the depth of erosion caused by the acids. Figure 4 shows the etching pattern caused by the two acids after 90 seconds of application. The etched pattern caused by 18% HCl was more prominent than that caused by 15% HCl with the same application times. Enamel removal by 15% HCl was more uniform and regular and resulted in less erosion, while 18% HCl caused a non-homogenous and irregular enamel etching, and the demineralization was greater around enamel rods, and consequently, the erosion was deeper.
Table 1: Mean and standard deviation (SD) of the depth (µm) of surface erosion in the six groups
{kind=link}
Figure 3: Mean and standard deviation (SD) of the erosion depth (µm) in the six groups, CI=Confidence interval
{kind=link}
Figure 4: SEM micrographs showing the pattern of erosion. (A): 15% HCl/90 seconds. (B): 18% HCl/90 seconds.
{kind=link}
Discussion
This study assessed the enamel erosion caused by 15% and 18% HCl gels after different application times and showed that 18% HCl applied for 75 seconds had an effect similar to that of 15% HCl applied for 120 seconds, and that these two gels were not significantly different in terms of the efficacy for enamel erosion after the mentioned application periods. Thus, the application of domestically manufactured 18% HCl for 75 seconds is a suitable alternative to the application of 15% HCl in the resin infiltration technique.
Esthetic treatment of discolored teeth is among the most common reasons of dental visits. (1-3) The final goal of treatment of tooth discoloration is to yield an acceptable esthetic result by using a conservative method. (11) Enamel microabrasion is the most commonly used and the most conservative technique for treatment of tooth discoloration due to fluorosis, hypoplasia, hypocalcification, and post-orthodontic decalcifications. (19,20) This method was first used for removal of discoloration caused by fluorosis. This method is much more conservative than the use of composite veneers and ceramics. (5) Mechanical and chemical techniques are combined in enamel microabrasion. An abrasive acidic substance in the form of a thick paste is applied to the buccal surface of the discolored tooth. The removal of a thin layer of enamel by the dissolution of minerals is known as enamel erosion. Since it is sometimes necessary to place this paste on the tooth surface several times to completely remove the color change, It is not known for how many times this process can be repeated before causing dentin exposure, and no consensus has been reached in this regard. Many clinicians do not feel comfortable using this technique. (11) On the other hand, after microabrasion, the tooth surface is polished and left uncovered without applying any other substance; this can result in the development of WSLs which give an opaque appearance to the tooth. (7)
Many studies have evaluated the efficacy of the resin infiltration technique for ceasing incipient caries. (21-24) In this technique, a resin infiltrant with a high penetration capacity and a low viscosity is applied, which penetrates into the areas etched with 15% HCl. (13) One advantage of this technique is that the resin penetrates into enamel microporosities and fills them; consequently, the enamel surface would no longer have the chalky white appearance, and it resembles sound enamel. Thus, based on the literature, this technique can improve the appearance of WSLs on buccal surfaces. (10,11,14-15) It is still a matter of debate that whether or not large lesions are infiltrated completely. (21,23,25) Several factors can influence this matter, such as surface porosity, the porosity of the body of the lesion, dryness of the lesion, and capillary forces. (25)
Munoz et al and Kim et al showed that the resin infiltration technique was efficient for mildly and moderately fluorosed teeth as well as for tooth discolorations due to enamel hypoplasia. (11,15)
The current study was the first to use sound teeth for the measurement of the enamel erosion caused by acids. Due to the higher concentration of the domestically made acid, the enamel erosion caused by this acid was greater than that in 15% HCl groups. Also, the mean and SD of the depth of the enamel erosion caused by 15% HCl applied for 120 seconds in our study was less than that reported by Paris et al (33.65±7.94µm in our study versus 58±37µm in the study by Paris et al). (24) The greater depth of erosion due to the application of 15% HCl for 120 seconds in the study by Paris et al may be due to the use of carious teeth since they were already demineralized and had less mineral content. (24)
In the study by Paris et al in 2007, the penetration depth of an adhesive was measured to assess the depth of erosion caused by acids. (9) However, this method decreases the accuracy of measurement because the penetration depth of resin is influenced by factors such as the penetration ability of resin. In our study, the depth of erosion caused by the acidic gels was measured directly without the application of an adhesive, which is more accurate, since in this method, the measurement of the erosion depth is not affected by resin properties.
The methodology of our study was somehow similar to that of the study by Paris et al in 2007. (9) The only difference was that we used sound teeth, while they used carious teeth. Moreover, instead of confocal microscopy, we used SEM which can more accurately show the pattern of etching.
In our study, the erosion depth in 15% HCl groups had a significantly higher predictability and a limited distribution; 18% HCl yielded a more irregular etching pattern compared to 15% HCl. The composition of acid, the additives, and the pH may also play a role in this regard; thus, future studies are required in this respect. The results showed that for the treatment of discolorations of labial surfaces of anterior teeth by using the resin infiltration technique, 18% HCl for 75 seconds may be used instead of 15% HCl for 120 seconds. Consequently, the cost of treatment, which is the main factor limiting the application of this technique and negatively affecting the patient's acceptance, is reduced. The use of 18% HCl for 75 seconds is cost effective and timesaving. A shorter application time results in an easier handling while decreasing the risk of chemical burn of oral mucosa caused by acid. Comparing the effect of resins other than an infiltrant resin with that of the domestically made 18% HCl is recommended in future studies.
Conclusions
The results of this experimental study revealed that the application of 18% HCl for 75 seconds has the same effects as the application of 15% HCl for 120 seconds. Therefore, the use of 18% HCl for 75 seconds can be a good alternative to the use of 15% HCl in the resin infiltration technique.
Type of Study: Original article |
Subject:
Oral & maxillofacial surgery
References
1. Carey CM. Tooth whitening: what we now know. J Evid Based Dent Pract. 2014 Jun; 14 Suppl:70–6.
2. Ibiyemi O, Taiwo JO. Psychosocial Aspect of Anterior Tooth Discoloration among Adolescents in Igbo-ora, Southwestern Nigeria. Ann Ib Postgrad Med. 2011 Dec;9(2):94-9..
3. Gbadebo SO, Ajayi DM. Self reported tooth discolorations among patients seen at dental center university college hospital Ibadan. J West Afr Coll Surg. 2015 Jul-Sep;5(3):66–77.
4. Shivanna V, Shivakumar B. Novel treatment of white spot lesions: A report of two cases. J Conserv Dent. 2011 Oct;14(4):423-6.
5. Ahmadi Zenouz G, Ezoji F, Enderami SA, Khafri S. Effect of fluoride, casein phosphopeptide-amorphous calcium phosphate and casein phosphopeptide-amorphous calcium phosphate fluoride on enamel surface microhardness after microabrasion: An in vitro study. J Dent (Tehran). 2015 Oct;12(10):705–11.
6. Pini NI, Sundfeld-Neto D, Aguiar FH, Sundfeld RH, Martins LR, Lovadino JR, et al. Enamel microabrasion: An overview of clinical and scientific considerations. World J Clin Cases. 2015 Jan 16;3(1):34–41.
7. Perete-de-Freitas CE, Silva PD, Faria-E-Silva AL. Impact of Microabrasion on the Effectiveness of Tooth Bleaching . Braz Dent J. 2017 Sep-Oct;28(5):612-617.
8. Meyer-Lueckel H, Paris S. Improved resin infiltration of natural caries lesion. J Dent Res. 2008 Dec;87(12):1112–6.
9. Paris S, Meyer-Lueckel H, Kielbessa AM. Resin infiltration of natural caries lesion. J Dent Res 2007;86(7):662–6
10. Gugnani N, Pandit IK, Gupta M, Gugnani S, Soni S, Goyal V. Comparative evaluation of esthetic changes in nonpitted fluorosis stains when treated with resin infiltration, in-office bleaching, and combination therapies. J Esthet Restor Dent. 2017 Sep;29(5):317-4.
11. Muñoz MA, Arana-Gordillo LA, Gomes GM, Gomes OM, Bombarda NH, Reis A, et al. Loguercio AD. Alternative esthetic management of fluorosis and hypoplasia stains: blending effect obtained with resin infiltration techniques. J Esthet Restor Dent. 2013 Feb;25(1):32-9.
12. Crombie F, Manton D, Palamara J, Reynolds E. Resin infiltration of developmentally hypomineralised enamel. Int J Paediatr Dent. 2014 Jan;24(1):51-5.
13. Swamy DF, Barretto ES, Mallikarjun SB, Dessai SSR. In vitro Evaluation of Resin Infiltrant Penetration into White Spot Lesions of Deciduous Molars. J Clin Diagn Res.2017 Sep;11(9):ZC71-ZC74.
14. Paris S, Meyer-Lueckel H. Masking of labial enamel white spot lesions by resin infiltration -a Clinical report. Quintessence Int. 2009 Oct;40(9):713–8.
15. Kim S, Kim EY, Jeong TS, Kim JW. The evaluation of resin infiltration for masking labial enamel white spot lesions. Int J Paediatr Dent. 2011 Jul;21(4):241-8.
16. Perdigao J, Lam VQ, Burseth BG, Real C. Masking of enamel Fluorosis Discolorations and Tooth Misalignment With a Combination of At-Home Whitening, Resin Infiltration, and Direct Composite Restorations. Oper Dent. 2017 Jul/Aug;42(4):347-56.
17. Yetkiner E, Wegehaupt F, Wiegand A, Attin R, Attin T. Colour improvement and stability of white spot lesions following infiltration, micro-abrasion, or fluoride treatments in vitro. Eur J Orthod. 2014 Oct;36(5):595–602.
18. Zhao X, Gao X. Effect of resin infiltration treatment on the colour of white spot lesions. Hua Xi Kou Qiang Yi Xue Za Zhi. 2014 Jun;32(3):306-9.
19. Yim H K, Min J H, Kwon H K, and Kim B I. Modification of surface pretreatment of white spot lesions to improve the safety and efficacy of resin infiltration. Korean J Orthod. 2014 Jul; 44(4): 195–202.
20. Sundfeld RH, Croll TP, Briso AL, de Alexandre RS, Sundfeld Neto D. Considerations about enamel microabrasion after 18 years. Am J Dent. 2007 Apr;20(2):67-72.
21. Paris S, Bitter K, Naumann M, Dorfer CE, Meyer-Lueckel H. Resin infiltration of proximal caries lesions differing in ICDAS codes. Eur J Oral Sci. 2011 Apr;119(2):182-6.
22. Paris S, Meyer-Lueckel H. Infiltrants inhibit progression of natural caries lesions in vitro. J Dent Res. 2010 Nov;89(11):1276-80.
23. Arnold WH, Gaengler P. Light- and electronmicroscopic study of infiltration of resin into initial caries lesions a new meth-odological approach. J Microsc. 2012 Jan;245(1):26-33.
24. Neuhaus KW, Schlafer S, Lussi A, Nyvad B. Infiltration of natural caries lesions in relation to their activity status and acid pretreatment in vitro. Caries Res. 2013;47(3):203–10.
25. Paris S, Soviero VM, Seddig S, Meyer- Lueckel H. Penetra-tion depths of an infiltrant into proximal caries lesions in primary molars after different application times in vitro. Int J Paediatr Dent. 2012 Sep;22(5):349-55.
26. Paris S, Meyer-Lueckel H, Colfen H, Kielbassa AM. Penetration coefficients of commercially available and experimental composites intended to infiltrate enamel carious lesions. Dent Mater. 2007 Jun;23(6):742-8.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
