Journal of Research in Dental
and Maxillofacial Sciences
Volume 1, Issue 4 (12-2016)
J Res Dent Maxillofac Sci 2016, 1(4): 9-15 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sakhdari S, JafariNaini A, kharazi M, Najafi N. Evaluating the Correlation between the Body Mass Index (BMI) and Dental Age in 6 to 13-Yyear-Old Children. J Res Dent Maxillofac Sci 2016; 1 (4) :9-15
URL: http://jrdms.dentaliau.ac.ir/article-1-139-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-139-en.html


1- Periodontics Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran.
2- Assistant Professor,Orthodontics Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran
3- Assistant Professor, Epidemiologist, Dental Research Center, Tehran University of Medical Sciences, Tehran, Iran
4- Post Graduate Student, Radiology Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran. ,Najafinaz@yahoo.com
2- Assistant Professor,Orthodontics Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran
3- Assistant Professor, Epidemiologist, Dental Research Center, Tehran University of Medical Sciences, Tehran, Iran
4- Post Graduate Student, Radiology Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran. ,
Full-Text [PDF 327 kb]
(2486 Downloads)
| Abstract (HTML) (6823 Views)
Abstract
Background and aim: Methods of age estimation with the aid of radiography have higher accuracy compared with other methods. Some investigations have been performed in this regard, but the correlation between dental development and Body Mass Index (BMI) has been limitedly researched. In the present study, the correlation between dental development and BMI in the children referring to the dental school of Islamic Azad University of Tehran was evaluated with the use of panoramic radiography.
Materials and methods: In this cross-sectional analysis, panoramic radiographs of 104 children aged 6 to 13 years were evaluated. The date of radiography minus the birth date was used to determine the chronologic age for each child and then, this age was compared with the dental age estimated by the Demirjian method. Afterwards, the height and weight of the children were measured and the BMI was calculated for each subject. The difference between the estimated dental age and the chronologic age of the subjects was analyzed according to gender and BMI classification. Statistical analyses were performed using the ANOVA test, Pearson correlation coefficient and linear regression.
Results: In the 104 samples, the difference between the estimated dental age and the chronologic age was not significant (p=0.516). The dental age in normal weight children was lower than the chronologic age while in obese children, it was higher than the chronologic age (p=0.00001). The correlation coefficient of the estimated dental age using the Demirjian method and the chronologic age in normal weight and obese boys was 0.936 and 0.901, respectively, while in normal weight and obese girls, it equaled 0.916 and 0.942, respectively.
Conclusion: The results of the present study showed that dental development is accelerated in obese children.
Keywords: panoramic radiography, body mass index, age, odontogenesis
Introduction
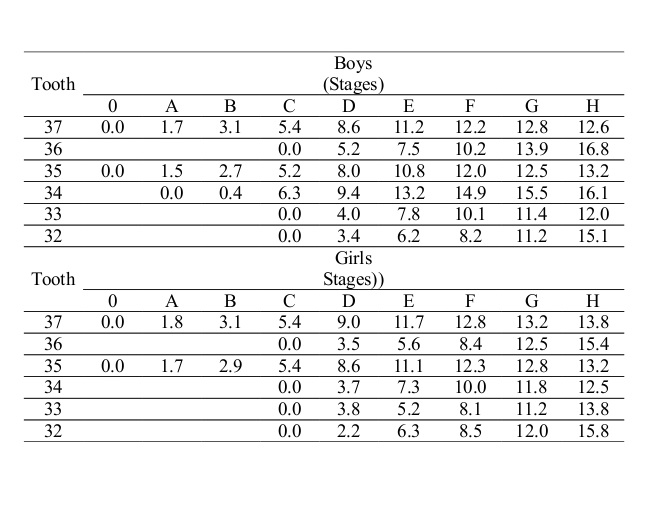
Childhood obesity is an increasing concern and is partly due to sedentary lifestyle and nutritional habits. In Iran, childhood obesity is following an ascending trend. In addition to diseases such as diabetes, high blood pressure and heart diseases, obesity causes accelerated growth and early puberty in girls. Obesity can alter the onset of puberty in boys. (1) Recent studies show that obese children experience faster craniofacial growth, and this accelerated development is an important variable in pediatric dental and orthodontic treatments. (2) Neoviou et al in 2004 found that children with high Body Mass Index (BMI) have more erupted teeth. (3) Evaluation of dental development with the use of radiography has a higher efficacy in the estimation of the chronologic age of children compared with other maturation indices. In addition, dental development is a biological index in growing children, mostly as an indicator of dental age. Dental age of children can be estimated based on tooth eruption or based on dental formation stages according to radiographic observations. (4,5) One of the methods for determining dental development according to radiography is the Demirjian method which was first introduced in 1973 following a study on a large sample of Canadian children, and it evaluates the development of seven perah on the left side of the mandible using panoramic radiographs. All the teeth are classified from A to H and from the stage of formation of the first calcified points to apex closure. (6,7)
The efficacy of the Demirjian method has been assessed among some of the ethnicities. (8-11) Also in previous studies, the correlation between dental development and height and weight has been evaluated, which was found to be a significant correlation in many studies. (12-16)
Considering the controversies among the results of the previous studies and also the gap of information regarding this matter in Iran, the present study aimed to evaluate the correlation between the BMI and dental development in the patients referring to the oral and maxillofacial radiology department of the dental school of Islamic Azad University of Tehran.
Materials and methods
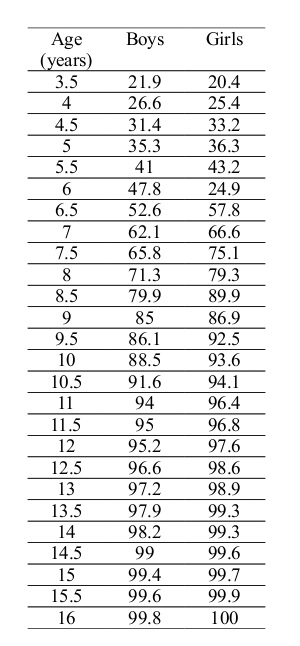
This cross-sectional analysis was performed on 104 children aged 6 to 13 years that referred for panoramic radiography. The 6 to 13-year-olds with seven permanent teeth (or tooth buds) on the left side of the mandible without any systemic or developmental diseases were included in the study. Radiographs of suitable quality were obtained as files from the radiology center and were saved in a laptop and the seven permanent teeth on the left side of the mandible were evaluated in each participant. All the dental buds pass different stages form the beginning of calcification to reach the final shape. (According to the Demirjian method). These stages are classified from A to H based on the stage of calcification. The stages of conversion of dental buds to the final form based on the degree of calcification include A: calcification at the tip of the cusps, B: connection of the calcified cusps, C: completion of enamel formation and beginning of dentin accumulation, D: completion of crown to the cemento-enamel junction (CEJ) area, E: parallel pulp chamber walls, root length less than coronal length, visible furcation, F: root length more than or equal to coronal length, funnel-shaped apex, G: parallel root walls and open apex, H: apex is closed and the periodontal ligament has a uniform width around the root. For each tooth, a numerical index was designated based on the determined developmental stage. With reference to table 1, this value was determined considering the gender of the subject. Indices for all the seven teeth were determined. The overall maturity score was obtained by summing up the seven indices, which ranged from 0 to 100. Then, with reference to table 2 the index was converted to dental age. (8,9) The chronologic age and the age calculated according to the Demirjian method were compared. The height and weight of the children were measured and the BMI (weight in kilograms divided by squared height in meters) was calculated for each subject. (10) Afterwards, the calculated values were transferred to the age- and gender-specific curves. If the calculated number was higher than the 95th percentile, it was considered as obesity and if it was between the 95th and 5th percentiles, it was considered as normal weight. Afterwards, the differences between the estimated dental age and the chronologic age of the participants were analyzed based on gender and BMI classification. Statistical analyses were performed by the ANOVA test, Pearson correlation coefficient and linear regression in SPSS software. The significance level was set at 0.05.
Results
The study was performed on 104 digital panoramic radiographs of healthy 6 to 13-year-old children (52 boys and 52 girls) without any systemic disorders that had all the permanent teeth or tooth buds on the left side of the mandible. The average age of the subjects was 9.46±1.28 years with the minimum age of 6 years and the maximum age of 13 years. The average height was 115±3.2 cm and the average weight equaled 27.2±2.4 kg. Also, the minimum BMI equaled 13.21 and the maximum BMI equaled 28.31 with the average value of 20.74±3.18. From 52 male samples, 36 subjects had normal weight and 16 subjects were obese while from 52 female samples, 35 subjects had normal weight and 17 subjects were obese.
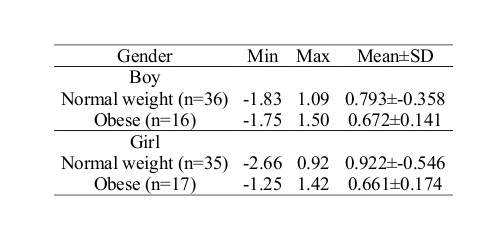
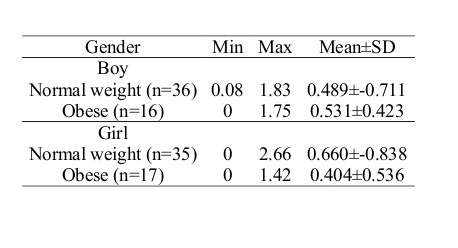
Overall, the difference between the chronologic age and dental age in the 104 samples equaled a minimum of -2.66 years and a maximum of +1.50 years. The mean difference between the chronologic age and dental age equaled -0.25±0.84 years. (Table 3) The absolute value of the diagnostic error in the present study ranged from a minimum of 0 to a maximum of 2.66 years with the average of 0.68±0.56 years. (Table 4) The repeatability coefficient (ICC) equaled 0.955. (Table 5) The correlation coefficient of the dental age estimated according to the Demirjian method and the chronologic age in normal weight and obese boys was 0.936 and 0.901 respectively, while in normal weight and obese girls, it equaled 0.916 and 0.942, respectively.
In 52 male samples, the below formula was calculated for the estimation of the chronologic age:
The dental age refers to the age calculated according to the Demirjian method. (12)
The chronologic age of normal weight individuals = (1.32+dental age×0.89)
The chronologic age of obese individuals = (1.07+dental age×0.87)
In 52 female samples, the below formula was calculated for the estimation of the chronologic age:
The chronologic age of normal weight individuals = (0.66+dental age×0.98)
The chronologic age of obese individuals = (1.19+dental age×0.85)
The following formula was calculated to estimate the chronologic age irrespective of gender:
The chronologic age = (1.13+dental age×0.905)
According to the two-way ANOVA test, age and gender variables do not have an interactive effect on the level of the estimate error (p=0.955). But the estimate error was different between normal weight and obese individuals (p=0.012), so that the estimate error in obese boys and girls was lower than that in the normal weight subjects. Also, the two-way ANOVA test showed that the interaction of the two variables was not significant in the difference between the estimated dental age and the chronologic age (p=0.516). But the difference between the chronologic age and the estimated dental age was significant between normal weight and obese subjects (p=0.00001), so that in normal weight subjects, the dental age was estimated to be lower than the chronologic age. The dental age in normal weight boys and girls was estimated to be -0.358 and -0.546 years lower respectively, and in obese boys and girls it was estimated to be +0.141 and +0.174 years more than the chronologic age, respectively.
Table 1- The scores related to each stage of dental maturation in boys and girls
Table 2-Dental maturation index conversion in boys and girls
Table 3- The mean difference between the estimated dental age and chronologic age based on gender and weight
Table 4- The absolute value of the diagnostic error based on gender and weight
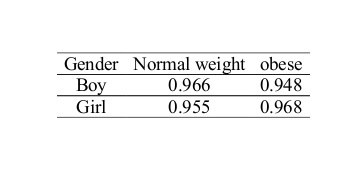
Table 5- The repeatability coefficient (ICC) by gender and weight
Discussion
The present study was performed on 104 digital panoramic radiograph samples of healthy 6 to 13-year-olds without any systemic disorders that had all the permanent teeth or tooth buds on the left side of the mandible. The average difference between the chronologic age and the estimated dental age equaled -0.25 years. Moreover, the repeatability coefficient (ICC) of 0.955 is also indicative of the high repeatability of the present study. Also, the high correlation coefficient in boys and in girls shows the high correlation between the dental age estimated by the Demirjian method and the chronologic age. Thus far, many studies have assessed the Demirjian method and its ability to estimate age in Iranian children. In these studies, the researchers concluded that the Demirjian method is a suitable technique for age estimation in Iranian children. (1,7,9)
The results of the present study showed that the dental age in children with normal weight is estimated lower than the chronologic age, but in obese children it is estimated higher, which shows that dental development is more advanced in obese children. The difference between the chronologic age and dental age in both obese and normal weight girls was higher than that in boys but overall, the age estimation error was not significantly correlated with gender and was only correlated with child's weight.
Hedayati et al in 2014 assessed the correlation between the BMI and skeletal maturation and dental development in 6 to 15-year-old children and found a direct correlation between accelerated dental maturation and increased BMI (p=0.002). (1) In a study by Eid et al on 6 to 14-year-old Brazilian children, no significant correlation was detected between dental maturation and BMI, but the results showed that on average, dental maturation of Brazilian children is 0.616 to 0.681 years more advanced than their chronologic age. (4) In the current study, the dental age of normal weight children was estimated lower than the chronologic age but in obese children, the dental age was higher than the chronologic age, and in fact there was a direct correlation between the BMI and dental development. Ethnical differences can be a reason for this difference between the results of these two studies.
Hilgers et al in 2006 concluded that the Demirjian method shows the dental age of American children to be higher than the chronologic age, but they also insisted on the positive effect of increasing BMI on dental maturation. They concluded that in overweight and obese children, the dental age is approximately 1.5 years more advanced than the chronologic age. (2) This finding is almost in line with the results of the present study. Also, they found that in girls, the difference between the chronologic age and dental age in both obese and normal weight groups was higher than that in boys. (2) This finding is also similar with our results. However, in both studies an accelerated dental development was noticed in obese children. The differences in the average numerical values can be due to ethnical diversity. Moreover, according to a study by Must et al in 2012 which involved 5 to 14-year-olds, obese children had a more advanced dental maturation compared with normal weight children and on average, in obese children dental maturation was 1.44 teeth more advanced than in normal weight children and a significant correlation was detected. (12) Mack et al in 2013 concluded that development of the cervical vertebrae and the dental age were more advanced in obese children. In these children, for a single unit change in BMI percentile, the dental age and cervical vertebrae development were 0.05 years more advanced. The mentioned study also indicated that obesity affects dental development. (13) Begherian et al in 2011 assessed the validity of the Demirjian method in a group of Iranian population. No significant correlation was detected between dental maturation and BMI. However, they stated that obesity affects dental maturation. (8) Likewise, in a study by Zangouei-Booshehri et al in 2011 the dental age in obese children was estimated higher than the chronologic age and a significant correlation was detected between age and BMI (p<0.01). In the mentioned study, similar to our study, children were divided to two groups of normal weight and obese according to the BMI and the results of the two studies were also similar. (14)
In a study by DuPlessis et al in 2016 also a significant correlation was detected between the BMI and dental development (p<0.01), however no difference was noticed between boys and girls. (17)
In a longitudinal study by Sanchez et al on Mexican elementary school children, the researchers found that overweight children with increasing BMI have more erupted teeth compared with other children in the same age (p<0.001) and that there is a complex correlation between the BMI and oral health in pediatric patients. (15)
Kumar et al in 2013 performed a study on 14 to 18-year-olds based on the Demirjian method, and found a direct correlation between the dental age and weight of the male subjects. (18)
Sadeghianrizi and colleagues explained the probable reasons for the accelerated dental growth in obese children. They stated that obese children in the pre-pubertal stage have a normal height despite the decreasing secretion of the growth hormone and the potential abnormality of the GH-insulin-like growth factor (IGF) system. Therefore, it has been stated that other factors such as hyperinsulinemia, decreasing level of GF-binding protein-1 (IGFBP-1) and increasing level of free IGF-1 (FIGF-1), which are effective growth proteins, can be influential in this process. (19)
Conclusion
The results of the present study showed that dental development is accelerated in obese children, and this should be considered in pediatric dental and orthodontic treatment planning.
Full-Text: (1081 Views)
Abstract
Background and aim: Methods of age estimation with the aid of radiography have higher accuracy compared with other methods. Some investigations have been performed in this regard, but the correlation between dental development and Body Mass Index (BMI) has been limitedly researched. In the present study, the correlation between dental development and BMI in the children referring to the dental school of Islamic Azad University of Tehran was evaluated with the use of panoramic radiography.
Materials and methods: In this cross-sectional analysis, panoramic radiographs of 104 children aged 6 to 13 years were evaluated. The date of radiography minus the birth date was used to determine the chronologic age for each child and then, this age was compared with the dental age estimated by the Demirjian method. Afterwards, the height and weight of the children were measured and the BMI was calculated for each subject. The difference between the estimated dental age and the chronologic age of the subjects was analyzed according to gender and BMI classification. Statistical analyses were performed using the ANOVA test, Pearson correlation coefficient and linear regression.
Results: In the 104 samples, the difference between the estimated dental age and the chronologic age was not significant (p=0.516). The dental age in normal weight children was lower than the chronologic age while in obese children, it was higher than the chronologic age (p=0.00001). The correlation coefficient of the estimated dental age using the Demirjian method and the chronologic age in normal weight and obese boys was 0.936 and 0.901, respectively, while in normal weight and obese girls, it equaled 0.916 and 0.942, respectively.
Conclusion: The results of the present study showed that dental development is accelerated in obese children.
Keywords: panoramic radiography, body mass index, age, odontogenesis
Introduction
Childhood obesity is an increasing concern and is partly due to sedentary lifestyle and nutritional habits. In Iran, childhood obesity is following an ascending trend. In addition to diseases such as diabetes, high blood pressure and heart diseases, obesity causes accelerated growth and early puberty in girls. Obesity can alter the onset of puberty in boys. (1) Recent studies show that obese children experience faster craniofacial growth, and this accelerated development is an important variable in pediatric dental and orthodontic treatments. (2) Neoviou et al in 2004 found that children with high Body Mass Index (BMI) have more erupted teeth. (3) Evaluation of dental development with the use of radiography has a higher efficacy in the estimation of the chronologic age of children compared with other maturation indices. In addition, dental development is a biological index in growing children, mostly as an indicator of dental age. Dental age of children can be estimated based on tooth eruption or based on dental formation stages according to radiographic observations. (4,5) One of the methods for determining dental development according to radiography is the Demirjian method which was first introduced in 1973 following a study on a large sample of Canadian children, and it evaluates the development of seven perah on the left side of the mandible using panoramic radiographs. All the teeth are classified from A to H and from the stage of formation of the first calcified points to apex closure. (6,7)
The efficacy of the Demirjian method has been assessed among some of the ethnicities. (8-11) Also in previous studies, the correlation between dental development and height and weight has been evaluated, which was found to be a significant correlation in many studies. (12-16)
Considering the controversies among the results of the previous studies and also the gap of information regarding this matter in Iran, the present study aimed to evaluate the correlation between the BMI and dental development in the patients referring to the oral and maxillofacial radiology department of the dental school of Islamic Azad University of Tehran.
Materials and methods
This cross-sectional analysis was performed on 104 children aged 6 to 13 years that referred for panoramic radiography. The 6 to 13-year-olds with seven permanent teeth (or tooth buds) on the left side of the mandible without any systemic or developmental diseases were included in the study. Radiographs of suitable quality were obtained as files from the radiology center and were saved in a laptop and the seven permanent teeth on the left side of the mandible were evaluated in each participant. All the dental buds pass different stages form the beginning of calcification to reach the final shape. (According to the Demirjian method). These stages are classified from A to H based on the stage of calcification. The stages of conversion of dental buds to the final form based on the degree of calcification include A: calcification at the tip of the cusps, B: connection of the calcified cusps, C: completion of enamel formation and beginning of dentin accumulation, D: completion of crown to the cemento-enamel junction (CEJ) area, E: parallel pulp chamber walls, root length less than coronal length, visible furcation, F: root length more than or equal to coronal length, funnel-shaped apex, G: parallel root walls and open apex, H: apex is closed and the periodontal ligament has a uniform width around the root. For each tooth, a numerical index was designated based on the determined developmental stage. With reference to table 1, this value was determined considering the gender of the subject. Indices for all the seven teeth were determined. The overall maturity score was obtained by summing up the seven indices, which ranged from 0 to 100. Then, with reference to table 2 the index was converted to dental age. (8,9) The chronologic age and the age calculated according to the Demirjian method were compared. The height and weight of the children were measured and the BMI (weight in kilograms divided by squared height in meters) was calculated for each subject. (10) Afterwards, the calculated values were transferred to the age- and gender-specific curves. If the calculated number was higher than the 95th percentile, it was considered as obesity and if it was between the 95th and 5th percentiles, it was considered as normal weight. Afterwards, the differences between the estimated dental age and the chronologic age of the participants were analyzed based on gender and BMI classification. Statistical analyses were performed by the ANOVA test, Pearson correlation coefficient and linear regression in SPSS software. The significance level was set at 0.05.
Results
The study was performed on 104 digital panoramic radiographs of healthy 6 to 13-year-old children (52 boys and 52 girls) without any systemic disorders that had all the permanent teeth or tooth buds on the left side of the mandible. The average age of the subjects was 9.46±1.28 years with the minimum age of 6 years and the maximum age of 13 years. The average height was 115±3.2 cm and the average weight equaled 27.2±2.4 kg. Also, the minimum BMI equaled 13.21 and the maximum BMI equaled 28.31 with the average value of 20.74±3.18. From 52 male samples, 36 subjects had normal weight and 16 subjects were obese while from 52 female samples, 35 subjects had normal weight and 17 subjects were obese.
Overall, the difference between the chronologic age and dental age in the 104 samples equaled a minimum of -2.66 years and a maximum of +1.50 years. The mean difference between the chronologic age and dental age equaled -0.25±0.84 years. (Table 3) The absolute value of the diagnostic error in the present study ranged from a minimum of 0 to a maximum of 2.66 years with the average of 0.68±0.56 years. (Table 4) The repeatability coefficient (ICC) equaled 0.955. (Table 5) The correlation coefficient of the dental age estimated according to the Demirjian method and the chronologic age in normal weight and obese boys was 0.936 and 0.901 respectively, while in normal weight and obese girls, it equaled 0.916 and 0.942, respectively.
In 52 male samples, the below formula was calculated for the estimation of the chronologic age:
The dental age refers to the age calculated according to the Demirjian method. (12)
The chronologic age of normal weight individuals = (1.32+dental age×0.89)
The chronologic age of obese individuals = (1.07+dental age×0.87)
In 52 female samples, the below formula was calculated for the estimation of the chronologic age:
The chronologic age of normal weight individuals = (0.66+dental age×0.98)
The chronologic age of obese individuals = (1.19+dental age×0.85)
The following formula was calculated to estimate the chronologic age irrespective of gender:
The chronologic age = (1.13+dental age×0.905)
According to the two-way ANOVA test, age and gender variables do not have an interactive effect on the level of the estimate error (p=0.955). But the estimate error was different between normal weight and obese individuals (p=0.012), so that the estimate error in obese boys and girls was lower than that in the normal weight subjects. Also, the two-way ANOVA test showed that the interaction of the two variables was not significant in the difference between the estimated dental age and the chronologic age (p=0.516). But the difference between the chronologic age and the estimated dental age was significant between normal weight and obese subjects (p=0.00001), so that in normal weight subjects, the dental age was estimated to be lower than the chronologic age. The dental age in normal weight boys and girls was estimated to be -0.358 and -0.546 years lower respectively, and in obese boys and girls it was estimated to be +0.141 and +0.174 years more than the chronologic age, respectively.
Table 1- The scores related to each stage of dental maturation in boys and girls
{kind=link}
Table 2-Dental maturation index conversion in boys and girls
{kind=link}
Table 3- The mean difference between the estimated dental age and chronologic age based on gender and weight
{kind=link}
Table 4- The absolute value of the diagnostic error based on gender and weight
{kind=link}
Table 5- The repeatability coefficient (ICC) by gender and weight
{kind=link}
Discussion
The present study was performed on 104 digital panoramic radiograph samples of healthy 6 to 13-year-olds without any systemic disorders that had all the permanent teeth or tooth buds on the left side of the mandible. The average difference between the chronologic age and the estimated dental age equaled -0.25 years. Moreover, the repeatability coefficient (ICC) of 0.955 is also indicative of the high repeatability of the present study. Also, the high correlation coefficient in boys and in girls shows the high correlation between the dental age estimated by the Demirjian method and the chronologic age. Thus far, many studies have assessed the Demirjian method and its ability to estimate age in Iranian children. In these studies, the researchers concluded that the Demirjian method is a suitable technique for age estimation in Iranian children. (1,7,9)
The results of the present study showed that the dental age in children with normal weight is estimated lower than the chronologic age, but in obese children it is estimated higher, which shows that dental development is more advanced in obese children. The difference between the chronologic age and dental age in both obese and normal weight girls was higher than that in boys but overall, the age estimation error was not significantly correlated with gender and was only correlated with child's weight.
Hedayati et al in 2014 assessed the correlation between the BMI and skeletal maturation and dental development in 6 to 15-year-old children and found a direct correlation between accelerated dental maturation and increased BMI (p=0.002). (1) In a study by Eid et al on 6 to 14-year-old Brazilian children, no significant correlation was detected between dental maturation and BMI, but the results showed that on average, dental maturation of Brazilian children is 0.616 to 0.681 years more advanced than their chronologic age. (4) In the current study, the dental age of normal weight children was estimated lower than the chronologic age but in obese children, the dental age was higher than the chronologic age, and in fact there was a direct correlation between the BMI and dental development. Ethnical differences can be a reason for this difference between the results of these two studies.
Hilgers et al in 2006 concluded that the Demirjian method shows the dental age of American children to be higher than the chronologic age, but they also insisted on the positive effect of increasing BMI on dental maturation. They concluded that in overweight and obese children, the dental age is approximately 1.5 years more advanced than the chronologic age. (2) This finding is almost in line with the results of the present study. Also, they found that in girls, the difference between the chronologic age and dental age in both obese and normal weight groups was higher than that in boys. (2) This finding is also similar with our results. However, in both studies an accelerated dental development was noticed in obese children. The differences in the average numerical values can be due to ethnical diversity. Moreover, according to a study by Must et al in 2012 which involved 5 to 14-year-olds, obese children had a more advanced dental maturation compared with normal weight children and on average, in obese children dental maturation was 1.44 teeth more advanced than in normal weight children and a significant correlation was detected. (12) Mack et al in 2013 concluded that development of the cervical vertebrae and the dental age were more advanced in obese children. In these children, for a single unit change in BMI percentile, the dental age and cervical vertebrae development were 0.05 years more advanced. The mentioned study also indicated that obesity affects dental development. (13) Begherian et al in 2011 assessed the validity of the Demirjian method in a group of Iranian population. No significant correlation was detected between dental maturation and BMI. However, they stated that obesity affects dental maturation. (8) Likewise, in a study by Zangouei-Booshehri et al in 2011 the dental age in obese children was estimated higher than the chronologic age and a significant correlation was detected between age and BMI (p<0.01). In the mentioned study, similar to our study, children were divided to two groups of normal weight and obese according to the BMI and the results of the two studies were also similar. (14)
In a study by DuPlessis et al in 2016 also a significant correlation was detected between the BMI and dental development (p<0.01), however no difference was noticed between boys and girls. (17)
In a longitudinal study by Sanchez et al on Mexican elementary school children, the researchers found that overweight children with increasing BMI have more erupted teeth compared with other children in the same age (p<0.001) and that there is a complex correlation between the BMI and oral health in pediatric patients. (15)
Kumar et al in 2013 performed a study on 14 to 18-year-olds based on the Demirjian method, and found a direct correlation between the dental age and weight of the male subjects. (18)
Sadeghianrizi and colleagues explained the probable reasons for the accelerated dental growth in obese children. They stated that obese children in the pre-pubertal stage have a normal height despite the decreasing secretion of the growth hormone and the potential abnormality of the GH-insulin-like growth factor (IGF) system. Therefore, it has been stated that other factors such as hyperinsulinemia, decreasing level of GF-binding protein-1 (IGFBP-1) and increasing level of free IGF-1 (FIGF-1), which are effective growth proteins, can be influential in this process. (19)
Conclusion
The results of the present study showed that dental development is accelerated in obese children, and this should be considered in pediatric dental and orthodontic treatment planning.
Type of Study: Original article |
Subject:
Radiology
References
1. Hedayati Z, Khalafinejad F. Relationship between Body Mass Index, Skeletal Maturation and Dental Development in 6- to 15- Year Old Orthodontic Patients in a Sample of Iranian Population. J Dent (Shiraz) 2014;15(4):180-6.
2. Hilgers KK, Akridge M, Scheetz JP, Kinane DE. Childhood obesity and dental development. Pediatr Dent 2006;28(1):18-22.
3. Neoviou MG, Linne YM, Barkeling BS, Rossner SO. Sensitivity and specificity of classification systems for fatness in adolescents. AM J clin Nutr 2004;80(3):597-603.
4. Eid RM, Simi R, Friggi MN, fisberg M. Assessment of dental maturity of Brazilian children aged 6 to 14 years using Demirjians method. Int J paediatr Dent 2002;12(6):423-8.
5. Nykänen R, Espeland L, Kvaal SI, Krogstad O. Validity of the Demirjian method for dental age estimation when applied to Norwegian children. Acta Odontol Sc and 1998;56(4):238-44.
6. Bagherpour A, Imanimoghaddam M, Bagherpour MR, Einolghozati M. Dental age assessment among Iranian children aged 6-13 years using the Demirjian method.Forensic Sci Int 2010; 197(1-3):121.e1-4.
7. Willems G, Van Olmen A, Spiessens B, Carels C. Dental Age Estimation in Belgian Children: Demirjian’s Technique Revisited. J Forensic Sci 2001;46(4):893-5.
8. Bagherian A, Sadeghi M. Assessment of dental maturity of children aged 3.5 to 13.5 years using the Demirjian method in an Iranian population. J Oral Sci 2011;53(1):37-42.
9. Ziad D. Baghdadi, Dental Maturity in Saudi Children Using the Demirjian Method: A Comparative Study and New Prediction Models. ISRN Dentistry 2013;2013:1-9.
10. Celikoglu M, Cantekin K, Ceylan I. Dental age assessment: the applicability of Demirjian method in eastern Turkish children. J Forensic Sci 2011;56 (Suppl 1):S220-2.
11. Flood SJ, Mitchell WJ, Oxnard CE, Turlach BA, McGeachie J. A Comparison of Demirjian's Four Dental Development Methods for Forensic Age Assessment. J Forensic Sci 2011;56(6):1610-5
12. Must A, Phillips SM, Tybor DJ, Lividini K, Hayes C. The association between childhood obesity and tooth eruption. Obesity (Silver Spring) 2012;20(10):2070-4.
13. Mack KB, Phillips C, Jain N, Koroluk LD. Relationship between body mass index percentile and skeletal maturation and dental development in orthodontic patients. Am J Orthod Dentofacial Orthop 2013;143(2):228-34.
14. Zangouei Booshehri M, Ezoddini Ardakani F,Agha Aghili H, Sharifi A. Assessment of the relationship between body mass index (BMI) and dental age. Health 2011;3(5):253-7.
15. Sanchez-perez L,Irigoyen ME,Zepeda M. Dental careis,tooth eruption timing and obesity: a longitudinal study in a group of Mexican schoolchildren.Acta odontol sc and 2010;68(1):57-64.
16. Samadi M, Sadrzade-Yeganeh H, Azadbakht L, Jafarian K, Rahimi A, Sotoudeh G. Sensitivity and specificity of body mass index in determining obesity in children. J Res Med Sci 2013;18(7):537-42.
17. DuPlessis EA, Araujo EA, Behrents RG, Kim KB. Relationship between body mass and dental and skeletal development in children and adolescents. Am J Orthod Dentofacial Orthop. 2016;150(2):268-73.
18. Kumar V, Venkataraghavan K, Krishnan R, Patil K, Munoli K, Karthik S. The relationship between dental age, bone age and chronological age in underweight children. J Pharm Bioallied Sci 2013;5(Suppl 1):S73-9.
19. Sadeghianrizi A, Forsberg CM,Marcus C,Dahllof G.Craniofacial development in obese adolescents. Eur J Orthod 2005;27(6):550-5.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |