Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 1 (3-2026)
J Res Dent Maxillofac Sci 2026, 11(1): 31-44 |
Back to browse issues page
Ethics code: IR.SBMU.DRC.REC.1404.004
Clinical trials code: IRCT20240807062679N1
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Molaasadolah F, Soltani M, Jafarian M. Clinical Efficacy and Pain of Computer-Controlled Intraosseous Anesthesia versus the Conventional Inferior Alveolar Nerve Block in Pulpotomy of Primary Molars: A Clinical Trial. J Res Dent Maxillofac Sci 2026; 11 (1) :31-44
URL: http://jrdms.dentaliau.ac.ir/article-1-1201-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-1201-en.html


1- Department of Pediatric Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Pediatric Dentistry, Faculty of Dentistry, Shahed University, Tehran, Iran. ,soltanimansooreh5@sbmu.ac.ir
3- Department of Oral and Maxillofacial Surgery, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Pediatric Dentistry, Faculty of Dentistry, Shahed University, Tehran, Iran. ,
3- Department of Oral and Maxillofacial Surgery, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 482 kb]
(34 Downloads)
| Abstract (HTML) (44 Views)
Table 1. Mean HR at different time points in the two groups
Table 2. Frequency distribution of WBPRS score at T1 (during injection) and T2 (during pulpotomy) based on the injection type in the two treatment sessions
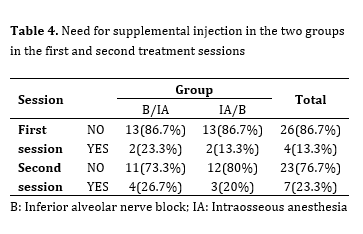
Need for supplemental injection: Table 4 shows the need for supplemental injection in the two groups in the first and second treatment sessions. Using the Fisher's exact test, there was no significant difference in the need for supplemental injections between the two types of injections in the first session (P=0.701) and the second session (P=0.500).
Secondary outcome:
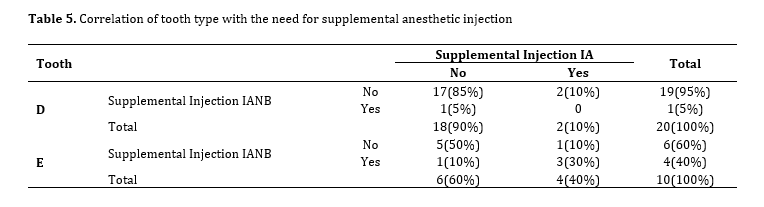
Tooth type: Of all teeth that underwent pulpotomy, 20 pairs were Ds (66.7%) and 10 pairs were Es (33.3%). Table 5 shows the correlation of tooth type with the need for supplemental anesthetic injection. The McNemar test showed that there was no statistically significant difference in the need for supplemental injections between Ds and Es (P=1.000).
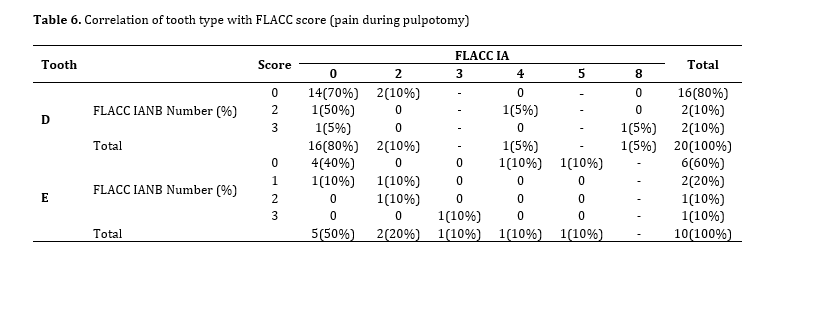
Table 6 shows the correlation of tooth type with the FLACC score (pain during pulpotomy). The Wilcoxon signed rank test showed that there was no statistically significant difference in FLACC score between the two methods in Ds (P=0.518) and Es (P=0.197).
Table 3. Frequency of different FLACC scores in the two treatment sessions in the two groups
Table 4. Need for supplemental injection in the two groups in the first and second treatment sessions
Table 5. Correlation of tooth type with the need for supplemental anesthetic injection
Table 6. Correlation of tooth type with FLACC score (pain during pulpotomy)
Discussion
This study compared the efficacy and pain of IA and the conventional IANB for pulpotomy of primary molars. This study was designed as a crossover randomized controlled trial. To limit inter-individual variability, a split-mouth design was used, and each patient was his or her own control group. Monteiro et al, [25] in their meta-analysis suggested that for this type of study, parallel design may be preferable to crossover design, because the initial level of patient anxiety in the second session depends on the success of the first session. In the present study, the results of the second session might have been influenced by the anesthetic experience in the first session (carry over effect). In the current study, randomization of the order of injections in the 2 groups was performed to eliminate this effect, and an adequate wash-out period between the 2 treatment sessions (14 days) was considered. However, despite these measures, it is not easy to erase the memory of this experience since the results of the intervention were assessed through behavioral measures and self-reported pain [26]. Therefore, to increase the reliability of the results, presence of period effect and carry-over effect was analyzed using statistical analysis, but the carry-over effect was not significant. Since the period effect was significant in assessment of pain during injection and the FLACC variable during treatment, the relationship between these two variables and the type of injection was analyzed in the first period. The results showed that pain during injection and efficacy of the IANB and IA were not significantly different.
Quantification of pain in children is challenging because the results of behavioral scales depend on the observer, and the results of self-reported scales depend on the age of children, and their level of perception and understanding of pain. Thus, physiological parameters such as HR may be used for objective measurement of pain in children. Nonetheless, such objective variables are not always correlated with the intensity of perceived pain by patients [27] and may cause bias, complicating precise assessment of the efficacy of IA [4]. In the present study, a combination of subjective and objective scales was used to maximize the methodological quality of the study and increase the reliability of the results. The current results showed no significant difference in WBPRS score (immediately after injection) and HR (during injection) between the two injection techniques. Similarly, AlRaddadi et al. [28] found no significant difference in pain perception and behavior between the buccal infiltration and intraosseous techniques. Also, Prol Castelo et al. [29] reported that although pain associated with intraosseous injection measured by the WBPRS was lower than the IANB, the physical reaction of children during injection, as measured by the FLACC, was not significantly different between the two techniques. On the other hand, unlike the present study, pain associated with intraosseous injection was lower than the conventional technique in some studies [16, 30, 31]. Methodological differences and using different methods for quantification of pain, different age range of children, type of randomization and blinding, type of device, type of dental procedure, anatomical location, and tooth type are among the main reasons for the observed differences in the results [4, 16, 29-31] . Smaïl-Faugeron et al. [16] stated that although the difference in pain scores between the IA injection and infiltration anesthesia in their study was statistically significant, it corresponded to less than one unit of the visual analog scale, which limits its clinical significance. Nonetheless, any benefit in terms of pain control for patients should not be overlooked [16]. Pain due to anesthetic injection can adversely affect the cooperation of pediatric dental patients; thus, any reduction in pain is an advantage. Therefore, although the present study found no significant difference in pain score between the two techniques, within-group comparison of injection pain showed significantly higher pain score associated with IANB in the group that received IA in the first session. Also, IANB increased the HR more than IA (although insignificantly), which can be due to higher pain of IANB. Many relevant previous studies did not use physiological parameters for pain assessment. Nonetheless, the results regarding the association of HR and injection type are controversial. Recent clinical trials have reported a transient increase in HR for a few minutes following intraosseous injection of 4% articaine with epinephrine using the Quick Sleeper computer-controlled system [32] Increased HR in intraosseous injection is attributed to faster entry of catecholamines into the vascular system [33]. Some studies used Quick Sleeper and did not report any increase in HR [28, 34] or reported an insignificant short-term increase following the use of 2% lidocaine plus 1:80,000 epinephrine. The increased HR and blood pressure changes during dental procedures are due to the release of endogenous catecholamines caused by emotional stress, and not the drug side effects [35]. The higher HR following IANB injection can be attributed to greater pain. Another reason could be that the dose of epinephrine administered to children with IANB was higher than with IA, because the volume of the anesthetic agent administered with IANB injection was greater than with IA injection. In any case, the transient increase in HR would not be clinically significant in most healthy patients [36]. Within-group comparison of pain during injection showed that in the IA/IANB injection order, the pain associated with IANB was significantly higher than in IA, but in the group with the IANB/IA injection order, this difference was not significant. The authors did not find an explanation for this finding, but it may be attributed to relatively small sample size. Further studies with a larger sample size are required on this topic to cast a final judgment. According to a meta-analysis by Monteiro et al, [25] success of anesthesia is a dependent variable that is not usually evaluated in clinical studies related to local anesthesia in children and adolescents. In the present study, the efficacy and success of the two techniques were evaluated by examining the HR during treatment, recording the FLACC behavioral scale during treatment, recording the WBPRS at the end of treatment, and the need for supplemental injections during pulpotomy treatment. The mean HR of children in the two techniques did not differ significantly at the time of pulp exposure during pulpotomy, and both groups had the highest difference in HR at the time of injection, and the lowest difference at the time of entering the pulp. Also, the mean HR was not significantly different at baseline and at the time of entering the pulp in the two groups, which indicates the comfort of the child and the effectiveness of both types of injections. Moreover, the pain reported by children after pulpotomy treatment using the WBPRS did not differ significantly in the two injection types. Within-group assessment of this scale after pulpotomy treatment revealed no difference between the two injection techniques. On the other hand, the pain recorded by the FLACC scale by the observer during pulpotomy treatment did not differ significantly in the two types of injections. This finding confirms lack of difference in efficacy between the two types of injections. The lack of need for supplemental injections during pulpotomy treatment indicates the effectiveness of both anesthetic injections. Similar to the present study, AlRaddadi et al. [34] showed no difference in effectiveness of infiltration anesthesia and intraosseous injection in pulpotomy of mandibular primary teeth. In the study by Prol Castelo et al. [29] similar to the present study, the need for supplemental injections, pain during treatment, and the child's behavior during treatment did not differ between IA and IANB injections. The effectiveness of IA and IANB injections by tooth type was also analyzed in this study. According to the FLACC scale and the need for supplemental injections, there was no statistically significant difference between Ds and Es. This result is reasonable because pulpal anesthesia of one quadrant of the mandible is achieved with IANB; although sometimes additional injections are required in some areas. Also, since intraosseous injections cause anesthesia of 3 adjacent teeth in the mandible by injecting half of the cartridge in the distal bone of the respective tooth [12], there is probably no difference in pulpal anesthesia of Ds and Es considering their anatomical location. The authors did not find similar studies on the effectiveness and pain of intraosseous injections versus conventional injections by tooth type to compare our results with.
This study had some limitations. Due to the difference in appearance of the Sleeper One5 device and the conventional syringe, it was not possible to blind the operator and children. Computerized injection systems have a learning curve. Before the study onset, the operator was trained on how to use the Sleeper One5 device, but the role of experience in using such technologies cannot be ignored. The high cost of the device, the need for a special needle, and the longer injection time are among the disadvantages of this device. Future studies are suggested to measure the level of anxiety of children before the procedure and compare the two types of anesthesia techniques in terms of the time to anesthesia, duration of anesthesia, and complications after the injection. Another limitation of this study was that we did not evaluate the minimal clinically important difference (MCID) for the FLACC and WBPRS pain scales. While statistical significance was assessed, interpretation of pain outcomes would be more meaningful if related to established MCID thresholds. As MCID values provide insight into whether observed differences are clinically relevant to patients, future studies should incorporate MCID and effect size analyses to strengthen the clinical interpretation of findings. This study compared 2 types of anesthesia techniques for pulpotomy treatment of mandibular primary molars in 30 cooperative 4–6-year-old children referred to Shahid Beheshti Dental School, which may affect the generalizability of the findings to other dental treatments and injections, other age groups, non-cooperative children, and different communities. Future studies with a larger sample size are required in other age groups, comparing different dental treatments and injections, and in different communities. Studies on non-cooperative children are also recommended.
Conclusion
The research results showed that IA administered by a CCLAD may be used as an alternative to IANB for pulpotomy of primary molars, due to comparable efficacy and injection pain, as shown by the HR, and self-reported and behavioral measures.
Full-Text: (14 Views)
Abstract
Background and Aim: This study assessed the efficacy of intraosseous anesthesia (IA) administered by a computer-controlled local anesthetic device (CCLAD) and its associated pain in comparison with the conventional inferior alveolar nerve block (IANB) for pulpotomy of primary molars.
Materials and Methods: This crossover split-mouth randomized controlled clinical trial was conducted on 30 children between 4-6 years requiring pulpotomy of mandibular primary molars bilaterally. The children were randomly assigned to two groups to receive IA and IANB in two orders of IA/IANB and IANB/IA within two treatment sessions. Pain during injection and during treatment was quantified subjectively using the Wong-Baker Faces Pain Rating Scale (WBPRS), and objectively using the Face, Legs, Activity, Cry, and Consolability (FLACC) scale. Heart rate (HR) was measured by a pulse oximeter, and the need for supplemental injection was recorded. Data were analyzed using repeated measures ANOVA, Wilcoxon, Mann-Whitney, Bonferroni, Fisher’s exact, and McNemar tests (alpha=0.05).
Results: Injection type had no significant effect on the HR in the first or second treatment session, injection pain, procedural pain, FLACC score, or the need for supplemental injection (P>0.05). Within-group comparison of pain in the IA/IANB group showed significantly higher pain associated with IANB (P=0.015) while this difference was not significant in the IANB/IA group (P>0.05). Primary first and second molars had no significant difference in FLACC score or the need for supplemental injection (P>0.05).
Conclusion: IA may be used as an alternative to IANB for pulpotomy of primary molars, due to comparable efficacy and injection pain.
Keywords: Anesthesia, Local; Mandibular Nerve; Pain; Heart Rate; Visual Analog Scale
Introduction
Management of dental fear and anxiety and limiting painful procedures to achieve sufficiently high level of cooperation are imperative in pediatric dentistry [1]. The patients associate maximum pain with local anesthetic injection, which causes the highest level of anxiety [2,3]. Pain from anesthetic injection can cause behavioral problems in young patients, and affect the clinician’s performance [4].
Infiltration anesthesia and inferior alveolar nerve block (IANB) injections are the most common techniques used in pediatric dentistry, which are administered with conventional dental syringes, disposable cartridges, and conventional needles [5]. The appearance of the conventional local anesthetic injection syringes can be intimidating and anxiety-inducing [6]. When performing pulpotomy for mandibular primary molars, the infiltration anesthesia technique is less effective than the IANB, possibly due to greater bone density that impedes diffusion of the anesthetic agent [7]. IANB injection can be painful and has the added risk of patient-induced soft tissue injury, nerve damage, and needle breakage [8]. A high prevalence of self-inflicted soft tissue injuries (tongue, lips, and cheeks) following local anesthesia has been reported in children, with a higher incidence in younger patients, especially after IANB [9]. Therefore, methods that provide adequate anesthesia for treatment but are not associated with prolonged anesthesia of the soft tissue are considered an advantage in pediatric dentistry.
Pain due to traditional syringe-based anesthetic injection is attributed to physical trauma during needle insertion, and tissue distension due to the introduction of the anesthetic agent [10]. However, it is difficult to control the pressure and rate of anesthetic injection with traditional syringes [11]. Intraosseous anesthesia (IA) is a local anesthetic technique in which the anesthetic agent is injected directly into the cancellous bone around the root, and is not accompanied by lip and tongue anesthesia. This technique was initially used only in special cases, such as failure of anesthesia induced by nerve block, need for short-term anesthesia, and patients at risk of bleeding [12]. According to the American Academy of Pediatric Dentistry, IA technique is reliable in children [5]. The advantages of this technique are numerous, and include immediate onset of action (30 seconds), the need for minimal local anesthetic volume, and low rate of postoperative complications [12]. Recently, computer-controlled local anesthetic devices (CCLADs) were introduced to the market. CCLAD generally refers to devices that not only slow and maintain the injection rate, but also keep the rate constant by taking into account the anatomical characteristics of the tissues being injected [4]. One of the newest CCLAD systems available in the market is the SleeperOne5 (Dentalhitec, France). This device consists of an electronic control unit, a pedal, and an injection pen that is noninvasive and capable of providing infiltration anesthesia, nerve block, intra-ligamental anesthesia, intra-septal anesthesia, and IA. This device uses specially designed needles. A review of the literature showed controversial results for reducing the injection pain and the effectiveness of anesthesia with the help of CCLADs [4, 13-16]. Studies comparing IA and IANB in pediatric dentistry are also limited. If pain during IA injection is reduced by using computer-controlled injection systems and these methods prove to be sufficient for complete anesthesia for treatment of primary molars, while avoiding prolonged soft tissue anesthesia and reducing the risk of tissue damage by the child himself after treatment, an important step will be taken in gaining children's cooperation for dental treatments. Thus, this study aimed to compare the efficacy of IA administered by a CCLAD and its associated pain in comparison with the conventional IANB for pulpotomy of primary molars.
Materials and Methods
This study was conducted at the Pediatric Dentistry Department of School of Dentistry, Shahid Beheshti University of Medical Sciences between April 2024 and March 2025 after obtaining ethical approval (IR.SBMU.DRC.REC.1404.0404), and registration in the Iranian Registry of Clinical Trials (IRCT20240807062679N1).
Trial design:
A double-blind split-mouth crossover randomized controlled clinical trial was designed in which one group received anesthetic injection through an IA in the first session and conventional IANB in the second session for pulpotomy of primary molars while this order was reverse in the other group. The results were reported according to the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings:
The inclusion criteria were 4-6-year-old children with the ability to comprehend and respond to self-report Wong-Baker Faces Pain Rating Scale (WBPRS), children with scores 3 and 4 of the Frankl behavior rating scale [17], requiring pulpotomy and stainless-steel crown for homologous primary molars in the right and left quadrants of the mandible, no history of previous dental procedure requiring anesthetic injection, no allergy to anesthetic agents, no intake of analgesics or medications affecting pain perception within 48 hours prior to treatment, complete systemic health with American Society of Anesthesiologists Physical Status Classification System 1, and no clinical or radiographic evidence of pulp degeneration (edema, sinus tract, mobility, PDL widening, sensitivity to percussion, history of continuous and spontaneous pain, internal/external root resorption, or periapical or inter-radicular radiolucency) [18].
The exclusion criteria were children showing uncooperative behavior during the procedure, parents not consenting to participation of their children in the study, and learning or communication problems.
The sample consisted of 30 eligible children presenting to the School of Dentistry of Shahid Beheshti University of Medical Sciences.
Interventions:
Thirty eligible children were enrolled after obtaining their parents’ written informed consent. An informatory session was first held for children to familiarize them with the dental office environment and equipment by the tell-show-do technique, and the children received a fluoride varnish. The level of cooperation of children in this session was assessed using the Frankl behavior rating scale [17], and those with class 3 and 4 were enrolled. The children were then randomly assigned to two groups of 15. In the first treatment session, children in group 1 received pulpotomy and stainless-steel crown for the primary molar of one mandibular quadrant following an IANB, which was administered by using a conventional 30-gauge, 21 mm syringe (NOP, South Korea) and 2% Xylopen cartridge (Exir, Iran) containing 20 mg lidocaine hydrochloride and 12.5 µg 1:80,000 epinephrine. In the second treatment session, the primary molar of the other mandibular quadrant of children in group 1 underwent pulpotomy after anesthetic injection by using the CCLAD (SleeperOne 5; Dental Hi-Tec, Cholet, France) with a short 9-mm, 30-gauge needle (Effitec, France) as instructed by the manufacturer. Children in group 2 received pulpotomy and stainless-steel crown for the primary molar of one mandibular quadrant after anesthetic injection by IA in their first treatment session, and conventional IANB in their second treatment session. The mandibular quadrant to be treated in the first session was selected randomly. The second treatment session was scheduled 14 days after the first session. Before the start of the trial, the postgraduate student who performed all clinical procedures was calibrated by an experienced pediatric dentist. Calibration was carried out through the independent assessment of several children using the same diagnostic and anesthetic criteria, and the level of inter-examiner agreement was determined using Cohen’s kappa (κ = 0.8), indicating substantial reliability.
It should be noted that gluten-free 20% benzocaine topical anesthetic gel (Avant Dental Supply ADS, USA) which contains xylitol and vitamin E was applied at the injection site for 30 seconds after drying the mucosa with a sterile gauze before all injections for all children. Both injections were performed using 2% lidocaine plus 1:80,000 epinephrine (Xylopen; Exir, Iran). The required amount of anesthetic agent for IANB was calculated according to the child’s weight. This amount in using the IA was half of the anesthetic cartridge as instructed by the manufacturer. In using the IA, first the gingiva was anesthetized by inserting the DHT Effitec needle (Dental Hi-Tec, Cholet, France) in almost parallel angulation such that its flat surface faced the mucosa. The needle was inserted by no more than 0.5 mm [19]. The injection was performed distal to the respective tooth; however, if the bone in this area was not suitable for injection, injection was performed mesial to the respective tooth. The needle was inserted into the interproximal septal bone through the interdental papilla tip with 20- to 45-degree buccolingual angulation, and injection was performed as such [19]. The children were treated in an isolated room to eliminate the confounding effect of the environment and behavior of other children in the area on the results [20].
The perceived pain by children was quantified subjectively at two time points i.e., after anesthetic injection (time 1) and after termination of pulpotomy treatment (time 2) using the WBPRS, which is a self-reporting scale for pain with confirmed validity and reliability for use in children [21]. The children were first briefed about this scale and how to use it before the treatment onset by a senior postgraduate student of pediatric dentistry. Children who could not learn or select a face were excluded and replaced.
The pain level was quantified objectively using the Face, Legs, Activity, Cry, and Consolability (FLACC) scale by an experienced pediatric dentist [22], who was blinded to the type of anesthetic injection technique. To assess intra-examiner reliability, 15% of the cases were randomly selected and re-scored by the same examiner after a two-week interval. The examiner was blinded to the initial scores, and the agreement between the two assessments was evaluated using Cohen’s kappa, which yielded a value of 0.80, indicating substantial reliability.
The heart rate (HR) was also recorded as a physiological parameter and an objective finding related to pain. The HR of children was recorded at 3 time points using a pulse oximeter (ChoiceMMed; China): prior to the procedure (time 0), during anesthetic injection (time 1), and during pulp exposure in pulpotomy (time 2).
The efficacy of the anesthetic injection technique was determined based on the level of pain experienced by children during treatment (FLACC scale), HR during pulp exposure, and the need for supplemental anesthetic injections during the procedure.
The wash-out period between interventions was set at 14 days. Although the pharmacologic effects of local anesthetics such as lidocaine resolve within hours, procedural responses related to pain perception and injection-associated anxiety may persist for several days. A 14-day interval provides a conservative buffer to ensure that participants are fully recovered both physiologically and psychologically before the subsequent session. This choice aligns with previous crossover investigations in dentistry that scheduled contralateral procedures at least two weeks apart to minimize potential carryover effect [23].
Outcomes:
Self-reported pain, FLACC score, HR, and the need for supplemental anesthesia were the primary outcomes. The effect of type of tooth was evaluated as the secondary outcome measure.
Sample size calculation:
The sample size was calculated to be 30 assuming alpha=0.05 (Z 1- α 2 =1.96 Z 1- β =0.84
Interim analyses and stopping guidelines:
None.
Randomization:
Each child was assigned a random code from 1 to 30 in sealed opaque envelopes, which were selected by the children themselves. A list of random numbers generated online (http://www.randomizer.org) was used to randomly assign children to two groups.
Blinding:
Since the appearance of the conventional syringe and SleeperOne 5 is different, blinding of the operator and children was not possible. However, the assessor of the FLACC scale was not aware of the anesthetic injection technique. Also, the statistician was blinded to the group allocations. Therefore, the study had an assessor- and statistician-blinded design.
Statistical analysis:
The normality of data distribution was examined using the Shapiro-Wilk test. According to the cross-over design of the study and according to the data distribution, the carry-over effect, period effect and treatment effect were analyzed using independent t-test and Mann-Whitney test. Comparison of the mean HR at T0 (before the procedure), T1 (during injection) and T2 (during pulp exposure) in the two types of injection techniques in each of the two periods (2 treatment sessions) was performed using two-way repeated measures ANOVA. Pairwise comparisons were made using the Bonferroni test. Also, within-group comparison for the WBPRS variable was performed using the Wilcoxon signed rank test. Comparison of the need for supplemental injection in the two injection techniques in each of the two treatment sessions was performed using the Fisher’s exact test. In order to investigate the effect of tooth type (D, E) on FLACC variable and the need for supplemental injection, the two types of injections were compared for the variable of need for supplemental injection using the McNemar test, and for the FLACC variable using the Wilcoxon signed rank test. Data analysis was performed using SPSS version 26 at 0.05 level of significance.
Results
Participant flow:
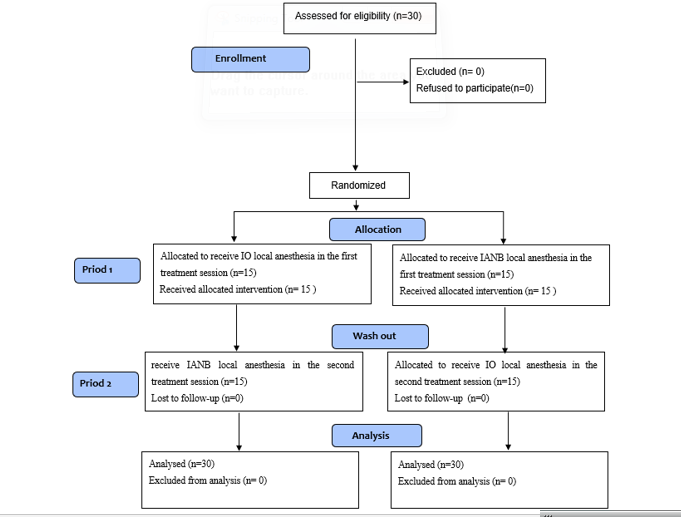
The sample consisted of 30 children including 15 females (50%) and 15 males (50%) with a mean age of 5.61±0.73 years (range 4.08 to 6.83 years). Figure 1 shows the CONSORT flow-diagram of the study. Considering the cross-over design of the study, first the carry-over effect and the period effect of the variables were examined, and then the treatment effect was analyzed. The period in our study was the treatment session (first or second), and the treatment type was IANB or IA with CCLAD.
Background and Aim: This study assessed the efficacy of intraosseous anesthesia (IA) administered by a computer-controlled local anesthetic device (CCLAD) and its associated pain in comparison with the conventional inferior alveolar nerve block (IANB) for pulpotomy of primary molars.
Materials and Methods: This crossover split-mouth randomized controlled clinical trial was conducted on 30 children between 4-6 years requiring pulpotomy of mandibular primary molars bilaterally. The children were randomly assigned to two groups to receive IA and IANB in two orders of IA/IANB and IANB/IA within two treatment sessions. Pain during injection and during treatment was quantified subjectively using the Wong-Baker Faces Pain Rating Scale (WBPRS), and objectively using the Face, Legs, Activity, Cry, and Consolability (FLACC) scale. Heart rate (HR) was measured by a pulse oximeter, and the need for supplemental injection was recorded. Data were analyzed using repeated measures ANOVA, Wilcoxon, Mann-Whitney, Bonferroni, Fisher’s exact, and McNemar tests (alpha=0.05).
Results: Injection type had no significant effect on the HR in the first or second treatment session, injection pain, procedural pain, FLACC score, or the need for supplemental injection (P>0.05). Within-group comparison of pain in the IA/IANB group showed significantly higher pain associated with IANB (P=0.015) while this difference was not significant in the IANB/IA group (P>0.05). Primary first and second molars had no significant difference in FLACC score or the need for supplemental injection (P>0.05).
Conclusion: IA may be used as an alternative to IANB for pulpotomy of primary molars, due to comparable efficacy and injection pain.
Keywords: Anesthesia, Local; Mandibular Nerve; Pain; Heart Rate; Visual Analog Scale
Introduction
Management of dental fear and anxiety and limiting painful procedures to achieve sufficiently high level of cooperation are imperative in pediatric dentistry [1]. The patients associate maximum pain with local anesthetic injection, which causes the highest level of anxiety [2,3]. Pain from anesthetic injection can cause behavioral problems in young patients, and affect the clinician’s performance [4].
Infiltration anesthesia and inferior alveolar nerve block (IANB) injections are the most common techniques used in pediatric dentistry, which are administered with conventional dental syringes, disposable cartridges, and conventional needles [5]. The appearance of the conventional local anesthetic injection syringes can be intimidating and anxiety-inducing [6]. When performing pulpotomy for mandibular primary molars, the infiltration anesthesia technique is less effective than the IANB, possibly due to greater bone density that impedes diffusion of the anesthetic agent [7]. IANB injection can be painful and has the added risk of patient-induced soft tissue injury, nerve damage, and needle breakage [8]. A high prevalence of self-inflicted soft tissue injuries (tongue, lips, and cheeks) following local anesthesia has been reported in children, with a higher incidence in younger patients, especially after IANB [9]. Therefore, methods that provide adequate anesthesia for treatment but are not associated with prolonged anesthesia of the soft tissue are considered an advantage in pediatric dentistry.
Pain due to traditional syringe-based anesthetic injection is attributed to physical trauma during needle insertion, and tissue distension due to the introduction of the anesthetic agent [10]. However, it is difficult to control the pressure and rate of anesthetic injection with traditional syringes [11]. Intraosseous anesthesia (IA) is a local anesthetic technique in which the anesthetic agent is injected directly into the cancellous bone around the root, and is not accompanied by lip and tongue anesthesia. This technique was initially used only in special cases, such as failure of anesthesia induced by nerve block, need for short-term anesthesia, and patients at risk of bleeding [12]. According to the American Academy of Pediatric Dentistry, IA technique is reliable in children [5]. The advantages of this technique are numerous, and include immediate onset of action (30 seconds), the need for minimal local anesthetic volume, and low rate of postoperative complications [12]. Recently, computer-controlled local anesthetic devices (CCLADs) were introduced to the market. CCLAD generally refers to devices that not only slow and maintain the injection rate, but also keep the rate constant by taking into account the anatomical characteristics of the tissues being injected [4]. One of the newest CCLAD systems available in the market is the SleeperOne5 (Dentalhitec, France). This device consists of an electronic control unit, a pedal, and an injection pen that is noninvasive and capable of providing infiltration anesthesia, nerve block, intra-ligamental anesthesia, intra-septal anesthesia, and IA. This device uses specially designed needles. A review of the literature showed controversial results for reducing the injection pain and the effectiveness of anesthesia with the help of CCLADs [4, 13-16]. Studies comparing IA and IANB in pediatric dentistry are also limited. If pain during IA injection is reduced by using computer-controlled injection systems and these methods prove to be sufficient for complete anesthesia for treatment of primary molars, while avoiding prolonged soft tissue anesthesia and reducing the risk of tissue damage by the child himself after treatment, an important step will be taken in gaining children's cooperation for dental treatments. Thus, this study aimed to compare the efficacy of IA administered by a CCLAD and its associated pain in comparison with the conventional IANB for pulpotomy of primary molars.
Materials and Methods
This study was conducted at the Pediatric Dentistry Department of School of Dentistry, Shahid Beheshti University of Medical Sciences between April 2024 and March 2025 after obtaining ethical approval (IR.SBMU.DRC.REC.1404.0404), and registration in the Iranian Registry of Clinical Trials (IRCT20240807062679N1).
Trial design:
A double-blind split-mouth crossover randomized controlled clinical trial was designed in which one group received anesthetic injection through an IA in the first session and conventional IANB in the second session for pulpotomy of primary molars while this order was reverse in the other group. The results were reported according to the Consolidated Standards of Reporting Trials.
Participants, eligibility criteria, and settings:
The inclusion criteria were 4-6-year-old children with the ability to comprehend and respond to self-report Wong-Baker Faces Pain Rating Scale (WBPRS), children with scores 3 and 4 of the Frankl behavior rating scale [17], requiring pulpotomy and stainless-steel crown for homologous primary molars in the right and left quadrants of the mandible, no history of previous dental procedure requiring anesthetic injection, no allergy to anesthetic agents, no intake of analgesics or medications affecting pain perception within 48 hours prior to treatment, complete systemic health with American Society of Anesthesiologists Physical Status Classification System 1, and no clinical or radiographic evidence of pulp degeneration (edema, sinus tract, mobility, PDL widening, sensitivity to percussion, history of continuous and spontaneous pain, internal/external root resorption, or periapical or inter-radicular radiolucency) [18].
The exclusion criteria were children showing uncooperative behavior during the procedure, parents not consenting to participation of their children in the study, and learning or communication problems.
The sample consisted of 30 eligible children presenting to the School of Dentistry of Shahid Beheshti University of Medical Sciences.
Interventions:
Thirty eligible children were enrolled after obtaining their parents’ written informed consent. An informatory session was first held for children to familiarize them with the dental office environment and equipment by the tell-show-do technique, and the children received a fluoride varnish. The level of cooperation of children in this session was assessed using the Frankl behavior rating scale [17], and those with class 3 and 4 were enrolled. The children were then randomly assigned to two groups of 15. In the first treatment session, children in group 1 received pulpotomy and stainless-steel crown for the primary molar of one mandibular quadrant following an IANB, which was administered by using a conventional 30-gauge, 21 mm syringe (NOP, South Korea) and 2% Xylopen cartridge (Exir, Iran) containing 20 mg lidocaine hydrochloride and 12.5 µg 1:80,000 epinephrine. In the second treatment session, the primary molar of the other mandibular quadrant of children in group 1 underwent pulpotomy after anesthetic injection by using the CCLAD (SleeperOne 5; Dental Hi-Tec, Cholet, France) with a short 9-mm, 30-gauge needle (Effitec, France) as instructed by the manufacturer. Children in group 2 received pulpotomy and stainless-steel crown for the primary molar of one mandibular quadrant after anesthetic injection by IA in their first treatment session, and conventional IANB in their second treatment session. The mandibular quadrant to be treated in the first session was selected randomly. The second treatment session was scheduled 14 days after the first session. Before the start of the trial, the postgraduate student who performed all clinical procedures was calibrated by an experienced pediatric dentist. Calibration was carried out through the independent assessment of several children using the same diagnostic and anesthetic criteria, and the level of inter-examiner agreement was determined using Cohen’s kappa (κ = 0.8), indicating substantial reliability.
It should be noted that gluten-free 20% benzocaine topical anesthetic gel (Avant Dental Supply ADS, USA) which contains xylitol and vitamin E was applied at the injection site for 30 seconds after drying the mucosa with a sterile gauze before all injections for all children. Both injections were performed using 2% lidocaine plus 1:80,000 epinephrine (Xylopen; Exir, Iran). The required amount of anesthetic agent for IANB was calculated according to the child’s weight. This amount in using the IA was half of the anesthetic cartridge as instructed by the manufacturer. In using the IA, first the gingiva was anesthetized by inserting the DHT Effitec needle (Dental Hi-Tec, Cholet, France) in almost parallel angulation such that its flat surface faced the mucosa. The needle was inserted by no more than 0.5 mm [19]. The injection was performed distal to the respective tooth; however, if the bone in this area was not suitable for injection, injection was performed mesial to the respective tooth. The needle was inserted into the interproximal septal bone through the interdental papilla tip with 20- to 45-degree buccolingual angulation, and injection was performed as such [19]. The children were treated in an isolated room to eliminate the confounding effect of the environment and behavior of other children in the area on the results [20].
The perceived pain by children was quantified subjectively at two time points i.e., after anesthetic injection (time 1) and after termination of pulpotomy treatment (time 2) using the WBPRS, which is a self-reporting scale for pain with confirmed validity and reliability for use in children [21]. The children were first briefed about this scale and how to use it before the treatment onset by a senior postgraduate student of pediatric dentistry. Children who could not learn or select a face were excluded and replaced.
The pain level was quantified objectively using the Face, Legs, Activity, Cry, and Consolability (FLACC) scale by an experienced pediatric dentist [22], who was blinded to the type of anesthetic injection technique. To assess intra-examiner reliability, 15% of the cases were randomly selected and re-scored by the same examiner after a two-week interval. The examiner was blinded to the initial scores, and the agreement between the two assessments was evaluated using Cohen’s kappa, which yielded a value of 0.80, indicating substantial reliability.
The heart rate (HR) was also recorded as a physiological parameter and an objective finding related to pain. The HR of children was recorded at 3 time points using a pulse oximeter (ChoiceMMed; China): prior to the procedure (time 0), during anesthetic injection (time 1), and during pulp exposure in pulpotomy (time 2).
The efficacy of the anesthetic injection technique was determined based on the level of pain experienced by children during treatment (FLACC scale), HR during pulp exposure, and the need for supplemental anesthetic injections during the procedure.
The wash-out period between interventions was set at 14 days. Although the pharmacologic effects of local anesthetics such as lidocaine resolve within hours, procedural responses related to pain perception and injection-associated anxiety may persist for several days. A 14-day interval provides a conservative buffer to ensure that participants are fully recovered both physiologically and psychologically before the subsequent session. This choice aligns with previous crossover investigations in dentistry that scheduled contralateral procedures at least two weeks apart to minimize potential carryover effect [23].
Outcomes:
Self-reported pain, FLACC score, HR, and the need for supplemental anesthesia were the primary outcomes. The effect of type of tooth was evaluated as the secondary outcome measure.
Sample size calculation:
The sample size was calculated to be 30 assuming alpha=0.05 (
Interim analyses and stopping guidelines:
None.
Randomization:
Each child was assigned a random code from 1 to 30 in sealed opaque envelopes, which were selected by the children themselves. A list of random numbers generated online (http://www.randomizer.org) was used to randomly assign children to two groups.
Blinding:
Since the appearance of the conventional syringe and SleeperOne 5 is different, blinding of the operator and children was not possible. However, the assessor of the FLACC scale was not aware of the anesthetic injection technique. Also, the statistician was blinded to the group allocations. Therefore, the study had an assessor- and statistician-blinded design.
Statistical analysis:
The normality of data distribution was examined using the Shapiro-Wilk test. According to the cross-over design of the study and according to the data distribution, the carry-over effect, period effect and treatment effect were analyzed using independent t-test and Mann-Whitney test. Comparison of the mean HR at T0 (before the procedure), T1 (during injection) and T2 (during pulp exposure) in the two types of injection techniques in each of the two periods (2 treatment sessions) was performed using two-way repeated measures ANOVA. Pairwise comparisons were made using the Bonferroni test. Also, within-group comparison for the WBPRS variable was performed using the Wilcoxon signed rank test. Comparison of the need for supplemental injection in the two injection techniques in each of the two treatment sessions was performed using the Fisher’s exact test. In order to investigate the effect of tooth type (D, E) on FLACC variable and the need for supplemental injection, the two types of injections were compared for the variable of need for supplemental injection using the McNemar test, and for the FLACC variable using the Wilcoxon signed rank test. Data analysis was performed using SPSS version 26 at 0.05 level of significance.
Results
Participant flow:
The sample consisted of 30 children including 15 females (50%) and 15 males (50%) with a mean age of 5.61±0.73 years (range 4.08 to 6.83 years). Figure 1 shows the CONSORT flow-diagram of the study. Considering the cross-over design of the study, first the carry-over effect and the period effect of the variables were examined, and then the treatment effect was analyzed. The period in our study was the treatment session (first or second), and the treatment type was IANB or IA with CCLAD.
{kind=link}
Harms:
No patients were harmed during the study.
Subgroup analyses:
Primary outcomes:
HR: Table 1 presents the HR of the patients in the two groups at different time points. Due to normal distribution of carry over effect on HR at all three time points, independent t-test was applied, which showed that the carry-over effect on HR was not significant at any time point (P=0.182 for T0, P=0.627 at T1, and P=0.870 at T2). Independent t-test (due to the normal distribution of the period effect on HR at T0 and T2) and Mann-Whitney U test (due to its non-normal distribution at T1) showed that the period effect on HR was not significant (P=0.609 for T0, P=0.325 for T1, and P=0.958 for T2).
Given the normal distribution of the treatment effect on HR at T0 and T2, and non-normal distribution of this variable at T1, the effect of injection type was compared at T0 and T2 using independent t-test, and at T1 using the Mann–Whitney test. The results showed that there was no statistically significant difference in the mean HR of children in the two types of injections at any of the three time points (P=0.154 for T0, P=0.148 for T1, and P=0.259 for T2). Despite lack of a significant difference, IANB increased the HR of children more than the IA, although insignificant. The largest difference in HR between the two injection techniques was at T1, and the smallest at T2 (although insignificant).
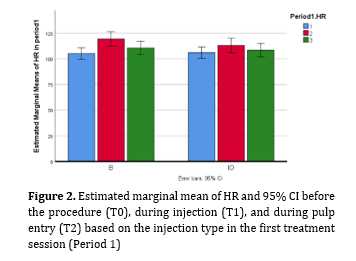
Comparison of the mean HR at T0, T1, and T2 in first treatment session was performed with respect to the type of injection using two-way repeated measures ANOVA. The results showed that the mean HR had a statistically significant difference at three times (P<0.001). Based on the results of Figure 2 and using the Bonferroni method, the HR at injection time was higher than both T0 and T2 (P<0.001 in both comparisons). However, T0 and T2 did not have a statistically significant difference in this regard (P=0.460). Also, the interaction effect of time and injection type was not significant (P>0.05). That is, a similar trend of change in HR was seen in both types of injections. The effect of injection type on HR was not significant either (P=0.506). That is, what caused the fluctuation of HR was not the type of injection, but the time.
Figure 2. Estimated marginal mean of HR and 95% CI before the procedure (T0), during injection (T1), and during pulp entry (T2) based on the injection type in the first treatment session (Period 1)
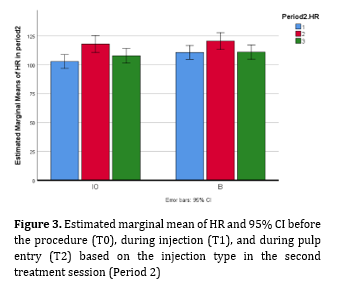
To assess the changes in the mean HR at T0, T1 and T2 in the second treatment session, two-way repeated measures ANOVA was used independently based on the injection type, and the results indicated a significant difference in HR at the three time points in this period (P<0.001). As shown in Figure 3, pairwise comparisons by the Bonferroni test showed that the mean HR at T1 was significantly higher than T0 (P<0.001) and T2 (P=0.001), and T0 and T2 did not have a statistically significant difference (P=0.460). The effect of injection type was not significant (P=0.251), and the interaction effect of time and injection type was not significant either (P=0.340). That is, an increase in the mean HR from T0 to T1 and then a decrease from T1 to T2 were seen in both types of injections.
No patients were harmed during the study.
Subgroup analyses:
Primary outcomes:
HR: Table 1 presents the HR of the patients in the two groups at different time points. Due to normal distribution of carry over effect on HR at all three time points, independent t-test was applied, which showed that the carry-over effect on HR was not significant at any time point (P=0.182 for T0, P=0.627 at T1, and P=0.870 at T2). Independent t-test (due to the normal distribution of the period effect on HR at T0 and T2) and Mann-Whitney U test (due to its non-normal distribution at T1) showed that the period effect on HR was not significant (P=0.609 for T0, P=0.325 for T1, and P=0.958 for T2).
Given the normal distribution of the treatment effect on HR at T0 and T2, and non-normal distribution of this variable at T1, the effect of injection type was compared at T0 and T2 using independent t-test, and at T1 using the Mann–Whitney test. The results showed that there was no statistically significant difference in the mean HR of children in the two types of injections at any of the three time points (P=0.154 for T0, P=0.148 for T1, and P=0.259 for T2). Despite lack of a significant difference, IANB increased the HR of children more than the IA, although insignificant. The largest difference in HR between the two injection techniques was at T1, and the smallest at T2 (although insignificant).
Comparison of the mean HR at T0, T1, and T2 in first treatment session was performed with respect to the type of injection using two-way repeated measures ANOVA. The results showed that the mean HR had a statistically significant difference at three times (P<0.001). Based on the results of Figure 2 and using the Bonferroni method, the HR at injection time was higher than both T0 and T2 (P<0.001 in both comparisons). However, T0 and T2 did not have a statistically significant difference in this regard (P=0.460). Also, the interaction effect of time and injection type was not significant (P>0.05). That is, a similar trend of change in HR was seen in both types of injections. The effect of injection type on HR was not significant either (P=0.506). That is, what caused the fluctuation of HR was not the type of injection, but the time.
Figure 2. Estimated marginal mean of HR and 95% CI before the procedure (T0), during injection (T1), and during pulp entry (T2) based on the injection type in the first treatment session (Period 1)
{kind=link}
To assess the changes in the mean HR at T0, T1 and T2 in the second treatment session, two-way repeated measures ANOVA was used independently based on the injection type, and the results indicated a significant difference in HR at the three time points in this period (P<0.001). As shown in Figure 3, pairwise comparisons by the Bonferroni test showed that the mean HR at T1 was significantly higher than T0 (P<0.001) and T2 (P=0.001), and T0 and T2 did not have a statistically significant difference (P=0.460). The effect of injection type was not significant (P=0.251), and the interaction effect of time and injection type was not significant either (P=0.340). That is, an increase in the mean HR from T0 to T1 and then a decrease from T1 to T2 were seen in both types of injections.
Figure 3. Estimated marginal mean of HR and 95% CI before the procedure (T0), during injection (T1), and during pulp entry (T2) based on the injection type in the second treatment session (Period 2)
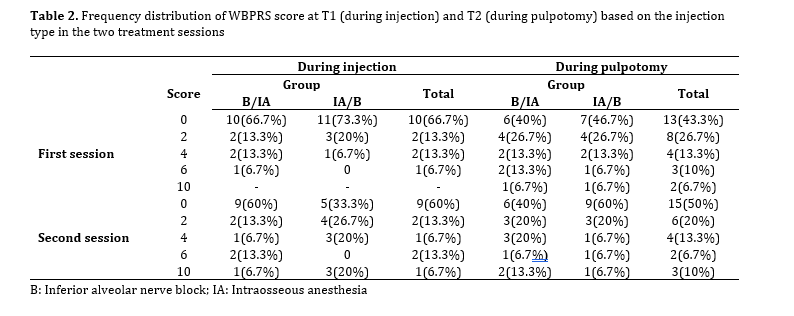
WBPRS score: Table 2 shows the WBPRS score at T1 (during injection) and T2 (during pulpotomy) based on the injection type in the two treatment sessions. Due to the non-normal distribution of the carry-over effect variable for the WBPRS, this effect was analyzed using the Mann-Whitney test. The results showed that the carry-over effect was not significant at T1 (P=0.486) and T2 (P=0.512). Also, due to the non-normal distribution of the period effect at T1, the Mann-Whitney test was used, which indicated the significance of the period effect at T1 (P=0.033). Due to the normal distribution of the period effect variable at T2, the period effect was analyzed using independent t-test, and the results indicated that the period effect at T2 was not significant (P=0.867).
Given the normal distribution of the treatment effect variable at T2, independent t-test was used to compare the effects of the two injection types. The results showed that at this time point, the effect of injection type was not significant (P=0.616), and the injection type had no effect on the pain score during pulpotomy treatment. Since the period effect was significant at T1, assessment of the relationship between the injection type and pain perceived during injection was performed using the Mann-Whitney test only in the first period (first session). The results indicated that there was no difference between the two types of injections (P=0.586), and the injection type had no effect on the pain perceived during injection.
Within-group comparison of the WBPRS by the Wilcoxon signed rank test showed that at the time of injection, the difference in pain reported between the two injection methods in each of the 2 treatment sessions was not significant in the IANB/IA group (P=0.266). While in the IA/IANB group, the pain associated with IANB was more than IA (P=0.015). However, at T2 (during pulpotomy), the two groups did not have a significant difference in the reported pain (P=0.355 and P=0.356, respectively).
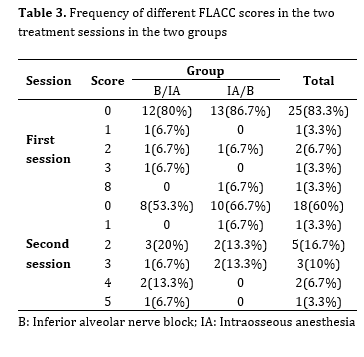
FLACC score: Table 3 presents the frequency of different FLACC scores in the two treatment sessions in the two groups. Due to the non-normal distribution of the carry-over effect, period effect, and treatment effect for the FLACC variable with normal distribution, evaluation of the effects of these three factors was performed using the Mann-Whitney test. The results showed that the carry-over effect was not significant (P=0.461). However, the period effect was significant (P=0.045). The effect of type of injection on the FLACC variable (pain during pulpotomy treatment) was not significant (P=0.233). Given the significance of the period effect, the effect of the type of injection was also compared in first session, and the results showed that the difference between the two types of injections was not significant in this period (P=0.933).
{kind=link}
WBPRS score: Table 2 shows the WBPRS score at T1 (during injection) and T2 (during pulpotomy) based on the injection type in the two treatment sessions. Due to the non-normal distribution of the carry-over effect variable for the WBPRS, this effect was analyzed using the Mann-Whitney test. The results showed that the carry-over effect was not significant at T1 (P=0.486) and T2 (P=0.512). Also, due to the non-normal distribution of the period effect at T1, the Mann-Whitney test was used, which indicated the significance of the period effect at T1 (P=0.033). Due to the normal distribution of the period effect variable at T2, the period effect was analyzed using independent t-test, and the results indicated that the period effect at T2 was not significant (P=0.867).
Given the normal distribution of the treatment effect variable at T2, independent t-test was used to compare the effects of the two injection types. The results showed that at this time point, the effect of injection type was not significant (P=0.616), and the injection type had no effect on the pain score during pulpotomy treatment. Since the period effect was significant at T1, assessment of the relationship between the injection type and pain perceived during injection was performed using the Mann-Whitney test only in the first period (first session). The results indicated that there was no difference between the two types of injections (P=0.586), and the injection type had no effect on the pain perceived during injection.
Within-group comparison of the WBPRS by the Wilcoxon signed rank test showed that at the time of injection, the difference in pain reported between the two injection methods in each of the 2 treatment sessions was not significant in the IANB/IA group (P=0.266). While in the IA/IANB group, the pain associated with IANB was more than IA (P=0.015). However, at T2 (during pulpotomy), the two groups did not have a significant difference in the reported pain (P=0.355 and P=0.356, respectively).
FLACC score: Table 3 presents the frequency of different FLACC scores in the two treatment sessions in the two groups. Due to the non-normal distribution of the carry-over effect, period effect, and treatment effect for the FLACC variable with normal distribution, evaluation of the effects of these three factors was performed using the Mann-Whitney test. The results showed that the carry-over effect was not significant (P=0.461). However, the period effect was significant (P=0.045). The effect of type of injection on the FLACC variable (pain during pulpotomy treatment) was not significant (P=0.233). Given the significance of the period effect, the effect of the type of injection was also compared in first session, and the results showed that the difference between the two types of injections was not significant in this period (P=0.933).
Table 1. Mean HR at different time points in the two groups
{kind=link}
Table 2. Frequency distribution of WBPRS score at T1 (during injection) and T2 (during pulpotomy) based on the injection type in the two treatment sessions
{kind=link}
Need for supplemental injection: Table 4 shows the need for supplemental injection in the two groups in the first and second treatment sessions. Using the Fisher's exact test, there was no significant difference in the need for supplemental injections between the two types of injections in the first session (P=0.701) and the second session (P=0.500).
Secondary outcome:
Tooth type: Of all teeth that underwent pulpotomy, 20 pairs were Ds (66.7%) and 10 pairs were Es (33.3%). Table 5 shows the correlation of tooth type with the need for supplemental anesthetic injection. The McNemar test showed that there was no statistically significant difference in the need for supplemental injections between Ds and Es (P=1.000).
Table 6 shows the correlation of tooth type with the FLACC score (pain during pulpotomy). The Wilcoxon signed rank test showed that there was no statistically significant difference in FLACC score between the two methods in Ds (P=0.518) and Es (P=0.197).
Table 3. Frequency of different FLACC scores in the two treatment sessions in the two groups
{kind=link}
Table 4. Need for supplemental injection in the two groups in the first and second treatment sessions
{kind=link}
Table 5. Correlation of tooth type with the need for supplemental anesthetic injection
{kind=link}
Table 6. Correlation of tooth type with FLACC score (pain during pulpotomy)
{kind=link}
Discussion
This study compared the efficacy and pain of IA and the conventional IANB for pulpotomy of primary molars. This study was designed as a crossover randomized controlled trial. To limit inter-individual variability, a split-mouth design was used, and each patient was his or her own control group. Monteiro et al, [25] in their meta-analysis suggested that for this type of study, parallel design may be preferable to crossover design, because the initial level of patient anxiety in the second session depends on the success of the first session. In the present study, the results of the second session might have been influenced by the anesthetic experience in the first session (carry over effect). In the current study, randomization of the order of injections in the 2 groups was performed to eliminate this effect, and an adequate wash-out period between the 2 treatment sessions (14 days) was considered. However, despite these measures, it is not easy to erase the memory of this experience since the results of the intervention were assessed through behavioral measures and self-reported pain [26]. Therefore, to increase the reliability of the results, presence of period effect and carry-over effect was analyzed using statistical analysis, but the carry-over effect was not significant. Since the period effect was significant in assessment of pain during injection and the FLACC variable during treatment, the relationship between these two variables and the type of injection was analyzed in the first period. The results showed that pain during injection and efficacy of the IANB and IA were not significantly different.
Quantification of pain in children is challenging because the results of behavioral scales depend on the observer, and the results of self-reported scales depend on the age of children, and their level of perception and understanding of pain. Thus, physiological parameters such as HR may be used for objective measurement of pain in children. Nonetheless, such objective variables are not always correlated with the intensity of perceived pain by patients [27] and may cause bias, complicating precise assessment of the efficacy of IA [4]. In the present study, a combination of subjective and objective scales was used to maximize the methodological quality of the study and increase the reliability of the results. The current results showed no significant difference in WBPRS score (immediately after injection) and HR (during injection) between the two injection techniques. Similarly, AlRaddadi et al. [28] found no significant difference in pain perception and behavior between the buccal infiltration and intraosseous techniques. Also, Prol Castelo et al. [29] reported that although pain associated with intraosseous injection measured by the WBPRS was lower than the IANB, the physical reaction of children during injection, as measured by the FLACC, was not significantly different between the two techniques. On the other hand, unlike the present study, pain associated with intraosseous injection was lower than the conventional technique in some studies [16, 30, 31]. Methodological differences and using different methods for quantification of pain, different age range of children, type of randomization and blinding, type of device, type of dental procedure, anatomical location, and tooth type are among the main reasons for the observed differences in the results [4, 16, 29-31] . Smaïl-Faugeron et al. [16] stated that although the difference in pain scores between the IA injection and infiltration anesthesia in their study was statistically significant, it corresponded to less than one unit of the visual analog scale, which limits its clinical significance. Nonetheless, any benefit in terms of pain control for patients should not be overlooked [16]. Pain due to anesthetic injection can adversely affect the cooperation of pediatric dental patients; thus, any reduction in pain is an advantage. Therefore, although the present study found no significant difference in pain score between the two techniques, within-group comparison of injection pain showed significantly higher pain score associated with IANB in the group that received IA in the first session. Also, IANB increased the HR more than IA (although insignificantly), which can be due to higher pain of IANB. Many relevant previous studies did not use physiological parameters for pain assessment. Nonetheless, the results regarding the association of HR and injection type are controversial. Recent clinical trials have reported a transient increase in HR for a few minutes following intraosseous injection of 4% articaine with epinephrine using the Quick Sleeper computer-controlled system [32] Increased HR in intraosseous injection is attributed to faster entry of catecholamines into the vascular system [33]. Some studies used Quick Sleeper and did not report any increase in HR [28, 34] or reported an insignificant short-term increase following the use of 2% lidocaine plus 1:80,000 epinephrine. The increased HR and blood pressure changes during dental procedures are due to the release of endogenous catecholamines caused by emotional stress, and not the drug side effects [35]. The higher HR following IANB injection can be attributed to greater pain. Another reason could be that the dose of epinephrine administered to children with IANB was higher than with IA, because the volume of the anesthetic agent administered with IANB injection was greater than with IA injection. In any case, the transient increase in HR would not be clinically significant in most healthy patients [36]. Within-group comparison of pain during injection showed that in the IA/IANB injection order, the pain associated with IANB was significantly higher than in IA, but in the group with the IANB/IA injection order, this difference was not significant. The authors did not find an explanation for this finding, but it may be attributed to relatively small sample size. Further studies with a larger sample size are required on this topic to cast a final judgment. According to a meta-analysis by Monteiro et al, [25] success of anesthesia is a dependent variable that is not usually evaluated in clinical studies related to local anesthesia in children and adolescents. In the present study, the efficacy and success of the two techniques were evaluated by examining the HR during treatment, recording the FLACC behavioral scale during treatment, recording the WBPRS at the end of treatment, and the need for supplemental injections during pulpotomy treatment. The mean HR of children in the two techniques did not differ significantly at the time of pulp exposure during pulpotomy, and both groups had the highest difference in HR at the time of injection, and the lowest difference at the time of entering the pulp. Also, the mean HR was not significantly different at baseline and at the time of entering the pulp in the two groups, which indicates the comfort of the child and the effectiveness of both types of injections. Moreover, the pain reported by children after pulpotomy treatment using the WBPRS did not differ significantly in the two injection types. Within-group assessment of this scale after pulpotomy treatment revealed no difference between the two injection techniques. On the other hand, the pain recorded by the FLACC scale by the observer during pulpotomy treatment did not differ significantly in the two types of injections. This finding confirms lack of difference in efficacy between the two types of injections. The lack of need for supplemental injections during pulpotomy treatment indicates the effectiveness of both anesthetic injections. Similar to the present study, AlRaddadi et al. [34] showed no difference in effectiveness of infiltration anesthesia and intraosseous injection in pulpotomy of mandibular primary teeth. In the study by Prol Castelo et al. [29] similar to the present study, the need for supplemental injections, pain during treatment, and the child's behavior during treatment did not differ between IA and IANB injections. The effectiveness of IA and IANB injections by tooth type was also analyzed in this study. According to the FLACC scale and the need for supplemental injections, there was no statistically significant difference between Ds and Es. This result is reasonable because pulpal anesthesia of one quadrant of the mandible is achieved with IANB; although sometimes additional injections are required in some areas. Also, since intraosseous injections cause anesthesia of 3 adjacent teeth in the mandible by injecting half of the cartridge in the distal bone of the respective tooth [12], there is probably no difference in pulpal anesthesia of Ds and Es considering their anatomical location. The authors did not find similar studies on the effectiveness and pain of intraosseous injections versus conventional injections by tooth type to compare our results with.
This study had some limitations. Due to the difference in appearance of the Sleeper One5 device and the conventional syringe, it was not possible to blind the operator and children. Computerized injection systems have a learning curve. Before the study onset, the operator was trained on how to use the Sleeper One5 device, but the role of experience in using such technologies cannot be ignored. The high cost of the device, the need for a special needle, and the longer injection time are among the disadvantages of this device. Future studies are suggested to measure the level of anxiety of children before the procedure and compare the two types of anesthesia techniques in terms of the time to anesthesia, duration of anesthesia, and complications after the injection. Another limitation of this study was that we did not evaluate the minimal clinically important difference (MCID) for the FLACC and WBPRS pain scales. While statistical significance was assessed, interpretation of pain outcomes would be more meaningful if related to established MCID thresholds. As MCID values provide insight into whether observed differences are clinically relevant to patients, future studies should incorporate MCID and effect size analyses to strengthen the clinical interpretation of findings. This study compared 2 types of anesthesia techniques for pulpotomy treatment of mandibular primary molars in 30 cooperative 4–6-year-old children referred to Shahid Beheshti Dental School, which may affect the generalizability of the findings to other dental treatments and injections, other age groups, non-cooperative children, and different communities. Future studies with a larger sample size are required in other age groups, comparing different dental treatments and injections, and in different communities. Studies on non-cooperative children are also recommended.
Conclusion
The research results showed that IA administered by a CCLAD may be used as an alternative to IANB for pulpotomy of primary molars, due to comparable efficacy and injection pain, as shown by the HR, and self-reported and behavioral measures.
Type of Study: Randomized Clinical Trial |
Subject:
pediatric
References
1. Dentistry AAoP. Behavior guidance for the paediatric dental patient. The reference manual of pediatric dentistry Chicago: American Academy of Pediatric Dentistry. 2021.
2. Furgała D, Markowicz K, Koczor-Rozmus A, Zawilska A. Causes and severity of dentophobia in Polish adults-A questionnaire study. Healthcare (Basel). 2021 Jun;9(7):819. [DOI:10.3390/healthcare9070819] [PMID] []
3. Schmoeckel J, Mustafa Ali M, Wolters P, Santamaría RM, Usichenko TI, Splieth CH. Pain perception during injection of local anesthesia in pedodontics. Quintessence Int. 2021 Jul;52(8):706-12.
4. Pozos-Guillén A, Loredo-Cruz E, Esparza-Villalpando V, Martínez-Rider R, Noyola-Frías M, Garrocho-Rangel A. Pain and anxiety levels using conventional versus computer-controlled local anesthetic systems in pediatric patients: A meta-analysis. J Clin Pediatr Dent. 2020 Dec;44(6):371-99. [DOI:10.17796/1053-4625-44.6.1] [PMID]
5. American Academy of Pediatric Dentistry. Use of local anesthesia for pediatric dental patients. The reference manual of pediatric dentistry. 2020:332-7.
6. Bagher SM, Felemban OM, Alsabbagh GA, Aljuaid NA. The effect of using a camouflaged dental syringe on children's anxiety and behavioral pain. Cureus. 2023 Dec;15(12):e50023. [DOI:10.7759/cureus.50023]
7. Garcia J, Kratunova E, Shah A, Zhang IL, Marion I, da Fonseca MA, et al. Articaine infiltration versus lidocaine inferior alveolar nerve block for primary mandibular molars: A double-blind randomized controlled clinical trial. Pediatr Dent. 2023 Jul;45(4):299-306.
8. Aquilanti L, Mascitti M, Togni L, Contaldo M, Rappelli G, Santarelli A. A systematic review on nerve-related adverse effects following mandibular nerve block anesthesia. Int J Environ Res Public Health. 2022 Jan;19(3):1627. [DOI:10.3390/ijerph19031627] [PMID] []
9. Bagattoni S, D'Alessandro G, Gatto MR, Piana G. Self-induced soft-tissue injuries following dental anesthesia in children with and without intellectual disability. A prospective study. Eur Arch Paediatr Dent. 2020 Oct;21(5):617-22. [DOI:10.1007/s40368-019-00506-9] [PMID]
10. Altan H, Belevcikli M, Coşgun A, Demir O. Comparative evaluation of pain perception with a new needle-free system and dental needle method in children: a randomized clinical trial. BMC Anesthesiol. 2021 Dec;21(1):301. [DOI:10.1186/s12871-021-01524-1] [PMID] []
11. Anil Ö, Keskin G. Comparison of computer controlled local anesthetic delivery and traditional injection regarding disruptive behaviour, pain, anxiety and biochemical parameters: a randomized controlled trial. J Clin Pediatr Dent. 2024 Jan;48(1):120-7.
12. Feridoz J, Raj JD. Intraosseous anesthesia in dentistry-A review. Drug Invent Today. 2018 Oct;10.
13. Carugo N, Paglia L, Re D. Pain perception using a computer-controlled anaesthetic delivery system in paediatric dentistry: A review. Eur J Paediatr Dent. 2020 Sep;21(3):180-2.
14. Janik K, Niemczyk W, Peterek R, Rój R, Balicz A, Morawiec T. Computer-controlled local anaesthesia delivery efficacy - a literature review. Saudi Dent J. 2024 Aug;36(8):1066-71. [DOI:10.1016/j.sdentj.2024.05.012] [PMID] []
15. Libonati A, Nardi R, Gallusi G, Angotti V, Caruso S, Coniglione F, et al. Pain and anxiety associated with computer-controlled local anaesthesia: systematic review and meta-analysis of cross-over studies. Eur J Paediatr Dent. 2018 Dec;19(4):324-32.
16. Smaïl-Faugeron V, Muller-Bolla M, Sixou JL, Courson F. Evaluation of intraosseous computerized injection system (QuickSleeper™) vs conventional infiltration anaesthesia in paediatric oral health care: A multicentre, single-blind, combined split-mouth and parallel-arm randomized controlled trial. Int J Paediatr Dent. 2019 Sep;29(5):573-84. [DOI:10.1111/ipd.12494] [PMID]
17. Henedy SS, Khalil AM, Mahmoud SH, El-Habashy LM. The effect of different parenting styles on the child behavior during the dental visit: observational longitudinal study. BMC Oral Health. 2025 Mar;25(1):342. [DOI:10.1186/s12903-025-05659-2] [PMID] []
18. Alovisi M, Baldi A, Comba A, Gamerro R, Paolone G, Mandurino M, et al. Long-term evaluation of pulp vitality preservation in direct and indirect pulp capping: A retrospective clinical study. J Clin Med. 2024 Jul;13(13):3962. [DOI:10.3390/jcm13133962] [PMID] []
19. DENTAL HI TEC QuickSleeper5 User Manual. Available at: https://www.manualslib.com/manual/1658548/Dental-Hi-Tec-Quicksleeper5.html.
20. Shekhar S, Suprabha BS, Shenoy R, Rao A, Rao A. Effect of active and passive distraction techniques while administering local anaesthesia on the dental anxiety, behaviour and pain levels of children: a randomised controlled trial. Eur Arch Paediatr Dent. 2022 Jun;23(3):417-27. [DOI:10.1007/s40368-022-00698-7] [PMID] []
21. Nagarwal P, Rana V, Srivastava N, Kaushik N, Pruthi T. Reliability of three pain assessment tools in children requiring dental treatment: A comparative clinical study. J Indian Soc Pedod Prev Dent. 2023 Apr-Jun;41(2):126-32. [DOI:10.4103/jisppd.jisppd_132_23] [PMID]
22. Pizzinato A, Liguoro I, Pusiol A, Cogo P, Palese A, Vidal E. Detection and assessment of postoperative pain in children with cognitive impairment: A systematic literature review and meta-analysis. Eur J Pain. 2022 May;26(5):965-79. [DOI:10.1002/ejp.1936] [PMID] []
23. Deshpande N, Jadhav A, Bhola N, Gupta M. Anesthetic efficacy and safety of 2% lidocaine hydrochloride with 1:100,000 adrenaline and 4% articaine hydrochloride with 1:100,000 adrenaline as a single buccal injection in the extraction of maxillary premolars for orthodontic purposes. J Dent Anesth Pain Med. 2020 Aug;20(4):233-40. [DOI:10.17245/jdapm.2020.20.4.233] [PMID] []
24. Serdar CC, Cihan M, Yücel D, Serdar MA. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem Med (Zagreb). 2021 Feb;31(1):010502. [DOI:10.11613/BM.2021.010502] [PMID] []
25. Monteiro J, Tanday A, Ashley PF, Parekh S, Alamri H. Interventions for increasing acceptance of local anaesthetic in children and adolescents having dental treatment. Cochrane Database Syst Rev. 2020 Feb;2(2):CD011024. [DOI:10.1002/14651858.CD011024.pub2] [PMID]
26. Shi D, Ye T. Behavioral carry-over effect and power consideration in crossover trials. Biometrics. 2024 Mar;80(2):ujae023. [DOI:10.1093/biomtc/ujae023] [PMID] []
27. Shekhar V, Choudhary N, Rathore P, Singh SP, Bhatnagar S. Non-invasive objective markers to measure pain: A direction to develop a pain device - A narrative review. Indian J Palliat Care. 2023 Apr-Jun;29(2):217-22. [DOI:10.25259/IJPC_257_2022] [PMID] []
28. AlRaddadi ZA, AlHowaish LA, Sulimany AM. Pain-related behavior and pain perception associated with intraosseous local anesthesia (QuickSleeper 5®) in pediatric patients: A randomized controlled clinical trial. Children (Basel). 2025 Jan;12(1):65. [DOI:10.3390/children12010065] [PMID] []
29. Prol Castelo A, García Mato E, Varela Aneiros I, Sande López L, Outumuro Rial M, Abeleira Pazos MT, et al. Evaluation of intraligamentous and intraosseous computer-controlled anesthetic delivery systems in pediatric dentistry: A randomized controlled trial. Children (Basel). 2022 Dec;10(1):79. [DOI:10.3390/children10010079] [PMID] []
30. Dixit A, Randhawa RK, Randhawa GS, Solanki P, Takvani R, Vaghela I. Comparative analysis of local anesthetic techniques for pain management in pediatric dental procedures: A randomized clinical trial. J Pharm Bioallied Sci. 2024 Feb;16(Suppl 1):S196-8. [DOI:10.4103/jpbs.jpbs_454_23] [PMID] []
31. Dixit UB, Joshi AV. Efficacy of intraosseous local anesthesia for restorative procedures in molar incisor hypomineralization-affected teeth in children. Contemp Clin Dent. 2018 Sep;9(Suppl 2):S272-7. [DOI:10.4103/ccd.ccd_252_18] [PMID] []
32. Vatankhah M, Dianat O, Zargar N, Bejestani SG, Baghban AA, Shojaeian S. Efficacy of QuickSleeper intraosseous injection of 4% articaine in mandibular first molars with symptomatic irreversible pulpitis: A randomized controlled trial. Anesth Prog. 2024 Sep;71(3):123-30. [DOI:10.2344/363591] [PMID] []
33. Mathison M, Pepper T. Local Anesthesia Techniques in Dentistry and Oral Surgery. 2023 Jun 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan.
34. AlRaddadi ZA, AlHowaish LA, Sulimany AM. Effectiveness of intraosseous local anesthesia (QuickSleeper 5) during pulpotomy and stainless steel crown placement on mandibular primary molars: A crossover randomized controlled clinical trial. Children (Basel). 2025 Feb;12(3):294. [DOI:10.3390/children12030294] [PMID] []
35. Zhang D, Li S, Zhang R. Effects of dental anxiety and anesthesia on vital signs during tooth extraction. BMC Oral Health. 2024 May;24(1):632. [DOI:10.1186/s12903-024-04404-5] [PMID] []
36. Turan Y, Senirkentli GB, Cekmen N, Tirali E, Çakmak E. Retrospective evaluation of the effects of local anesthesia before tooth extraction procedures under general anesthesia on physiologic parameters and postoperative bleeding in children. Niger J Clin Pract. 2024 Jun;27(6):723-31. [DOI:10.4103/njcp.njcp_708_23] [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |