Journal of Research in Dental
and Maxillofacial Sciences
Volume 11, Issue 1 (3-2026)
J Res Dent Maxillofac Sci 2026, 11(1): 57-65 |
Back to browse issues page
Ethics code: IR.AJAUMS.REC.1400.280
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hosseinipour Z S, Bozhneh M, Hosseini Z. Effects of Commonly Consumed Pediatric Medications and Drinks on Color Stability of Two Types of Composite Resins: Packable and Bulk-Fill. J Res Dent Maxillofac Sci 2026; 11 (1) :57-65
URL: http://jrdms.dentaliau.ac.ir/article-1-1042-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-1042-en.html


1- Department of Pediatric Dentistry, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran.
2- Dentist, Private Practice, Tehran, Iran
3- Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran & Department of Pediatric Dentistry, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran ,zhosseini@tums.ac.ir
2- Dentist, Private Practice, Tehran, Iran
3- Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran & Department of Pediatric Dentistry, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran ,
Full-Text [PDF 302 kb]
(54 Downloads)
| Abstract (HTML) (74 Views)
Full-Text: (17 Views)
Abstract
Background and Aim: Composite resins are widely used in pediatric dentistry, but their color stability may be affected by medications and drinks. Since packable and bulk-fill composites differ in composition, this study aimed to compare their color stability after exposure to commonly consumed pediatric medications and drinks.
Materials and Methods: In this in vitro study, disc-shaped specimens were fabricated from a packable and a bulk-fill composite resin (n=64 from each). After initial spectrophotometric color assessment, the discs underwent pH-cycling. Next, each group was divided into 8 subgroups (n=8) for immersion in distilled water (control), orange juice, chocolate milk, amoxicillin, metronidazole, acetaminophen, iron drop, and multi-vitamin syrup for 2 minutes every 8 hours for one week. The color of the specimens was then assessed again spectrophotometrically, and their color change (ΔE) was calculated. Data were analyzed by t-test, one-way ANOVA, and Tukey’s test (alpha=0.05).
Results: The two composite types had no significant difference in ΔE (P=0.733). The discoloration caused by metronidazole, amoxicillin, iron drop, and multivitamin syrup was clinically unacceptable (> 3 units). The discoloration caused by different materials was significantly different within each of the two composite groups (P=0.001), such that metronidazole yielded the highest, and distilled water yielded the lowest ΔE.
Conclusion: The research results showed that both packable and bulk-fill composite resins experienced comparable discoloration after exposure to different materials, with no significant difference between the two composite types. The results also showed that metronidazole produced the highest discoloration, while distilled water caused the lowest.
Keywords: Acetaminophen; Amoxicillin; Color; Composite Resins; Metronidazole
Introduction
Facial attractiveness is an important parameter in social acceptance and occupational success [1]. Increased demand for tooth-colored dental restorations along with the existing concerns regarding the mercury content of amalgam led to the growing use of composite resins [2]. Composite resins soon gained increasing popularity due to their ability to micromechanically bond to tooth structure, excellent esthetics, optimal resistance, affordability, easy use, and reinforcement of tooth structure [3]. Different types of composite resins with variable shades and colors are available, and extensively used in pediatric dentistry.
Packable composite resins have a higher viscosity than the previous generation of composite resins, and were introduced in the late 1990 as a replacement for amalgam for tooth-colored posterior restorations. The handling of packable composite resins is similar to that of amalgam; they are stiffer and less sticky than the conventional composite resins, enabling their easier application and handling [4]. These high-density composite resins enable faster application, and provide tighter and more favorable interproximal contacts in Class II restorations, compared with the conventional composite resins [5].
Despite excellent primary esthetic results of composite resins, they often undergo discoloration over time following clinical use in the oral environment [6]. Discoloration of composite resins is the main reason for their replacement [7]. Color stability of composite resins is an important factor in their longevity [8].
Since their advent in 1960, the composition of composite resins has greatly improved, leading to their enhanced esthetics, mechanical properties, and clinical service [9]. Stress generation due to polymerization shrinkage, and limited depth of cure of 2 mm are the main drawbacks of conventional composite resins [10]. To overcome such problems, the oblique incremental technique is often adopted, which involves application of composite resin in 2 mm-thick increments [11]. Accordingly, separate light-polymerization of each increment decreases the overall polymerization shrinkage stresses. Nonetheless, this technique is time-consuming and susceptible to void formation. Also, it may leave some uncured or partially-cured areas, if not performed properly, which can decrease the restoration strength, prevent optimal sealing, and lead to postoperative tooth hypersensitivity, and eventual restoration failure [12].
To overcome such shortcomings, bulk-fill composite resins were introduced, which can be applied in one thick layer of 4-10 mm, expediting the procedure and decreasing its technical sensitivity [12]. Bulk-fill composite resins can be divided into two groups: low-viscosity materials which are applied as a base and require an additional covering layer of composite, and high-viscosity materials to fill the cavity [13].
To improve esthetics or physical properties of restorations, all bulk-fill composite resins may be coated with a layer of conventional composite resin [12]. Dual-cure bulk-fill composite resins are also available. They benefit from both light-cure and chemical-cure technologies such that the restoration surface can be light-cured for polishing while deep areas undergo chemical polymerization over time [12].
Success of composite restorations highly depends on their color stability in the long-term [14]. Optimal color stability ensures optimal esthetics, and eliminates the need for repeated replacements, the associated costs, and additional treatment sessions required, which is particularly important in pediatric dentistry [14].
Perceptible discoloration of restorative materials compromises esthetics, and is a major reason for replacement of anterior composite restorations [3, 15]. The degree of discoloration often varies from one patient to another, depending on oral hygiene status, diet, smoking status, and consumption of different drinks [15], as well as the brand and composition of composite resin used [16]. The discoloration susceptibility of resin-based restorative materials depends on intrinsic (e.g., composition of resin matrix, filler content, size of filler particles, and two-phase nature of composite resins) and extrinsic (e.g., type of colorant and duration of exposure) factors [17, 18]. Hydrophilicity of materials also plays a role in this respect [19]. Some medications and many of the consumed drinks can cause discoloration and staining of teeth and restorations, such as iron drops and multivitamin syrups, depending on their composition [20].
Considering all the above, and given that packable and bulk-fill composites differ in filler content, curing depth, and viscosity, this study aimed to assess and compare the effects of commonly consumed pediatric medications and drinks on the color stability of a packable composite (Beautifil II A1 shade; Shofu Dental, Kyoto, Japan) and a bulk-fill composite (Beautifil-Bulk; Shofu Dental, Kyoto, Japan) under simulated oral conditions.
Materials and Methods
This in vitro experimental study was conducted on a packable composite resin (Beautifil II A1 shade; Shofu Dental, Kyoto, Japan) and a bulk-fill composite resin (Beautifil-Bulk; Shofu Dental, Kyoto, Japan). The study protocol was approved by the ethics committee of the university (IR.AJAUMS.REC.1400.280).
Sample size:
The sample size was calculated using the following standard formula for comparing two means:
n = 2 × (Zα/2 + Zβ)² × σ² / δ²
Where n is the number of specimens per group, σ is the standard deviation, and δ is the expected difference in means, considering α = 0.05 and β = 0.2 (power = 80%). The values for σ and δ were adopted from a previous study [21]. Accordingly, a minimum of 8 specimens per group were required.
Specimen preparation:
Disc-shaped specimens with 6 mm diameter and 4 mm thickness were fabricated from each of the packable and bulk-fill composite resins (n = 64 per type). Composite resin was applied in cylindrical plastic molds. Transparent Mylar strips (Henry Schein Inc., Melville, NY, USA) were positioned beneath and on top of each mold, and the mold was compressed between two glass slabs (Corning Inc., NY, USA) with gentle pressure to extrude excess material. Light curing was then performed from the top and bottom surfaces for 40 seconds using a LED curing unit (LED.D curing light; Guilin Woodpecker Medical Instrument Co., Ltd., Guangxi, China) at an intensity of 1000 mW/cm², verified with a radiometer. The specimens were removed from the molds, and stored in distilled water at 37°C for 24 hours to complete the polymerization process. The upper surfaces were then polished sequentially with 800-, 1000-, and 1500-grit silicon carbide abrasive papers (3M ESPE, St. Paul, MN, USA) under water irrigation.
Baseline color assessment:
The specimens then underwent colorimetry using a spectrophotometer (Ci6x; X-rite, MI, USA). The CIE L*a*b* color space was used for color assessment. The L* parameter indicates lightness, the a* parameter indicates redness-greenness, and the b* parameter indicates yellowness-blueness. The spectrophotometer was calibrated with a standard white tile before each measurement, and all measurements were made in triplicate; the mean values were calculated and recorded.
pH cycling:
For pH cycling, the specimens were immersed in a demineralizing solution composed of calcium chloride (CaCl₂; Merck, Darmstadt, Germany), ammonium phosphate [(NH₄)₂HPO₄; Merck, Darmstadt, Germany], and acetic acid (CH₃COOH; Merck, Darmstadt, Germany) adjusted to a pH of 4.8 for 8 hours, followed by immersion in a remineralizing solution containing CaCl₂, NaH₂PO₄, and KCl (all from Merck, Darmstadt, Germany) adjusted to a pH of 7 for 16 hours. The specimens in each composite group were then randomly assigned to eight subgroups (n=8). Two control groups were also considered by immersion of packable and bulk-fill composite specimens in distilled water. This demineralization/remineralization cycle was performed daily to simulate the natural cycles of the oral environment and thereby increase the clinical relevance of the experiment [21].
Intervention:
Next, 15 mL of each solution was prepared, including amoxicillin syrup (Dana Pharmaceutical Co., Tabriz, Iran), metronidazole suspension (Alborz Darou Co., Tehran, Iran), acetaminophen syrup (Kharazmi Pharmaceutical Co., Tehran, Iran), iron drop (Kimiasalamat Pharmaceutical Co., Zanjan, Iran), multivitamin syrup (Hakimantebkar Pharmaceutical Co., Tehran, Iran), orange juice (Sunich Co., Saveh, Iran), chocolate milk (Mihan Dairy Co., Tehran, Iran), and distilled water (Osvah Co., Tehran, Iran). Coded specimens of each subgroup were immersed in the respective solutions for 2 minutes every 8 hours with gentle agitation [21]. This process was repeated for one week for all solutions. After each immersion, the specimens were rinsed with distilled water for 5 minutes, brushed with a soft toothbrush (Oral-B; Procter & Gamble, Cincinnati, OH, USA) for 15 seconds, and dried with a clean tissue. Between the immersion cycles, the specimens were stored in artificial saliva at 37°C to simulate oral conditions [21].
Secondary color assessment:
The color parameters of the specimens were spectrophotometrically assessed again after immersion using a spectrophotometer (Ci6x; X-Rite, Grand Rapids, MI, USA). The measurements were made in triplicate. The change in L*, a*, and b* parameters after the immersion compared with baseline was calculated, and the following formula was used to calculate the overall color change (ΔE):
ΔE = [(L2− L1)2 + (a2 − a1)2 + (b2 − b1)2]1/2
The obtained ΔE values were quantified according to the National Bureau of Standards (NBS) to simulate the clinical setting using the following formula:
NBS Units = ΔE × 0.92
The clinically acceptable ΔE according to the NBS is < 3.0 [22, 23].
The device was recalibrated before each session according to the manufacturer’s instructions.
Statistical analysis:
Data were analyzed using SPSS version 25 (SPSS Inc., IL, USA). Normal distribution of data was confirmed by the Shapiro-Wilk test (P>0.05). Thus, independent student t-test was applied to compare the ΔE values between the packable and bulk-fill composite resins. Also, ΔE of each composite type was compared following exposure to different solutions using ANOVA followed by pairwise comparisons with the Tukey’s test. P<0.05 was considered statistically significant.
Results
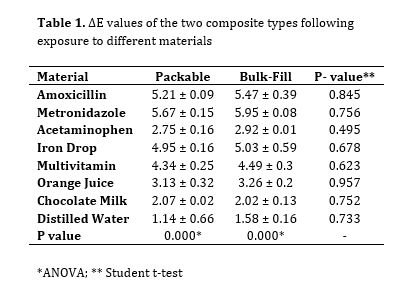
Table 1 presents the ΔE values of the two composite types following exposure to different solutions. As shown, although the bulk-fill composite experienced a slightly higher discoloration, the difference between the two composite types was not significant for any solution (P=0.733).
The discoloration caused by metronidazole, amoxycillin, iron drop, and multivitamin syrup was not clinically acceptable according to the NBS (>3 units). However, the discoloration caused by orange juice, acetaminophen, and chocolate milk was clinically acceptable (<3 units).
Table 1. ΔE values of the two composite types following exposure to different materials
Within-group comparison of ΔE values revealed significant differences in both bulk-fill (P=0.001) and packable (P=0.001) composite resins, such that metronidazole caused the highest and distilled water yielded the lowest ΔE. Based on post-hoc assessment, distilled water caused a significantly lower discoloration compared to amoxicillin, metronidazole, iron drop, and multivitamin (P<0.05). Among the tested solutions, metronidazole yielded the highest ΔE, followed by amoxicillin and iron drop. These groups had statistically significant differences with acetaminophen, orange juice, chocolate milk, and distilled water (P<0.05). Conversely, chocolate milk and distilled water caused the least discoloration.
Discussion
This study assessed the effects of commonly consumed pediatric medications and drinks on color stability of packable and bulk-fill composite resins. The results showed that the two composite types had no significant difference in ΔE, although the discoloration of bulk-fill composite was slightly higher than that of packable composite resin. This finding was in agreement with the results of Tüzüner et al [24]. Insignificantly higher ΔE of bulk-fill compared with packable composite resin may be explained by the fact that the capacity of the resin matrix for water sorption is determined by the filler volume percentage relative to the restoration volume. Thus, materials with a lower filler content and a higher resin matrix content have a higher water sorption [25]. Bulk-fill composite resins have a slightly lower filler content than packable composite resins, which increases their water sorption [26]. Discoloration of composite resins depends on their resin matrix, size of filler particles, polymerization depth, and type of colorant [27].
In the present study, pH-cycling was applied to better simulate the dynamic oral environment. Dental materials are frequently exposed to alternating demineralization and remineralization cycles in the oral cavity due to daily intake of foods and drinks, salivary buffering, and plaque metabolism. Therefore, incorporating pH-cycling into the experimental protocol increases the clinical relevance of in vitro findings, and provides a more realistic assessment of the discoloration potential of pediatric medications and drinks [21,24]. The present results were also in agreement with the findings of Mundim et al, [28] who reported that although the discoloration of composite resins with a higher filler content was less than that of composite resins with a lower filler content, this difference did not reach statistical significance.
Discoloration of composite resins following exposure to different solutions may be attributed to water sorption. However, water sorption alone cannot cause significant discoloration of composite resins [29, 30]. Several explanations have been offered in this regard. The bond strength at the resin-filler interface affects water sorption because greater water sorption causes expansion and plasticization of materials, followed by the formation of microcracks; penetration of pigments into the microcracks leads to eventual staining [31]. Chemical changes in the initiator-activator system and water sorption by monomers in composite resins lead to stain penetration and subsequent discoloration [32]. It should be noted that the magnitude of water sorption does not depend merely on the monomer type. Instead, presence of different components in restorative materials probably creates an osmotic effect, affecting water sorption. Thus, water sorption is a multifactorial phenomenon [33]. Also, silanization of filler particles in resin-based composites plays an important role in discoloration since silane is hydrophilic, and enhances water sorption [34]. Therefore, discoloration of bulk-fill and packable composite resins may be attributed to their high silane content [35].
In the present study, metronidazole yielded the highest, and distilled water yielded the lowest ΔE. The pH of metronidazole syrup is 5.6 while the pH of amoxicillin syrup is 5.39 [36]. The viscosity of metronidazole is 1194.0 cP while the viscosity of amoxicillin is 1396.67 cP [37, 38]. Since they both have a high viscosity, they tend to remain on the tooth surface for a longer period of time, and have a slower rate of wash out by the saliva, leading to enamel and restoration surface erosion [39]. The erosive effect of drinks can also affect their staining potential [19]. Safe colorants used in the composition of medicinal syrups may be absorbed by the resin component of composites, affecting their color stability [40]. The percentage of sucrose is 10% in metronidazole, and 5% in amoxicillin [41]. Thus, their nocturnal dose has an adverse effect on the primary enamel and composite restorations especially since the salivary flow decreases at night. Since the primary enamel is less mineralized than the permanent enamel, it is more susceptible to complications such as caries, erosion, and staining following frequent use of medicinal syrups with a low pH and high sucrose content [41]. Acidic solutions cause surface etching, dissolve materials, and enhance staining as such [19]. Thus, higher discoloration caused by metronidazole and amoxicillin may be explained by factors such as their low pH and high viscosity. It may be stated that pH and sucrose percentage are more important factors than viscosity in discoloration, explaining insignificantly higher ΔE of metronidazole than amoxicillin. On the other hand, orange juice contains citric acid and yellow pigments. A previous study reported dissolution of fillers and degradation of the resin matrix of flowable composites following exposure to orange juice [42]. In the present study, ΔE of the orange juice group was significantly smaller than that of the metronidazole and amoxycillin groups. Despite an acidic pH, orange juice has a low viscosity. Staining by chocolate milk is due to its organic components and fatty nature. Resultantly, it is easily absorbed by the resin component, interacts with the organic matrix, and causes discoloration [43]. Nonetheless, chocolate milk has a slightly higher viscosity than orange juice and a pH of 6.9 [44], which is more alkaline than the pH of other solutions tested in this study, and may explain the obtained results.
Staining by iron drop is due to the interaction of iron with sulfide ions following bacterial activity. Different brands of iron drops have different staining potentials, depending on the iron content of each drop, acidity, etchability of the restoration surface by each drop, bacterial flora, etc. [45]. In the present study, the discoloration caused by iron drop was slightly, but not significantly, higher than that caused by multivitamin syrup.
In the present study, the discoloration caused by metronidazole, amoxicillin, iron drop, and multivitamin syrup was clinically unacceptable (>3 units), indicating that it was detectable by the naked eye. However, the discoloration caused by orange juice, acetaminophen, and chocolate milk was clinically acceptable (<3 units). Also, the discoloration caused by distilled water was clinically acceptable, similar to previous studies [18, 46]. The present results showed that the two composite types had no significant difference in ΔE, although the discoloration of bulk-fill composite was slightly higher than that of packable composite resin. However, as this study evaluated only one brand of each composite type, the findings cannot be generalized to all bulk-fill and packable composite resins. The slightly higher ΔE observed in bulk-fill composites can be attributed to their lower filler content, higher resin matrix content, and greater potential for water sorption compared to packable composites. Additionally, the presence of hydrophilic silane at the resin–filler interface and the possibility of incomplete polymerization in deeper layers contribute to their susceptibility to discoloration. On the other hand, the clinically unacceptable ΔE values observed with metronidazole, amoxicillin, iron drop, and multivitamin syrups are explained by their acidic pH, sugar content, and viscosity, which prolong contact with the material surface, promote pigment penetration, and accelerate erosion. In contrast, orange juice and chocolate milk produced lower or clinically acceptable ΔE values, likely due to their lower viscosity and more neutral pH, despite containing staining agents. These mechanistic interpretations clarify why the present results followed the observed trends.
This study had an in vitro design. The clinical oral environment cannot be well simulated in vitro. Thus, generalizability of the results to the clinical setting should be done with caution. Also, only one brand of each composite type was evaluated. Future studies on other types and brands of composite resins are recommended. Furthermore, clinical studies are required to obtain more generalizable results.
Conclusion
Materials and Methods: In this in vitro study, disc-shaped specimens were fabricated from a packable and a bulk-fill composite resin (n=64 from each). After initial spectrophotometric color assessment, the discs underwent pH-cycling. Next, each group was divided into 8 subgroups (n=8) for immersion in distilled water (control), orange juice, chocolate milk, amoxicillin, metronidazole, acetaminophen, iron drop, and multi-vitamin syrup for 2 minutes every 8 hours for one week. The color of the specimens was then assessed again spectrophotometrically, and their color change (ΔE) was calculated. Data were analyzed by t-test, one-way ANOVA, and Tukey’s test (alpha=0.05).
Results: The two composite types had no significant difference in ΔE (P=0.733). The discoloration caused by metronidazole, amoxicillin, iron drop, and multivitamin syrup was clinically unacceptable (> 3 units). The discoloration caused by different materials was significantly different within each of the two composite groups (P=0.001), such that metronidazole yielded the highest, and distilled water yielded the lowest ΔE.
Conclusion: The research results showed that both packable and bulk-fill composite resins experienced comparable discoloration after exposure to different materials, with no significant difference between the two composite types. The results also showed that metronidazole produced the highest discoloration, while distilled water caused the lowest.
Keywords: Acetaminophen; Amoxicillin; Color; Composite Resins; Metronidazole
Introduction
Facial attractiveness is an important parameter in social acceptance and occupational success [1]. Increased demand for tooth-colored dental restorations along with the existing concerns regarding the mercury content of amalgam led to the growing use of composite resins [2]. Composite resins soon gained increasing popularity due to their ability to micromechanically bond to tooth structure, excellent esthetics, optimal resistance, affordability, easy use, and reinforcement of tooth structure [3]. Different types of composite resins with variable shades and colors are available, and extensively used in pediatric dentistry.
Packable composite resins have a higher viscosity than the previous generation of composite resins, and were introduced in the late 1990 as a replacement for amalgam for tooth-colored posterior restorations. The handling of packable composite resins is similar to that of amalgam; they are stiffer and less sticky than the conventional composite resins, enabling their easier application and handling [4]. These high-density composite resins enable faster application, and provide tighter and more favorable interproximal contacts in Class II restorations, compared with the conventional composite resins [5].
Despite excellent primary esthetic results of composite resins, they often undergo discoloration over time following clinical use in the oral environment [6]. Discoloration of composite resins is the main reason for their replacement [7]. Color stability of composite resins is an important factor in their longevity [8].
Since their advent in 1960, the composition of composite resins has greatly improved, leading to their enhanced esthetics, mechanical properties, and clinical service [9]. Stress generation due to polymerization shrinkage, and limited depth of cure of 2 mm are the main drawbacks of conventional composite resins [10]. To overcome such problems, the oblique incremental technique is often adopted, which involves application of composite resin in 2 mm-thick increments [11]. Accordingly, separate light-polymerization of each increment decreases the overall polymerization shrinkage stresses. Nonetheless, this technique is time-consuming and susceptible to void formation. Also, it may leave some uncured or partially-cured areas, if not performed properly, which can decrease the restoration strength, prevent optimal sealing, and lead to postoperative tooth hypersensitivity, and eventual restoration failure [12].
To overcome such shortcomings, bulk-fill composite resins were introduced, which can be applied in one thick layer of 4-10 mm, expediting the procedure and decreasing its technical sensitivity [12]. Bulk-fill composite resins can be divided into two groups: low-viscosity materials which are applied as a base and require an additional covering layer of composite, and high-viscosity materials to fill the cavity [13].
To improve esthetics or physical properties of restorations, all bulk-fill composite resins may be coated with a layer of conventional composite resin [12]. Dual-cure bulk-fill composite resins are also available. They benefit from both light-cure and chemical-cure technologies such that the restoration surface can be light-cured for polishing while deep areas undergo chemical polymerization over time [12].
Success of composite restorations highly depends on their color stability in the long-term [14]. Optimal color stability ensures optimal esthetics, and eliminates the need for repeated replacements, the associated costs, and additional treatment sessions required, which is particularly important in pediatric dentistry [14].
Perceptible discoloration of restorative materials compromises esthetics, and is a major reason for replacement of anterior composite restorations [3, 15]. The degree of discoloration often varies from one patient to another, depending on oral hygiene status, diet, smoking status, and consumption of different drinks [15], as well as the brand and composition of composite resin used [16]. The discoloration susceptibility of resin-based restorative materials depends on intrinsic (e.g., composition of resin matrix, filler content, size of filler particles, and two-phase nature of composite resins) and extrinsic (e.g., type of colorant and duration of exposure) factors [17, 18]. Hydrophilicity of materials also plays a role in this respect [19]. Some medications and many of the consumed drinks can cause discoloration and staining of teeth and restorations, such as iron drops and multivitamin syrups, depending on their composition [20].
Considering all the above, and given that packable and bulk-fill composites differ in filler content, curing depth, and viscosity, this study aimed to assess and compare the effects of commonly consumed pediatric medications and drinks on the color stability of a packable composite (Beautifil II A1 shade; Shofu Dental, Kyoto, Japan) and a bulk-fill composite (Beautifil-Bulk; Shofu Dental, Kyoto, Japan) under simulated oral conditions.
Materials and Methods
This in vitro experimental study was conducted on a packable composite resin (Beautifil II A1 shade; Shofu Dental, Kyoto, Japan) and a bulk-fill composite resin (Beautifil-Bulk; Shofu Dental, Kyoto, Japan). The study protocol was approved by the ethics committee of the university (IR.AJAUMS.REC.1400.280).
Sample size:
The sample size was calculated using the following standard formula for comparing two means:
n = 2 × (Zα/2 + Zβ)² × σ² / δ²
Where n is the number of specimens per group, σ is the standard deviation, and δ is the expected difference in means, considering α = 0.05 and β = 0.2 (power = 80%). The values for σ and δ were adopted from a previous study [21]. Accordingly, a minimum of 8 specimens per group were required.
Specimen preparation:
Disc-shaped specimens with 6 mm diameter and 4 mm thickness were fabricated from each of the packable and bulk-fill composite resins (n = 64 per type). Composite resin was applied in cylindrical plastic molds. Transparent Mylar strips (Henry Schein Inc., Melville, NY, USA) were positioned beneath and on top of each mold, and the mold was compressed between two glass slabs (Corning Inc., NY, USA) with gentle pressure to extrude excess material. Light curing was then performed from the top and bottom surfaces for 40 seconds using a LED curing unit (LED.D curing light; Guilin Woodpecker Medical Instrument Co., Ltd., Guangxi, China) at an intensity of 1000 mW/cm², verified with a radiometer. The specimens were removed from the molds, and stored in distilled water at 37°C for 24 hours to complete the polymerization process. The upper surfaces were then polished sequentially with 800-, 1000-, and 1500-grit silicon carbide abrasive papers (3M ESPE, St. Paul, MN, USA) under water irrigation.
Baseline color assessment:
The specimens then underwent colorimetry using a spectrophotometer (Ci6x; X-rite, MI, USA). The CIE L*a*b* color space was used for color assessment. The L* parameter indicates lightness, the a* parameter indicates redness-greenness, and the b* parameter indicates yellowness-blueness. The spectrophotometer was calibrated with a standard white tile before each measurement, and all measurements were made in triplicate; the mean values were calculated and recorded.
pH cycling:
For pH cycling, the specimens were immersed in a demineralizing solution composed of calcium chloride (CaCl₂; Merck, Darmstadt, Germany), ammonium phosphate [(NH₄)₂HPO₄; Merck, Darmstadt, Germany], and acetic acid (CH₃COOH; Merck, Darmstadt, Germany) adjusted to a pH of 4.8 for 8 hours, followed by immersion in a remineralizing solution containing CaCl₂, NaH₂PO₄, and KCl (all from Merck, Darmstadt, Germany) adjusted to a pH of 7 for 16 hours. The specimens in each composite group were then randomly assigned to eight subgroups (n=8). Two control groups were also considered by immersion of packable and bulk-fill composite specimens in distilled water. This demineralization/remineralization cycle was performed daily to simulate the natural cycles of the oral environment and thereby increase the clinical relevance of the experiment [21].
Intervention:
Next, 15 mL of each solution was prepared, including amoxicillin syrup (Dana Pharmaceutical Co., Tabriz, Iran), metronidazole suspension (Alborz Darou Co., Tehran, Iran), acetaminophen syrup (Kharazmi Pharmaceutical Co., Tehran, Iran), iron drop (Kimiasalamat Pharmaceutical Co., Zanjan, Iran), multivitamin syrup (Hakimantebkar Pharmaceutical Co., Tehran, Iran), orange juice (Sunich Co., Saveh, Iran), chocolate milk (Mihan Dairy Co., Tehran, Iran), and distilled water (Osvah Co., Tehran, Iran). Coded specimens of each subgroup were immersed in the respective solutions for 2 minutes every 8 hours with gentle agitation [21]. This process was repeated for one week for all solutions. After each immersion, the specimens were rinsed with distilled water for 5 minutes, brushed with a soft toothbrush (Oral-B; Procter & Gamble, Cincinnati, OH, USA) for 15 seconds, and dried with a clean tissue. Between the immersion cycles, the specimens were stored in artificial saliva at 37°C to simulate oral conditions [21].
Secondary color assessment:
The color parameters of the specimens were spectrophotometrically assessed again after immersion using a spectrophotometer (Ci6x; X-Rite, Grand Rapids, MI, USA). The measurements were made in triplicate. The change in L*, a*, and b* parameters after the immersion compared with baseline was calculated, and the following formula was used to calculate the overall color change (ΔE):
ΔE = [(L2− L1)2 + (a2 − a1)2 + (b2 − b1)2]1/2
The obtained ΔE values were quantified according to the National Bureau of Standards (NBS) to simulate the clinical setting using the following formula:
NBS Units = ΔE × 0.92
The clinically acceptable ΔE according to the NBS is < 3.0 [22, 23].
The device was recalibrated before each session according to the manufacturer’s instructions.
Statistical analysis:
Data were analyzed using SPSS version 25 (SPSS Inc., IL, USA). Normal distribution of data was confirmed by the Shapiro-Wilk test (P>0.05). Thus, independent student t-test was applied to compare the ΔE values between the packable and bulk-fill composite resins. Also, ΔE of each composite type was compared following exposure to different solutions using ANOVA followed by pairwise comparisons with the Tukey’s test. P<0.05 was considered statistically significant.
Results
Table 1 presents the ΔE values of the two composite types following exposure to different solutions. As shown, although the bulk-fill composite experienced a slightly higher discoloration, the difference between the two composite types was not significant for any solution (P=0.733).
The discoloration caused by metronidazole, amoxycillin, iron drop, and multivitamin syrup was not clinically acceptable according to the NBS (>3 units). However, the discoloration caused by orange juice, acetaminophen, and chocolate milk was clinically acceptable (<3 units).
Table 1. ΔE values of the two composite types following exposure to different materials
{kind=link}
Within-group comparison of ΔE values revealed significant differences in both bulk-fill (P=0.001) and packable (P=0.001) composite resins, such that metronidazole caused the highest and distilled water yielded the lowest ΔE. Based on post-hoc assessment, distilled water caused a significantly lower discoloration compared to amoxicillin, metronidazole, iron drop, and multivitamin (P<0.05). Among the tested solutions, metronidazole yielded the highest ΔE, followed by amoxicillin and iron drop. These groups had statistically significant differences with acetaminophen, orange juice, chocolate milk, and distilled water (P<0.05). Conversely, chocolate milk and distilled water caused the least discoloration.
Discussion
This study assessed the effects of commonly consumed pediatric medications and drinks on color stability of packable and bulk-fill composite resins. The results showed that the two composite types had no significant difference in ΔE, although the discoloration of bulk-fill composite was slightly higher than that of packable composite resin. This finding was in agreement with the results of Tüzüner et al [24]. Insignificantly higher ΔE of bulk-fill compared with packable composite resin may be explained by the fact that the capacity of the resin matrix for water sorption is determined by the filler volume percentage relative to the restoration volume. Thus, materials with a lower filler content and a higher resin matrix content have a higher water sorption [25]. Bulk-fill composite resins have a slightly lower filler content than packable composite resins, which increases their water sorption [26]. Discoloration of composite resins depends on their resin matrix, size of filler particles, polymerization depth, and type of colorant [27].
In the present study, pH-cycling was applied to better simulate the dynamic oral environment. Dental materials are frequently exposed to alternating demineralization and remineralization cycles in the oral cavity due to daily intake of foods and drinks, salivary buffering, and plaque metabolism. Therefore, incorporating pH-cycling into the experimental protocol increases the clinical relevance of in vitro findings, and provides a more realistic assessment of the discoloration potential of pediatric medications and drinks [21,24]. The present results were also in agreement with the findings of Mundim et al, [28] who reported that although the discoloration of composite resins with a higher filler content was less than that of composite resins with a lower filler content, this difference did not reach statistical significance.
Discoloration of composite resins following exposure to different solutions may be attributed to water sorption. However, water sorption alone cannot cause significant discoloration of composite resins [29, 30]. Several explanations have been offered in this regard. The bond strength at the resin-filler interface affects water sorption because greater water sorption causes expansion and plasticization of materials, followed by the formation of microcracks; penetration of pigments into the microcracks leads to eventual staining [31]. Chemical changes in the initiator-activator system and water sorption by monomers in composite resins lead to stain penetration and subsequent discoloration [32]. It should be noted that the magnitude of water sorption does not depend merely on the monomer type. Instead, presence of different components in restorative materials probably creates an osmotic effect, affecting water sorption. Thus, water sorption is a multifactorial phenomenon [33]. Also, silanization of filler particles in resin-based composites plays an important role in discoloration since silane is hydrophilic, and enhances water sorption [34]. Therefore, discoloration of bulk-fill and packable composite resins may be attributed to their high silane content [35].
In the present study, metronidazole yielded the highest, and distilled water yielded the lowest ΔE. The pH of metronidazole syrup is 5.6 while the pH of amoxicillin syrup is 5.39 [36]. The viscosity of metronidazole is 1194.0 cP while the viscosity of amoxicillin is 1396.67 cP [37, 38]. Since they both have a high viscosity, they tend to remain on the tooth surface for a longer period of time, and have a slower rate of wash out by the saliva, leading to enamel and restoration surface erosion [39]. The erosive effect of drinks can also affect their staining potential [19]. Safe colorants used in the composition of medicinal syrups may be absorbed by the resin component of composites, affecting their color stability [40]. The percentage of sucrose is 10% in metronidazole, and 5% in amoxicillin [41]. Thus, their nocturnal dose has an adverse effect on the primary enamel and composite restorations especially since the salivary flow decreases at night. Since the primary enamel is less mineralized than the permanent enamel, it is more susceptible to complications such as caries, erosion, and staining following frequent use of medicinal syrups with a low pH and high sucrose content [41]. Acidic solutions cause surface etching, dissolve materials, and enhance staining as such [19]. Thus, higher discoloration caused by metronidazole and amoxicillin may be explained by factors such as their low pH and high viscosity. It may be stated that pH and sucrose percentage are more important factors than viscosity in discoloration, explaining insignificantly higher ΔE of metronidazole than amoxicillin. On the other hand, orange juice contains citric acid and yellow pigments. A previous study reported dissolution of fillers and degradation of the resin matrix of flowable composites following exposure to orange juice [42]. In the present study, ΔE of the orange juice group was significantly smaller than that of the metronidazole and amoxycillin groups. Despite an acidic pH, orange juice has a low viscosity. Staining by chocolate milk is due to its organic components and fatty nature. Resultantly, it is easily absorbed by the resin component, interacts with the organic matrix, and causes discoloration [43]. Nonetheless, chocolate milk has a slightly higher viscosity than orange juice and a pH of 6.9 [44], which is more alkaline than the pH of other solutions tested in this study, and may explain the obtained results.
Staining by iron drop is due to the interaction of iron with sulfide ions following bacterial activity. Different brands of iron drops have different staining potentials, depending on the iron content of each drop, acidity, etchability of the restoration surface by each drop, bacterial flora, etc. [45]. In the present study, the discoloration caused by iron drop was slightly, but not significantly, higher than that caused by multivitamin syrup.
In the present study, the discoloration caused by metronidazole, amoxicillin, iron drop, and multivitamin syrup was clinically unacceptable (>3 units), indicating that it was detectable by the naked eye. However, the discoloration caused by orange juice, acetaminophen, and chocolate milk was clinically acceptable (<3 units). Also, the discoloration caused by distilled water was clinically acceptable, similar to previous studies [18, 46]. The present results showed that the two composite types had no significant difference in ΔE, although the discoloration of bulk-fill composite was slightly higher than that of packable composite resin. However, as this study evaluated only one brand of each composite type, the findings cannot be generalized to all bulk-fill and packable composite resins. The slightly higher ΔE observed in bulk-fill composites can be attributed to their lower filler content, higher resin matrix content, and greater potential for water sorption compared to packable composites. Additionally, the presence of hydrophilic silane at the resin–filler interface and the possibility of incomplete polymerization in deeper layers contribute to their susceptibility to discoloration. On the other hand, the clinically unacceptable ΔE values observed with metronidazole, amoxicillin, iron drop, and multivitamin syrups are explained by their acidic pH, sugar content, and viscosity, which prolong contact with the material surface, promote pigment penetration, and accelerate erosion. In contrast, orange juice and chocolate milk produced lower or clinically acceptable ΔE values, likely due to their lower viscosity and more neutral pH, despite containing staining agents. These mechanistic interpretations clarify why the present results followed the observed trends.
This study had an in vitro design. The clinical oral environment cannot be well simulated in vitro. Thus, generalizability of the results to the clinical setting should be done with caution. Also, only one brand of each composite type was evaluated. Future studies on other types and brands of composite resins are recommended. Furthermore, clinical studies are required to obtain more generalizable results.
Conclusion
The research results showed that the packable and bulk-fill composite resins tested in this study exhibited comparable discoloration following exposure to different pediatric medications and drinks, with no significant difference between them. Among the tested solutions, metronidazole caused the highest discoloration in both composite types.
Type of Study: Original article |
Subject:
Restorative Dentistry
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |