

Volume 8, Issue 1 (1-2023)
J Res Dent Maxillofac Sci 2023, 8(1): 57-61 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gupta G, Gupta D K, Gupta P, Rana K S, Chandra N. An Unusual Odontogenic Keratocyst Associated with Third Molar Crypt Near Condyle in an
Adolescent: A Case Report. J Res Dent Maxillofac Sci 2023; 8 (1) :57-61
URL: http://jrdms.dentaliau.ac.ir/article-1-444-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-444-en.html



1- Department of Pediatric and Preventive Dentistry, Jaipur Dental College, Private practice at Wisdom Dental Clinics, Jaipur, Rajasthan, India , dr.gauravgupta99@gmail.com
2- Department of Oral and Maxillofacial Surgery, RUHS College of Dental Sciences, Wisdom Dental Clinics, Jaipur, Rajasthan, India
3- RUHSCDS Govt Dental College, Jaipur, Rajasthan, India
4- Department of Conservative Dentistry and Endodontics, Government College of Dentistry, Indore, India
5- Department of Periodontics, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India
2- Department of Oral and Maxillofacial Surgery, RUHS College of Dental Sciences, Wisdom Dental Clinics, Jaipur, Rajasthan, India
3- RUHSCDS Govt Dental College, Jaipur, Rajasthan, India
4- Department of Conservative Dentistry and Endodontics, Government College of Dentistry, Indore, India
5- Department of Periodontics, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India
Full-Text [PDF 898 kb]
(441 Downloads)
| Abstract (HTML) (772 Views)
Introduction
Odontogenic keratocysts (OKCs) are odontogenic cysts that originate from the dental lamina which First observed by Phillipsen in 1956 [1]. OKC is distinguished by its quick development, aggressive nature, and propensity to infiltrate the nearby tissues, particularly bone. It often recurs, and basal cell nevus syndrome is sometimes linked to it [2]. Specific histopathological and clinical characteristics of OKC point to a tumor rather than a cyst. OKC was identified by researchers as a benign cystic neoplasm. Multiple OKCs were first identified in Gorlin-Goltz syndrome in 1960, which also included cutaneous, skeletal, ophthalmic, and neurological abnormalities [2]. The World Health Organization classifies OKC as a benign unicystic or multicystic intraosseous tumor of odontogenic origin with parakeratinized stratified squamous epithelial lining and the potential for aggressive infiltrative behavior. The World Health Organization suggests using the term keratocystic odontogenic tumor because it more accurately shows its neoplastic nature [3,4]. Jaw lesions commonly affect the children, and their causes range from developmental anomalies to neoplasia.
Odontogenic lesions of the jaw are the most frequent in children [5,6]. Dentigerous cysts are the most common odontogenic cysts associated with an erupted or developing tooth, most typically affecting mandibular third molars; other teeth that are frequently affected include the maxillary canines, maxillary third molars, and less frequently, central incisors [7,8]. In the current case report, we describe a case of major OKC in a teenager that caused mandibular damage. This case report discusses how to handle such uncommon situations while maintaining the mandible's continuity, original dentition, form, function, and contour.
Case Presentation
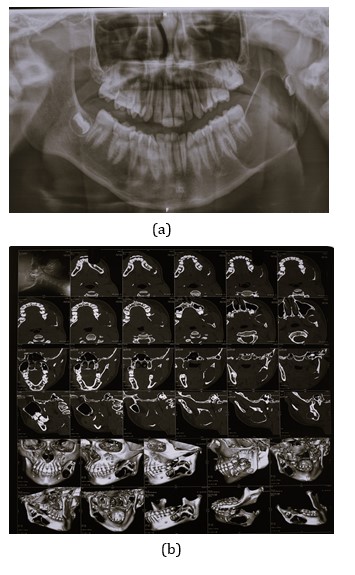
A 14-year-old patient who had been complaining of discomfort and swelling in the bottom left corner of his face for a few months was referred to our clinic. The patient had no other symptoms. An intraoral examination indicated integrity of the mucosa with mobile tooth #37 and edema in the left angle of the jaw. The patient had no prior dental or medical history. The patient underwent panoramic radiography. The third molar crypt and a well-defined radiolucent lesion were both detected on the panoramic radiograph at the left angle of the jaw with regard to teeth #36 and #37 (Figure 1a). After thorough explanation, the patient's parents signed an informed consent form on behalf of the patient. Because of the magnitude of the lesion, computed tomography (CT) was done (Figure 1b).
The CT-scan revealed that an inferiorly located lesion was connected to the mandibular first and second molars, and that
Figure 1. Preoperative Panoramic radiograph (a) and computed tomography scan (b) showing a radiolucency in the left angle of the mandible.
the crypt of the mandibular third molar was present in the ramus of the jaw close to the condyle. The left ramus was involved, and a well-defined osteolytic hypodense (5–10 HU) lesion spanning around 47 x 24 mm was identified, leading to bone growth. Cortex was intact, suggesting a benign etiology (mandibular cystic lesion). There was no sign of a soft tissue component. Under local anesthesia, the lesion was surgically removed by enucleation, followed by marsupialization and extraction of the crypts of the second and third mandibular molars (Figures 2a, b and c). A saline irrigation was performed after the extraction of tooth #37 and the third molar's crypt (Figure 2d). Iodoform dressing was applied after irrigation. For the next 10 days, the patient was recalled for periodic iodoform dressing. The specimen, which was a single cyst measuring 4 x 3 x 2 cm was obtained (Figure 2e). Its outer surface had a sleek finish. The cut surface was cystic and tan in color. The biopsy report revealed odontogenic dentigerous keratocyst instead of a benign inflammatory cystic lesion.
Figure 2. Sequence of treatment of patient:
(a) Extraction of tooth #37, (b) Extraction of 3rd molar crypt, (c) Extraction of the involved tooth, (d) Irrigation with saline, (e) Iodoform dressing application
After 6 months, the patient was recalled; neither radiolucency nor edema were seen. The patient seemed to be doing fine (Figure 3).
Figure 3. Postoperative radiograph at the six-month follow-up
Discussion
OKC is an aggressive lesion that develops from the dental lamina, while some experts speculate that it may have a basal cell origin [9]. The mandible accounts for 70% or more of OKC cases, particularly those involving the third molar, angle, and ramus. The maxillary third molar ranks next followed by mandibular premolar and maxillary canine region [10]. In comparison with radicular cysts or OKCs, dentigerous cysts have a stronger propensity to cause root resorption of neighboring teeth [11].
Cysts often grow faster in a growing youngster than they do in an adult. Lesions of 40 to 50 mm in diameter may form over a period of 3 to 4 years, yet patients may only report a history of swelling that is progressively growing [12,13]. When a cyst is infected, its boundaries may not be well defined, making it difficult to distinguish a tiny cyst from a healthy tooth follicle. Any follicular gap more than 4 mm should raise a serious concern for a dentigerous cyst, according to observations. Ameloblastoma, odontogenic keratocysts, and other odontogenic tumors, such as adenomatoid odontogenic tumor in anterior radiolucencies and ameloblastic fibroma in the posterior jaw of young patients, are included in the differential diagnosis list [14]. Cysts originate as a consequence of periapical inflammation, which generally starts in the follicles of non-vital deciduous teeth and spreads to unerupted permanent successors. Inflammatory exudates cause the reduced enamel epithelium to separate from the enamel, which leads to cyst formation. Dentigerous cysts come in two different varieties: inflammatory and developing [15]. Differential diagnoses for OKC include giant cell granuloma, dentigerous cyst, traumatic cyst, ameloblastoma, and odontogenic myxoma. Dentigerous cysts are attached to teeth at the cementoenamel junction. Traumatic cysts have unilocular, scalloped borders and seldom exhibit cortical extension [15]. The conservative methods of treating OKC, such as marsupialization and decompression, result in full clearance of the cystic lesion. They are preferred because they help protect vital structures, preserve bone and teeth, and reduce the risk of pathological fracture. The goal of the procedure is to lower the cystic osmotic pressure by exposing it to the oral cavity. It is helpful for bone deposition around the lesion's edge and for the cyst's size to gradually shrink. Segmental resection, en bloc, and complex procedures are other therapeutic options [16]. In the present case, the lesion was revealed to be related to permanent successor teeth, the mandibular third molar crypt, and was present in a 14-year-old asymptomatic and slow-growing youngster. We decided to remove the impacted teeth and lesion, followed by enucleation and marsupialization. In addition, periodic iodoform dressings were used to preserve the mandible's form, function, teeth, and contour. The six-month follow-up revealed no recurrence.
Conclusion
For general and pediatric dentists, managing odontogenic lesions in children may be difficult. A detailed grasp of the lesion's nature, supported by an excellent clinical history and cutting-edge radiography, may greatly aid physicians in making the optimal treatment decision for the patient's long-term interests. Such damaging lesions should be diagnosed and treated promptly and efficiently to prevent further damage.
Full-Text: (324 Views)
Abstract Background and Aim: A developing odontogenic cyst known as odontogenic keratocyst (OKC) originates from the remains of dental lamina. Its aggressive pattern of expansion and high recurrence rate differentiate it from other odontogenic cysts. Herein, we describe a large OKC in the mandibular ramus, close to the condyle, in a juvenile patient with a third molar crypt. Age and sex of patient, and size, location, and fast development of this lesion were different compared with previously reported OKCs. Our management strategy aimed to maintain the mandible's natural dentition, form, function, and continuity. Case Presentation: The conservative strategy of marsupialization and decompression, which results in final total clearance of the cystic lesion, is one of the treatment strategies for OKC. Segmental resection, en bloc, and complex procedures are other treatment options. Surgical enucleation of the lesion and subsequent marsupialization were conducted effectively in this case. After a lengthy follow-up, there was no recurrence. Conclusion: A detailed comprehension of the nature of the lesion supported by a strong clinical history and cutting-edge radiography may greatly aid the physician in making the appropriate treatment decision for patient's long-term interests. Key Words: Odontogenic Cysts; Mandible; Molar |
Introduction
Odontogenic keratocysts (OKCs) are odontogenic cysts that originate from the dental lamina which First observed by Phillipsen in 1956 [1]. OKC is distinguished by its quick development, aggressive nature, and propensity to infiltrate the nearby tissues, particularly bone. It often recurs, and basal cell nevus syndrome is sometimes linked to it [2]. Specific histopathological and clinical characteristics of OKC point to a tumor rather than a cyst. OKC was identified by researchers as a benign cystic neoplasm. Multiple OKCs were first identified in Gorlin-Goltz syndrome in 1960, which also included cutaneous, skeletal, ophthalmic, and neurological abnormalities [2]. The World Health Organization classifies OKC as a benign unicystic or multicystic intraosseous tumor of odontogenic origin with parakeratinized stratified squamous epithelial lining and the potential for aggressive infiltrative behavior. The World Health Organization suggests using the term keratocystic odontogenic tumor because it more accurately shows its neoplastic nature [3,4]. Jaw lesions commonly affect the children, and their causes range from developmental anomalies to neoplasia.
Odontogenic lesions of the jaw are the most frequent in children [5,6]. Dentigerous cysts are the most common odontogenic cysts associated with an erupted or developing tooth, most typically affecting mandibular third molars; other teeth that are frequently affected include the maxillary canines, maxillary third molars, and less frequently, central incisors [7,8]. In the current case report, we describe a case of major OKC in a teenager that caused mandibular damage. This case report discusses how to handle such uncommon situations while maintaining the mandible's continuity, original dentition, form, function, and contour.
Case Presentation
A 14-year-old patient who had been complaining of discomfort and swelling in the bottom left corner of his face for a few months was referred to our clinic. The patient had no other symptoms. An intraoral examination indicated integrity of the mucosa with mobile tooth #37 and edema in the left angle of the jaw. The patient had no prior dental or medical history. The patient underwent panoramic radiography. The third molar crypt and a well-defined radiolucent lesion were both detected on the panoramic radiograph at the left angle of the jaw with regard to teeth #36 and #37 (Figure 1a). After thorough explanation, the patient's parents signed an informed consent form on behalf of the patient. Because of the magnitude of the lesion, computed tomography (CT) was done (Figure 1b).
The CT-scan revealed that an inferiorly located lesion was connected to the mandibular first and second molars, and that
Figure 1. Preoperative Panoramic radiograph (a) and computed tomography scan (b) showing a radiolucency in the left angle of the mandible.
{kind=link}
the crypt of the mandibular third molar was present in the ramus of the jaw close to the condyle. The left ramus was involved, and a well-defined osteolytic hypodense (5–10 HU) lesion spanning around 47 x 24 mm was identified, leading to bone growth. Cortex was intact, suggesting a benign etiology (mandibular cystic lesion). There was no sign of a soft tissue component. Under local anesthesia, the lesion was surgically removed by enucleation, followed by marsupialization and extraction of the crypts of the second and third mandibular molars (Figures 2a, b and c). A saline irrigation was performed after the extraction of tooth #37 and the third molar's crypt (Figure 2d). Iodoform dressing was applied after irrigation. For the next 10 days, the patient was recalled for periodic iodoform dressing. The specimen, which was a single cyst measuring 4 x 3 x 2 cm was obtained (Figure 2e). Its outer surface had a sleek finish. The cut surface was cystic and tan in color. The biopsy report revealed odontogenic dentigerous keratocyst instead of a benign inflammatory cystic lesion.
Figure 2. Sequence of treatment of patient:
{kind=link}
(a) Extraction of tooth #37, (b) Extraction of 3rd molar crypt, (c) Extraction of the involved tooth, (d) Irrigation with saline, (e) Iodoform dressing application
After 6 months, the patient was recalled; neither radiolucency nor edema were seen. The patient seemed to be doing fine (Figure 3).
Figure 3. Postoperative radiograph at the six-month follow-up
{kind=link}
Discussion
OKC is an aggressive lesion that develops from the dental lamina, while some experts speculate that it may have a basal cell origin [9]. The mandible accounts for 70% or more of OKC cases, particularly those involving the third molar, angle, and ramus. The maxillary third molar ranks next followed by mandibular premolar and maxillary canine region [10]. In comparison with radicular cysts or OKCs, dentigerous cysts have a stronger propensity to cause root resorption of neighboring teeth [11].
Cysts often grow faster in a growing youngster than they do in an adult. Lesions of 40 to 50 mm in diameter may form over a period of 3 to 4 years, yet patients may only report a history of swelling that is progressively growing [12,13]. When a cyst is infected, its boundaries may not be well defined, making it difficult to distinguish a tiny cyst from a healthy tooth follicle. Any follicular gap more than 4 mm should raise a serious concern for a dentigerous cyst, according to observations. Ameloblastoma, odontogenic keratocysts, and other odontogenic tumors, such as adenomatoid odontogenic tumor in anterior radiolucencies and ameloblastic fibroma in the posterior jaw of young patients, are included in the differential diagnosis list [14]. Cysts originate as a consequence of periapical inflammation, which generally starts in the follicles of non-vital deciduous teeth and spreads to unerupted permanent successors. Inflammatory exudates cause the reduced enamel epithelium to separate from the enamel, which leads to cyst formation. Dentigerous cysts come in two different varieties: inflammatory and developing [15]. Differential diagnoses for OKC include giant cell granuloma, dentigerous cyst, traumatic cyst, ameloblastoma, and odontogenic myxoma. Dentigerous cysts are attached to teeth at the cementoenamel junction. Traumatic cysts have unilocular, scalloped borders and seldom exhibit cortical extension [15]. The conservative methods of treating OKC, such as marsupialization and decompression, result in full clearance of the cystic lesion. They are preferred because they help protect vital structures, preserve bone and teeth, and reduce the risk of pathological fracture. The goal of the procedure is to lower the cystic osmotic pressure by exposing it to the oral cavity. It is helpful for bone deposition around the lesion's edge and for the cyst's size to gradually shrink. Segmental resection, en bloc, and complex procedures are other therapeutic options [16]. In the present case, the lesion was revealed to be related to permanent successor teeth, the mandibular third molar crypt, and was present in a 14-year-old asymptomatic and slow-growing youngster. We decided to remove the impacted teeth and lesion, followed by enucleation and marsupialization. In addition, periodic iodoform dressings were used to preserve the mandible's form, function, teeth, and contour. The six-month follow-up revealed no recurrence.
Conclusion
For general and pediatric dentists, managing odontogenic lesions in children may be difficult. A detailed grasp of the lesion's nature, supported by an excellent clinical history and cutting-edge radiography, may greatly aid physicians in making the optimal treatment decision for the patient's long-term interests. Such damaging lesions should be diagnosed and treated promptly and efficiently to prevent further damage.
Type of Study: Case report |
Subject:
Oral & maxillofacial surgery
References
1. Neville BW. Oral and Maxillofacial Pathology. 3rd ed. St. Louis: Mosby, Elsevier; 2009.
2. Parikh NR. Nonsyndromic multiple odontogenic keratocysts: Report of case. Journal of Advanced Dental Research. 2010;2(1):71-4. [DOI:10.1177/2229411220100111]
3. Rajkumar CG, Hemalath M, Shashikala R, Sonal P. Massive keratocystic odontogenic tumor of the mandible: A case report and review of literature. Indian J Dent Res. 2011; 22: 181, 205-9. [DOI:10.4103/0970-9290.80000] [PMID]
4. Madras J, Lapointe H. Keratocystic odontogenic tumour: Reclassification of odontogenic keratocyst to tumour. J Can Dent Assoc. 2008; 74:165-165h.
5. Altini M, Cohen MJ. Experimental extra-follicular histogenesis of follicular cysts. J Oral Pathol 1987(16)49-52. [DOI:10.1111/j.1600-0714.1987.tb00686.x] [PMID]
6. Bhat S. Radicular cyst associated with endodontically treated deciduous tooth: A case report. J Indian Soc Pedo Prev Dent. 2001; 19:21-23.
7. Kusukawa J, Irie K, Morimatsu M, Koyanagi S, Kameyama T. Dentigerous cyst associated with a deciduous tooth. Oral Surg Oral Med Oral Pathol. 1992; 73:415-18. [DOI:10.1016/0030-4220(92)90317-J] [PMID]
8. Hasbini AS, Hadi U, Ghafari J. Endoscopic removal of an ectop-ic third molar obstructing the osteomeatal complex. Ear Nose Throat J. 2001; 80:667-70. [DOI:10.1177/014556130108000912] [PMID]
9. Khalam AS, Zacariah RK. Under diagnosis of an odontogenic keratocyst-a controversial lesion. IOSR J Dent Med Sci. 2012(2):37-40. [DOI:10.9790/0853-0253740]
10. Shear M. Dentigerous (follicular) cyst. In: Wright (ed). Cysts of the oral regions (3rd ed). Oxford: Pergamon Press 1992:75-98.
11. Seward G. Treatment of cysts. In: Shear M (Ed). Cysts of the oral regions (3rd ed). Oxford: Wright 1992:227-56.
12. Seward G. Radiology in general dental practice. London: British Dental Association 1964:154-61. [DOI:10.1111/j.1834-7819.1964.tb02683.x]
13. Daley TD, Wysocki GP. The small dentigerous cyst. A diagnostic dilemma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:77-81. [DOI:10.1016/S1079-2104(05)80078-2] [PMID]
14. Garg S, Sunil MK, Trivedi A, Singla N. Odontogenic keratocyst of the angle and ramus of the mandible-a case report. J Dent Spec. 2015(3)195-8. [DOI:10.5958/2393-9834.2015.00020.0]
15. Almeida P Jr., Cardoso LC, Garcia IR Jr., Magro-Filho O, Luvi-zuto ER, Felipini RC. Conservative approach to the treatment of keratocystic odontogenic tumor. J Dent Child (Chic). 2010(77)135-9.
16. Kshirsagar RA, Bhende RC, Raut PH, Mahajan V, Tapadiya VJ, Singh V. Odontogenic keratocyst: Developing a protocol for surgical intervention. Ann Maxillofac Surg. 2019(9):152-7. [DOI:10.4103/ams.ams_137_18] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
