

Volume 7, Issue 4 (10-2022)
J Res Dent Maxillofac Sci 2022, 7(4): 241-248 |
Back to browse issues page


Ethics code: A-10-893-1
Clinical trials code: 8963
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khalili M, Farazmehr K, Shafaeefard S, Irani F. Effect of Paracetamol and Magnesium Sulfate on Level of Pain and Opioid Intake following
Orthognathic Surgery: A Clinical Trial. J Res Dent Maxillofac Sci 2022; 7 (4) :241-248
URL: http://jrdms.dentaliau.ac.ir/article-1-372-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-372-en.html



1- Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
2- Department of Anesthesiology and Critical Care, Faculty of Medicine, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran , Shahroozshafaeefard@gmail.com
4- Private Dentistry practice, Tehran, Iran
2- Department of Anesthesiology and Critical Care, Faculty of Medicine, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
3- Department of Oral & Maxillofacial Surgery, Faculty of Dentistry, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran , Shahroozshafaeefard@gmail.com
4- Private Dentistry practice, Tehran, Iran
Full-Text [PDF 715 kb]
(523 Downloads)
| Abstract (HTML) (1285 Views)
Full-Text: (318 Views)
| Abstract
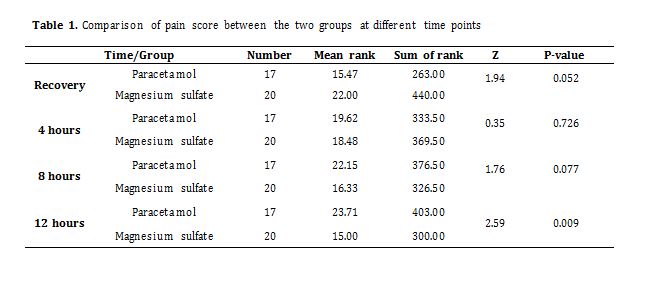
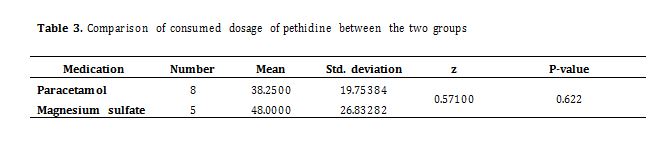
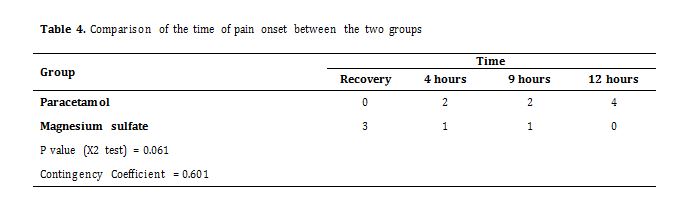
Background and Aim: Considering the side effects of high doses of opioids taken postoperatively for pain control, paracetamol and magnesium sulfate may be able to aid in pain control. This study assessed the effects of paracetamol and magnesium sulfate on the level of pain and opioid intake following orthognathic surgery. Materials and Methods: In this double-blind randomized clinical trial, patients scheduled for bimaxillary orthognathic surgery were randomly assigned to two groups of 25. Group 1 patients received 1 g infusion of intravenous acetaminophen (paracetamol) administered within 20 minutes while group 2 patients received 50 mg/kg magnesium sulfate infusion one hour prior to completion of surgery. The patients were asked to express their level of pain prior to discharge from the recovery, and every 4 hours for 12 hours using a visual analog scale (VAS). Patients with pain score > 5 at any time received 30 mg pethidine. The total received dosage of pethidine postoperatively was recorded and those that received pethidine were not included in pain score analysis. Data were analyzed by generalized estimating equation (GEE), and Mann-Whitney U, Chi-square, and t-tests. Results: The pain score was not significantly different between the two groups at the time of recovery and 4 and 8 hours (P>0.05). The magnesium sulfate group had significantly lower pain score at 12 hours (P=0.009). The difference in pethidine dosage was not significant (P>0.05). Conclusion: Both magnesium sulfate and paracetamol decreased postoperative pain and the need for opioid consumption, but magnesium sulfate was slightly more effective. Key Words: Acetaminophen; Magnesium Sulfate; Analgesics, Opioid; Orthognathic Surgery; Pain Introduction Pain is among the most important irritating post-surgical complications [1]. Pain management is an inseparable part of postoperative patient care [2]. Management of acute and chronic pain is an important priority. In the past, opioids were the cornerstone of pain reduction. Premedication with opioids is commonly performed in general anesthesia, and is continued perioperatively. However, considering their side effects such as nausea, vomiting, itching, and respiratory depression, attempts are ongoing to find non-opioid alternatives to decrease the administration of opioids [3]. Pain after orthognathic surgery is due to clinical problems related to masticatory muscles or temporomandibular joint such as muscle spasm in the head and neck, and maxillofacial region, and extensive manipulation of muscles and bones [4]. Nerve injury during orthognathic surgery can also result in orofacial or musculoskeletal pain [5]. Mobini et al. [6] evaluated pain after orthognathic surgery and the need for opioid intake, and reported a mean pain score of 6 according to a visual analog scale (VAS), which was relatively severe. Also, patients who underwent bimaxillary surgery or mandibular surgery had higher level of pain than those who only underwent maxillary surgery, and required higher doses of opioids. Thus, it is imperative to find a strategy to decrease the level of pain after orthognathic surgery while lowering the dosage of opioids by finding an efficient alternative. Acetaminophen is a relatively safe medication with insignificant side effects and limited contraindications. It does not have considerable interference with other medications [7]. Paracetamol is the injection form of acetaminophen (50 mL acetaminophen). Its onset of action starts immediately after injection, its effect quickly reaches its peak, and remains for 2 to 3 hours in adults. Magnesium sulfate (50% Infu-magnesol; 50 mL) is injected intravenously, its onset of action occurs within 1-2 minutes, its effect quickly reaches its peak, and remains for 30 minutes. It is a physiological calcium channel blocker and a non-competitive antagonist of N-methyl-D-aspartate “NMDA” receptors. Theoretically, it can play a role in part of the molecular process of sensitization, and relieve postoperative pain by blocking NMDA receptors [8]. According to a review study by Shin et al. [9], due to the pivotal function of NMDA receptors in pain transfer, the mechanism of analgesic effect of magnesium is mainly explained by its inhibitory effect on NMDA receptors and central sensitization. The analgesic efficacy of magnesium has been evaluated for different types of pain. Oral, intravenous, spinal, and epidural administration of magnesium may decrease postoperative pain and the need for analgesics. Beneficial effects of treatment with magnesium have also been reported in patients with neuropathic pain such as those with neurological symptoms due to malignancy, diabetic neuropathy, neuralgia after herpes labialis, and peripheral neuropathy due to chemotherapy. Thus, injection of magnesium is more commonly used in daily clinical practice [9,10]. Therefore, paracetamol and magnesium sulfate were selected for assessment in this study. A previous study showed that paracetamol decreased pain and the need for opioids [11] while another study reported no significant effect [12]. The reports regarding the analgesic efficacy of magnesium sulfate have also been controversial [13,14]. Mostafa et al. [15] evaluated the prophylactic effect of intravenous infusion of magnesium on postoperative sore throat after thyroid surgery and reported that it significantly decreased the incidence and severity of sore throat after thyroidectomy. Hamed and Al-Saeed [16] assessed the efficacy of intravenous magnesium sulfate versus intravenous paracetamol on pain in children after tonsillectomy and the need for analgesics and reported that magnesium sulfate had superior analgesic efficacy compared with paracetamol, and decreased the need for analgesics. However, Kalani et al. [12] compared the analgesic effects of paracetamol and magnesium sulfate on pain during surgery and found that although administration of narcotics decreased by the use of paracetamol and magnesium sulfate, this reduction was not significant. Another study by Talebi et al. [7] evaluated the effect of intravenous acetaminophen (paracetamol) administration on pain intensity and opioid consumption by patients undergoing radius shaft fracture surgery and reported that it had a significant effect on opioid consumption during and after surgery; however, the difference in pain scores was not significant between the two groups at any time point. Considering the abovementioned controversy, this study aimed to assess and compare the effects of magnesium sulfate and paracetamol on pain and opioid consumption in patients undergoing orthognathic surgery in Bouali Hospital in Tehran during 2019-2021. Materials and Methods This double-blind prospective randomized clinical trial (ethical code: IR.IAU.DENTAL.REC.1398.005, IRCT code: IRCT20201113049375N1) was conducted on 50 male and female patients between 18-45 years who were candidates for bimaxillary orthognathic surgery, were ASA class 1 or 2 according to the American Society of Anesthesiologists, did not have a history of previous orthognathic surgery, did not have drug allergy, substance abuse, or alcohol consumption, were not using psychedelic medications, had no hepatic or renal disease, did not have major anemia or arrhythmia, were not under chronic treatment with corticosteroids, calcium channel blockers, or non-steroidal anti-inflammatory drugs, and were willing to patriciate in the study and signed informed consent forms. Emergency cases and those with multiple facial trauma were excluded. The patients were randomly divided into two groups of 25. After 8 hours of fasting, the patients underwent standard monitoring of SPO2, ETCO2, ECG, and NIBP (Non-invasive blood pressure). After obtaining a venous access, 500 mL of saline was administered prior to anesthesia induction. The patients were pre-oxygenated with 100% oxygen for a minimum of 5 minutes, and after receiving premedication with 0.03 mg/kg midazolam and 3 mic/kg fentanyl, anesthesia was induced by 1.5-2 mg/kg propofol; 0.5 mg/kg atracurium as muscle relaxant was also administered and the patients were intubated. Patients were ventilated in both groups and ETCO2 was precisely controlled by capnography to prevent hypo- or hypercarbia. Anesthesia maintenance was the same in both groups with continuous infusion of 2% sevoflurane and 0.5 mg/kg atracurium every 20-30 minutes and N2O + O2 with 50/50 ratio. In both groups, 0.1 mg/kg morphine sulfate was infused within 20 minutes one hour after the onset of surgery. Vital signs were recorded every 30 minutes. Urinary output, bleeding, and the volume of consumed crystalloids perioperatively were recorded. Approximately 1 hour prior to termination of surgery when screws were fixed in the mandible and prior to suturing of the maxilla and mandible, intravenous acetaminophen (paracetamol, 1 g; Apotel; Alborz Daru) was infused within 20 minutes in group A. In group B, 50 mg/kg magnesium sulfate (50 mL; 50% Infu-magnesol, Shahid Ghazi, Tabriz) was infused within 20 minutes one hour prior to termination of surgery. Hypotension or reduction of heart rate were treated in case of occurrence. After termination of surgery and after returning of spontaneous respiration of patients, the effects of muscle relaxant were reversed by 0.2 mg/kg atropine and 0.04 mg/kg neostigmine and nerve stimulator to ensure no residual muscle relaxation. After extubation, the patients were transferred to the recovery room. The vital signs were checked every 15 minutes, and when the patients acquired a score > 9 according to the modified Aldrete scoring system, they were discharged to the ward. After discharge, the patients were asked about their level of pain using a 0-10 visual analog scale (VAS) with 0 indicating no pain and 10 indicating most severe pain experienced. The patients were asked about pain every 4 hours up to 12 hours postoperatively, and the total dose of pethidine injected in the first 12 hours postoperatively was recorded. In case of pain (VAS > 5) at any time after discharge to the ward, 30 mg pethidine was gradually infused intravenously. Patients who received pethidine at any time within the first 12 hours postoperatively were excluded from the pain comparisons, and were separately compared regarding the dosage of pethidine received between the two groups of Apotel and magnesium sulfate. In case of postoperative nausea or vomiting, 4 mg ondansetron was gradually injected intravenously within 10 minutes. The level of pain was recorded at the time of recovery, and at 4, 8 and 12 hours using a VAS, and recorded. The frequency of opioid intake was also recorded during this period. Table 1. Comparison of pain score between the two groups at different time points The Mann-Whitney U test and generalized estimation equation (GEE) were applied to compare the level of pain at each time point between the two groups, and over time. T-test and Mann-Whitney U test were also used to compare opioid intake between the two groups. The time of onset of severe pain was compared between the two groups by the Chi-square test. Results Comparison of pain score between the two groups: Table 1 compares the pain score between the two groups at different time points. The Mann-Whitney test showed no significant difference in the pain score between the two groups at the time of recovery, 4 hours and 8 hours (P>0.05). However, this difference was significant at 12 hours, and the mean pain score was significantly lower in magnesium sulfate group (P<0.05). The GEE model was then applied to assess the interaction effect of time and medication on pain score over time (Table 2). The results showed that the effect of type of medication on pain score was significant over time (P<0.05). Pain score did not experience a significant change over time (P>0.05). The interaction effect of time and medication on pain score was significant (P<0.05). Comparison of consumed dosage of pethidine: To compare the consumed dosage of pethidine between the two groups, the mean and standard deviation values were reported and the results were analyzed by the Mann-Whitney U test due to small sample size in each group. The results showed no significant difference in this regard between the two groups (Table 3). Time of pain onset: The coefficient of agreement and Chi-square test were applied and showed no significant difference between the two groups in time of onset of severe pain. The agreement coefficient, however, showed a good level of agreement between the two groups (Table 4). Time of severe pain onset had no significant correlation with type of received medication (P>0.05). Table 2. GEE model Table 3. Comparison of consumed dosage of pethidine between the two groups Table 4. Comparison of the time of pain onset between the two groups Discussion In this study, which was conducted on 50 patients undergoing orthognathic surgery, 13 had severe pain (VAS > 5), indicating the optimal analgesic efficacy of paracetamol and magnesium sulfate and subsequently decreased need for pethidine. Comparison of the mean pain score between the two groups indicated no significant difference at the time of recovery and 4 and 8 hours. However, at 12 hours, the pain score was significantly lower in magnesium sulfate group. No significant difference was found regarding the consumed dosage of pethidine between the two groups. Also, time of severe pain onset had no significant correlation with type of received medication. Other relevant studies mainly evaluated one type of medication for other surgical procedures. Some studies reported that paracetamol decreased the pain score and the need for analgesic intake [11,17] while some others found no significant effect [12]. The reports regarding the analgesic efficacy of magnesium sulfate have been controversial [13,18-20]. Mostafa et al. [15] evaluated the prophylactic effect of intravenous infusion of magnesium on postoperative sore throat after thyroid surgery. They evaluated 80 female patients in two groups of 30 mg/kg magnesium sulfate (test) and isotonic saline (control). The incidence of postoperative sore throat was 75% in the control group and 37.5% in the test group. This difference was significant. They concluded that magnesium sulfate significantly decreased the incidence and severity of postoperative sore throat after thyroidectomy. Magnesium sulfate also showed optimal analgesic efficacy in the present study. Hamed and Al-Saeed [16] assessed the efficacy of intravenous magnesium sulfate versus intravenous paracetamol on pain in children after tonsillectomy and the need for analgesics. They evaluated 60 children between 3 to 12 years in two groups of magnesium sulfate and paracetamol infusion. A nurse evaluated analgesia by observing the face, feet, activity, crying, bleeding, and sedation of patients. Rectal diclofenac sodium (12.5 mg) was administered in case of severe pain. They reported that magnesium sulfate had significantly superior analgesic efficacy compared with paracetamol, and significantly decreased the need for analgesics. The difference in bleeding and sedation was not significant. They compared two medications similar to the present study; however, they did not exclude patients who received diclofenac, while we excluded patients who received pethidine from the comparison of pain to obtain more accurate results. Kalani et al. [12] compared the analgesic effects of paracetamol and magnesium sulfate on pain during surgery. They evaluated 60 patients in three groups of paracetamol, magnesium sulfate, and control. Although the VAS pain score was higher in the control group at 6, 12, and 18 hours, postoperatively, this difference was not significant. In the present study, only patients undergoing orthognathic surgery were included, since type of surgery and its degree of difficulty can affect postoperative pain. Kalani et al. [12] found that although administration of narcotics decreased by the use of paracetamol and magnesium sulfate, this reduction was not significant. Memis et al. [11] evaluated the efficacy of intravenous paracetamol for reduction of opioid dose, extubation time, and opioid side effects in intubated patients in the ICU. They evaluated 40 patients in two groups of 1 g intravenous paracetamol every 6 hours, and 100 cc saline. The paracetamol group showed lower dosage of administered opioids, earlier extubation, and lower rate of opioid complications. In the present study, a small number of patients required pethidine, indicating that both medications decreased the need for opioids but the difference between the two groups was not significant. Hwang et al. [21] evaluated the efficacy of magnesium sulfate infusion during spinal anesthesia for postoperative pain reduction. They administered a bolus dose of 50 mg/kg, and reported significantly lower pain score at 4, 24, and 48 hours postoperatively in magnesium sulfate group. The present results were in line with their findings. Koing et al. [22] administered 50 mg/kg bolus dose magnesium sulfate followed by infusion of 8 mg/kg/h. The results showed no significant difference in VAS score postoperatively between the control and magnesium sulfate groups but the rate of consumption of opioids was lower in magnesium sulfate group. They only evaluated magnesium sulfate in their study, while we compared two medications and found a significant difference between them. In the present study, the interaction effect of time and medication on pain score was significant. But no significant correlation was found between time of pain onset and type of medication. However, the authors also witnessed that patients who received paracetamol did not have severe pain in the recovery but later experienced severe pain over time. Thus, it may be concluded that although paracetamol was effective in pain reduction early after surgery, its efficacy decreased with time, and patients in this group experienced greater pain over time than the magnesium sulfate group. Considering the trend of change in pain, we noticed that some patients had slightly higher pain score in magnesium sulfate group, which may also be due to the effects of intubation and shivering after regaining consciousness (which can be mistaken for pain). However, the trend of change in pain score was descending over time, indicating its long-term successful analgesic effects. Also, number of patients in magnesium sulfate group who required pethidine was lower (although not significantly). Conclusion It may be concluded that despite the relative success of both magnesium sulfate and paracetamol in pain control and reduction of opioids, it appears that magnesium sulfate was slightly more successful, and can be recommended for oral and maxillofacial surgical procedures, and particularly orthognathic surgery. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Type of Study: Randomized Clinical Trial |
Subject:
Oral & maxillofacial surgery
References
1. Shakeri M R, Derakhshan P, Sheykholvaezin F, Koleini Z. The comparison between postoperative analgesic effect of Morphine-Apotel and Ketorolac alone with intravenous patient control analgesia in patients candidate for plating surgery. JAP. 2016;7(2):1-8.
2. Sanjar Mousavi N, Khalili R. The effect of intravenous injection of Acetaminophen (Apothec) on pain relief after abdominoplasty. Journal of Islamic Azad University Mashhad Branch. 2014; 4(1):1-17.
3. Atef A, Fawaz AA. Intravenous paracetamol is highly effective in pain treatment after tonsillectomy in adults. Eur Arch Otorhinolaryngol. 2008 Mar;265(3):351-5. [DOI:10.1007/s00405-007-0451-5] [PMID]
4. Nitzan D W, Dolwick M F. Temporomandibular joint fibrous ankylosis following orthognathic surgery: report of eight cases. International Journal of Adult Orthodontics and Orthognathic Surgery. 1989;4(1):7-11.
5. Kim Y K. Complications associated with orthognathic surgery. J Korean Assoc Oral Maxillofac Surg. 2017;43(1):3-15. [DOI:10.5125/jkaoms.2017.43.1.3] [PMID] [PMCID]
6. Mobini A, Mehra P, Chigurupati R. Postoperative Pain and Opioid Analgesic Requirements After Orthognathic Surgery. J Oral Maxillofac Surg. 2018 Nov;76(11):2285-95. [DOI:10.1016/j.joms.2018.05.014] [PMID]
7. Talebi H, Kamali A, l Moshiri E, yazdi B, Hosseini M. Efficacy of intravenous acetaminophen injection on pain intensity and opioid consumption in patients undergoing radius shaft fracture surgery. JAP. 2014; 5(3):64-72.
8. James MF. Clinical use of magnesium infusions in anesthesia. Anesth Analg. 1992 Jan;74(1):129-36. [DOI:10.1213/00000539-199201000-00021] [PMID]
9. Shin HJ, Na HS, Do SH. Magnesium and Pain. Nutrients. 2020 Jul 23;12(8):2184. [DOI:10.3390/nu12082184] [PMID] [PMCID]
10. Miller RD. Miller's Anesthesia. 7 th ed. Philadelphia: Churchill livingstone/Elsevier;2010. 3312 p.
11. Memis D, Inal MT, Kavalci G, Sezer A, Sut N, et al. Intravenous paracetamol reduced the use of opioids, extubation time, and opioid-related adverse effects after major surgery in intensive care unit. J Crit Care. 2010 Sep; 25 (3):458-62. [DOI:10.1016/j.jcrc.2009.12.012] [PMID]
12. Kalani N, Sanie MS, Zabetian H, Radmehr M, Sahraei R, Kargar Jahromi H. Comparison of the Analgesic Effect of Paracetamol and Magnesium Sulfate during Surgeries. World J Plast Surg. 2016 Sep;5(3):280-6.
13. Davoudi M, Tahmasebi R, Zolhavareih S M. Evaluation of the Effect of Intravenous Magnesium Sulfate on Post-operative Pain after Cesarean Section under Spinal Anesthesia. Avicenna J Clin Med. 2013; 19(4):20-6.
14. Xie M, Li XK, Peng Y. Magnesium sulfate for postoperative complications in children undergoing tonsillectomies: A systematic review and meta-analysis. J Evid Based Med. 2017;10:16-25. [DOI:10.1111/jebm.12230] [PMID]
15. Mostafa RH, Saleh AN, Ibrahim IM. The prophylactic effect of intravenous magnesium infusion on postoperative sore throat after thyroid surgery. A randomized clinical trial. Rev Chil Anest. 2020;49:528-37. [DOI:10.25237/revchilanestv49n04-09]
16. Hamed MA, Al-Saeed MA. The Efficacy of Intravenous Magnesium Sulfate versus Intravenous Paracetamol on Children Posttonsillectomy Pain and Analgesic Requirement: A Randomized Controlled Study. Anesth Essays Res. 2018 Jul-Sep;12(3):724-728. [DOI:10.4103/aer.AER_113_18] [PMID] [PMCID]
17. Damirchi AN, Kamali A, Azami M, Monfared ME. Comparison of the effect of Apotel and pregabalin on postoperative pain among patients undergoing lower limb orthopedic surgeries. J Family Med Prim Care. 2019 Jul;8(7): 2405-2408. [DOI:10.4103/jfmpc.jfmpc_396_19] [PMID] [PMCID]
18. Santhi Sree M, Usha Rani A. Efficacy of intraoperative I.v Magnesium sulfate versus Iv Paracetamol on post-operative analgesic requirement in major surgeries under general anesthesia. IOSR J Dent Med Sci (IOSR-JDMS). 2018; 17:1-11.
19. Cristalli MP, La Monaca G, De Angelis C, Pranno N, Annibali S. Efficacy of Preoperative Administration of Paracetamol-Codeine on Pain following Impacted Mandibular Third Molar Surgery: A Randomized, Split-Mouth, Placebo-Controlled, Double-Blind Clinical Trial. Pain Res Manag. 2017;2017:9246352. [DOI:10.1155/2017/9246352] [PMID] [PMCID]
20. Shin HJ, Kim EY, Na HS, Kim TK, Kim MH, Do SH. Magnesium sulphate attenuates acute postoperative pain and increased pain intensity after surgical injury in staged bilateral total knee arthroplasty: a randomized, double-blinded, placebo-controlled trial. Br J Anaesth. 2016 Oct;117(4):497-503. [DOI:10.1093/bja/aew227] [PMID]
21. Hwang JY, Na HS, Jeon YT, Ro YJ, Kim CS, Do SH. I.V. infusion of magnesium sulfate during spinal anesthesia improves postoperative analgesia. Br J Anaesth. 2010 Jan; 104(1):89-93. [DOI:10.1093/bja/aep334] [PMID]
22. Koinig H, Wallner T, Marhofer P, Andel H, Hörauf K, Mayer N. Magnesium sulfate reduces intra- and postoperative analgesic requirements. Anesth Analg. 1998 Jul;87(1):206-10. [DOI:10.1213/00000539-199807000-00042]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
