

Volume 4, Issue 3 (9-2019)
J Res Dent Maxillofac Sci 2019, 4(3): 5-14 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
MalekiGorji M, Golestaneh A. Histological Evaluation of the Effect of Sildenafil and Pentoxifylline on Mandibular Fracture Healing in Rats. J Res Dent Maxillofac Sci 2019; 4 (3) :5-14
URL: http://jrdms.dentaliau.ac.ir/article-1-259-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-259-en.html



1- Postgraduate student, department of oral and maxillofacial surgery
2- Assistant professor, department of oral and maxillofacial surgery, Islamic Azad University, Isfahan (Khorasgan) branch, Isfahan, Iran , drgolestaneh@gmail.com
2- Assistant professor, department of oral and maxillofacial surgery, Islamic Azad University, Isfahan (Khorasgan) branch, Isfahan, Iran , drgolestaneh@gmail.com
Full-Text [PDF 362 kb]
(1278 Downloads)
| Abstract (HTML) (2920 Views)
Rats in the C2 group received saline orally on a daily basis after the surgery and were sacrificed after two weeks.
Rats in the S2 group received 10 mg/kg sildenafil (Sildenafil 50 mg, Marham Daru Co., Tehran, Iran) orally via gavage daily and were sacrificed after two weeks.
Rats in the P2 group received 50 mg/kg pentoxifylline (Pentoxifylline 400 mg; Extended Release, Amin Pharmaceutical Co., Isfahan, Iran) orally via gavage daily and were sacrificed after two weeks.
The C6 (control, 6 weeks), S6 (sildenafil, 6 weeks) and P6 (pentoxifylline, 6 weeks) groups received medications as in groups C2, S2, and P2 but were sacrificed after six weeks.
The dosage of administered medications was determined according to similar previous studies. (34,36-38) Use of higher doses may cause greater vasodilation but may be associated with side effects such as hypotension, decreased tissue perfusion, and severe anti-inflammatory responses. Use of lower doses may have no effect at all. (39)
Statistical analysis:
Data were analyzed using SPSS version 22 (SPSS Inc., Chicago, IL, USA) via one-way analysis of variance (ANOVA) and Tukey’s post-hoc test to find significant differences between groups. The mean and standard deviation (SD) of the findings of the histological analysis were reported.
Results
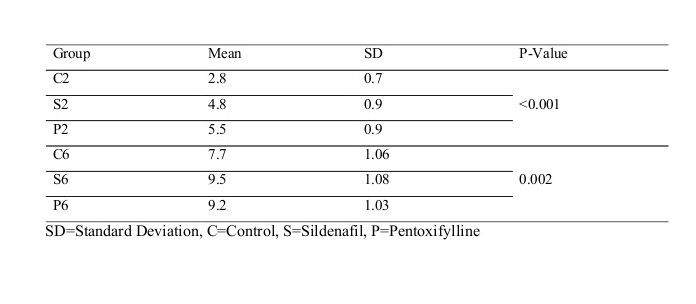
This study evaluated the effects of two phosphodiesterase inhibitors on bone healing in mandibular fractures in rats. Forty-eight rats were evaluated in six groups of eight. None of the rats expired during the study and no complication occurred. All rats well tolerated the surgical procedure. The mean rate of bone healing was 2.8±0.7, 4.8±0.9, and 5.5±0.9 in C2, S2, and P2 groups, respectively (Table 1).
Table 1: Mean and standard deviation (SD) of bone healing in mandibular fractures in the studied groups
One-way ANOVA showed that the mean rate of bone healing in mandibular fractures was significantly different among the aforementioned three groups after two weeks (P=0.0005). Tukey’s post-hoc test revealed that the mean rate of bone healing in S2 and P2 groups was significantly higher than that in the C2 group after two weeks (P=0.0005). The mean rate of bone healing in the P2 group was significantly higher than that in the S2 group after two weeks (P=0.04).
The mean rate of bone healing was 7.7±1.06, 9.5±1.08 and 9.2±1.03 in groups C6, S6, and P6, respectively (Table 1). One-way ANOVA revealed that the mean rate of bone healing was significantly different among the aforementioned three groups after 6 weeks (P=0.002). Tukey’s test revealed that the mean rate of bone healing in S6 (P=0.001) and P6 (P=0.004) groups was significantly higher than that in the C6 group after 6 weeks but no significant difference was noted between P6 and S6 groups in this respect (P=0.53).
Figure 2 shows histological images of study groups at x100 magnification.
Figure 2. Histological images of study groups at x100 magnification. (A) A specimen from the C2 group with bone healing score 3 (equal amount of fibrous and cartilage tissue). (B) A specimen from the S2 group with bone healing score 5 [mainly cartilage tissue and a small amount of immature (woven) bone]. (C) A specimen from the P2 group with bone healing score 7 [significantly immature (woven) bone and a small amount of cartilage]. (D) A specimen from the C6 group with bone healing score 8 [completely immature (woven) bone]. (E) A specimen from the S6 group with bone healing score 9 (healing with immature bone and a small amount of mature bone). (F) A specimen from the P6 group with bone healing score 10 [mature (lamellar) bone]
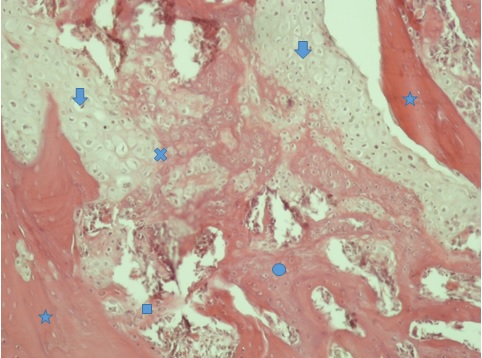
As shown in Figure 3, bone tissue can be divided into lamellar and woven bone according to its level of maturity. An eosinophilic area containing lacunae was noted in lamellar bone tissue under the microscope (marked by *), and lines confirming periodic calcification of bone could be seen. These parts were the old host bone, which were mature and seen on the two sides of the fracture line. The shorter the time duration since fracture, the less mature the tissue around the mature bone margins would be. The size and number of lacunae are also important. In areas marked with * (old bone), the number of lacunae and their size were smaller. The area marked with a circle indicates the newly forming, immature bone. This bone has a cancellous appearance and has differences with mature bone in terms of the number of lacunae (where the osteocytes are present) and their size. The area marked with a square indicates the interface of the newly formed bone and older bone. The area marked with an arrow shows the cartilage tissue. The area marked with x indicates cartilage calcification and its conversion to bone.
Figure 3. Histological image of the P2 group with bone healing score 5 (x100 magnification)
Discussion
This study assessed the effects of sildenafil and pentoxifylline on bone healing in mandibular fractures in rats. Healing of fractures is an important topic in maxillofacial surgery. The routine function of patients should be reinstated as soon as possible. (40) Many studies have evaluated this topic, (40,41) and evidence shows that the outcome of surgical procedures for treatment of fractures is influenced by several factors such as patient-related factors, type of bone defect, and type of surgical procedure. (40) Adequate blood supply plays a critical role in bone healing. (42,43) Impaired angiogenesis at the site leads to poor healing of bone. Oxygen and nutrients are delivered to the site of bone callus formation through the bloodstream. Moreover, the bloodstream delivers progenitor and inflammatory cells to the site of injury. (20,21,28) Nitric oxide and vasodilation are also imperative for angiogenesis. (44) Positive effects of nitric oxide on wound healing may be related to its functional effects on angiogenesis and inflammation. Sildenafil prevents the breakdown and degradation of nitric oxide, which leads to vasodilation and increased blood supply to the tissue. (16-18) Several studies have shown that sildenafil is effective for different pathological conditions via the nitric oxide pathway. In addition, many studies have focused on the effects of sildenafil on tissue healing. Many clinical and animal studies have shown the positive effects of sildenafil in cases of decreased blood supply to the skin and impaired vascularization as in ischemic wounds. (18,21,29) Moreover, evidence shows that enhanced bone healing by sildenafil can be due to the function of cysteine-rich angiogenic inducer 61 protein, which stimulates endothelial cell migration and induces proliferation and differentiation of osteoblasts and cell adhesion. (14,45) Pentoxifylline is a phosphodiesterase inhibitor derived from xanthine, which has a vasodilatory effect. In contrast to most peripheral vasodilators, pentoxifylline has rheological effects on blood and decreases its viscosity. (24) The therapeutic effects of pentoxifylline are mainly attributed to its potential for increasing the blood flow and oxygenation of tissues due to its hemorheological property. (25) It is not clear whether pentoxifylline increases the number of osteoblasts and osteoclasts or not. Takami et al showed that phosphodiesterase inhibitors increase the number of osteoclasts and their differentiation to osteoblasts. (46) Horiuchi et al demonstrated that pentoxifylline enhances new bone formation by upregulating the bone morphogenetic protein-2. (47,48) Tsutsumimoto et al indicated that pentoxifylline can be used to enhance bone formation. (49)
Many studies have evaluated several medications and factors to enhance bone healing and demonstrated that bone morphogenetic proteins, insulin-like growth factor 1 (IGF1), transforming growth factor B1 (TGFB1), and vitamin E can all enhance the process of bone healing. (50-53) Several studies have evaluated the effects of phosphodiesterase inhibitors on bone healing with results comparable to ours. However, no previous study evaluated the effects of sildenafil and pentoxifylline on maxillofacial fractures. (42,54,55) The current results revealed that pentoxifylline and sildenafil have positive effects on bone healing. Our findings regarding enhanced bone healing by sildenafil were in agreement with those of Yaman et al, Histing et al, and Çakir-Özkan et al. (42,19,56) Aydin et al used pentoxifylline in a dosage similar to ours and showed that pentoxifylline enhances the formation of a hematoma, which is the first phase of bone healing. (34) This result was in agreement with our findings. However, they showed that the anti-inflammatory effects of pentoxifylline might delay bone healing after 3 weeks. (34) This result was in contrast to ours. Our study showed positive effects of pentoxifylline on bone healing in the late stage. Since they evaluated femoral bone fractures, this difference in the results may be related to different rates and modes of metabolism of femoral bone and mandibular bone at the final stages of fracture healing.
Our results regarding enhanced bone healing by sildenafil were in line with those of Histing et al, (19) with the difference that they used 5 mg/kg dose of sildenafil while we used 10 mg/kg dosage according to the previously published studies. The reason behind the use of 5 mg/kg dosage of sildenafil in their study was that the speed of metabolism of sildenafil is higher in rats and sildenafil has a half-life of one hour in rats and four hours in humans. They used 5 mg/kg dosage for rats, which is 5 times the standard dosage for humans (0.7 to 1.5 mg/kg). Despite the different dosages used in the two studies, the outcomes were the same. Atalay et al used the same dosage of pentoxifylline as ours. (40) The mean histological score of bone healing in their study was 7.8 after 6 weeks while it was 9.2 in our study. This difference was probably due to the difference in defect size in the two studies. The bone gap created in their study after osteotomy was 1 mm while it was 0.5 mm in our study. In the present study, bone healing in the pentoxifylline group was significantly higher than that in the sildenafil group after two weeks but the score of bone healing in the sildenafil group was higher than that in the pentoxifylline group after six weeks. It seems that the rheological effects of pentoxifylline and reduction of blood viscosity by this medication in the first two weeks enhanced the primary phase of healing and formation of a hematoma at the site of fracture. However, the authors believe that at the end of the sixth week, the anti-inflammatory effects of pentoxifylline, similar to those of other non-steroidal anti-inflammatory drugs (NSAIDs), delay the process of bone healing. For this reason, at the end of the sixth week, the bone-healing rate in the sildenafil group was higher than that in the pentoxifylline group.
Infection also plays a role in bone healing. Aydin et al (34) showed lower bone healing rate (7.1 versus 9.2) at similar time points and with the use of the same dosage of pentoxifylline, which may be due to no use of antibiotics postoperatively in their study. As they reported, 40% of the samples in the pentoxifylline group had an infection, which seemed to slow down the process of bone healing. (34) Gong et al indicated that the use of tadalafil and vardenafil phosphodiesterase inhibitors decreased the bone mass. (57) Their study was the only one that reported results contrary to ours. This difference may be attributed to different study designs and different types of selective phosphodiesterase inhibitors used.
Despite the abovementioned studies, our knowledge about the effects of phosphodiesterase inhibitors on bone metabolism and healing is insufficient. A good understanding of the biological events that occur in the process of bone healing is imperative to find the most efficient approach to enhance bone healing. This study was the first to show the positive effects of sildenafil and pentoxifylline on healing of mandibular bone fractures. Thus, sildenafil and pentoxifylline can be used as adjuncts to enhance bone healing.
One limitation of this study was the daily use of 50 mg/kg dosage of pentoxifylline and 10 mg/kg dosage of sildenafil; thus, bone healing in response to higher and lower doses remains a matter of question. Also, due to ethical considerations, we could not employ a larger sample size. Finally yet importantly, it is not known to what extent the slight histological differences are clinically important. Clinical studies using different doses of sildenafil and pentoxifylline are required to assess bone healing at different time points. Also, similar studies are recommended on rabbits or dogs since they have higher histological and anatomical similarities with humans, and the surgical procedure of their mandible would be easier to perform. Moreover, radiographic and biomechanical assessments should be carried out in addition to histological analysis, and expression of genes involved in bone healing should be evaluated. Finally yet importantly, similar studies are required on osteoporotic mandibles, those under bisphosphonate therapy, chemotherapy, and radiotherapy to assess the efficacy of these medications to enhance bone healing in pathological conditions.
Conclusion
The results of this study showed that sildenafil and pentoxifylline can be used as adjuncts to enhance bone healing in mandibular fractures.
Full-Text: (922 Views)
Abstract
Background and Aim: Despite the advances in maxillofacial surgery, impaired bone healing remains a concern for surgical teams. Effects of sildenafil and pentoxifylline on healing of bone fractures have not been well investigated. This study aimed to assess the effects of sildenafil and pentoxifylline phosphodiesterase inhibitors on healing of mandibular fractures in rats.
Materials and Methods: In this animal study, 48 Wistar rats were randomly divided into six groups (n=8). Mandibular fracture was induced in all rats. After the surgical procedure, C2 group (control, 2 weeks) received saline, S2 group (sildenafil, 2 weeks) received 10 mg/kg sildenafil, and P2 group (pentoxifylline, 2 weeks) received 50 mg/kg pentoxifylline. The rats were sacrificed after 2 weeks. C6 (control, 6 weeks), S6 (sildenafil, 6 weeks), and P6 (pentoxifylline, 6 weeks) groups received pharmaceutical therapy as in C2, S2, and P2 but were sacrificed after 6 weeks. The samples then underwent histological analysis. Data were analyzed using SPSS 22 via one-way analysis of variance (ANOVA) and Tukey’s post-hoc test.
Results: The mean rate of healing of mandibular fractures in S2 and P2 was significantly higher than that in C2 after 2 weeks (P<0.001). The mean rate of healing of fractures in P2 was higher than that in S2 after 2 weeks (P=0.04). The mean rate of healing of fractures in S6 (P=0.001) and P6 (P=0.004) was significantly higher than that in C6 after 6 weeks but no significant difference was noted between P6 and S6 in this respect (P=0.53).
Conclusion: Sildenafil and pentoxifylline can be used as adjuncts to enhance bone healing.
Keywords: Bone Healing, Mandibular Fracture, Pentoxifylline, Sildenafil
Introduction
Successful management of maxillofacial fractures depends on correct reduction and precise fixation of broken segments to achieve a normal occlusion, resume function, and properly align the broken pieces next to each other. (1) Despite the advances in maxillofacial surgery, impaired bone healing remains a concern for surgical teams. (2) Mandibular fractures are among the most common fractures of the maxillofacial region accounting for 23% to 97% of all facial fractures. (3,4)
Bone healing is a complex process that includes three stages of inflammation, repair, and delayed remodeling. This biological process is controlled by complex cellular and molecular mechanisms. Systemic and local factors and several cell types and growth factors delivered via the adjacent tissues and bloodstream play a role in bone healing. (5-7) Several studies have evaluated growth factors, injection of medications, and electrical stimulation to accelerate and enhance bone healing. (8-10) In contrast, several studies have indicated that some medications, such as antibiotics and bisphosphonates, delay or impair the process of bone healing. By having comprehensive knowledge about these factors and not prescribing them in case of fracture, complete bone healing can be expected. (11,12) Bleeding at the site of injury is the most important factor for successful bone healing. (13) Decreased angiogenesis at the site of trauma and limited blood supply to the site are known as factors delaying or impairing the process of bone healing. (14,15) Nitric oxide and vasodilation are imperative for angiogenesis. Positive effects of nitric oxide on wound healing are probably due to its functional effects on angiogenesis and inflammation. (16-18)
Sildenafil is a selective phosphodiesterase-5 inhibitor and a potent stimulator of angiogenesis, which prevents the degradation of nitric oxide. Phosphodiesterase-5 results in the degradation of cyclic guanosine monophosphate, which relaxes the smooth muscles. (19) Sildenafil is a vasodilator of the peripheral arteries and veins and prevents the formation of thrombosis. (20,21) Also, it is the most commonly prescribed medication for males with erectile dysfunction. (22)
Pentoxifylline is a non-selective phosphodiesterase inhibitor that decreases inflammation and increases the blood flow and oxygenation of tissues. (23,24) Also, pentoxifylline decreases platelet accumulation and formation of thrombosis. (25) Compared to other medications in this class, pentoxifylline has fewer gastrointestinal side effects at a lower cost. (26,27)
Recent studies have shown that sildenafil affects growth factors such as vascular endothelial growth factor (VEGF) and cysteine rich-61, thereby enhancing bone healing. (14,28,29) Histing et al reported that sildenafil enhances bone healing by increasing bone formation. (19) Kinoshita et al showed that daily injections of pentoxifylline stimulate bone formation and increase bone mass in rats. (30) Labib et al indicated that pentoxifylline administration can be considered as a reliable approach to manage osseointegration. (31) Moreover, several studies have confirmed the positive effect of pentoxifylline for healing of osteoradionecrosis of the mandible. (32,33) Furthermore, pentoxifylline is extensively used in orthopedics to maintain the viability of the grafts and other vascular tissues used for regenerative treatments. (34)
Many studies have assessed the effects of sildenafil and pentoxifylline on wound healing; however, their efficacy for bone healing has not been well investigated. Moreover, no previous study has evaluated the efficacy of sildenafil and pentoxifylline to enhance the healing of maxillofacial fractures. Considering the gap of information in this regard, this study aimed to assess the effect of sildenafil and pentoxifylline on healing of mandibular fractures in rats.
Materials and Methods
The ethics committee of Isfahan Islamic Azad University (IR.IAU.KHUISF.REC.1398.188) has approved the study protocol. All rats received standard laboratory nutrition and were kept in a calm environment with controlled temperature and moisture (22±2°C and 40-60% humidity) and 12:12 h light/dark cycle as instructed by Welfare. (35) Forty-eight male 12-14-week-old Albino Wistar rats weighing 300-360 gr were evaluated. They did not have any infection or pathological condition affecting the experiment. The rats were randomly divided into six groups of 8 samples each.
Surgical phase:
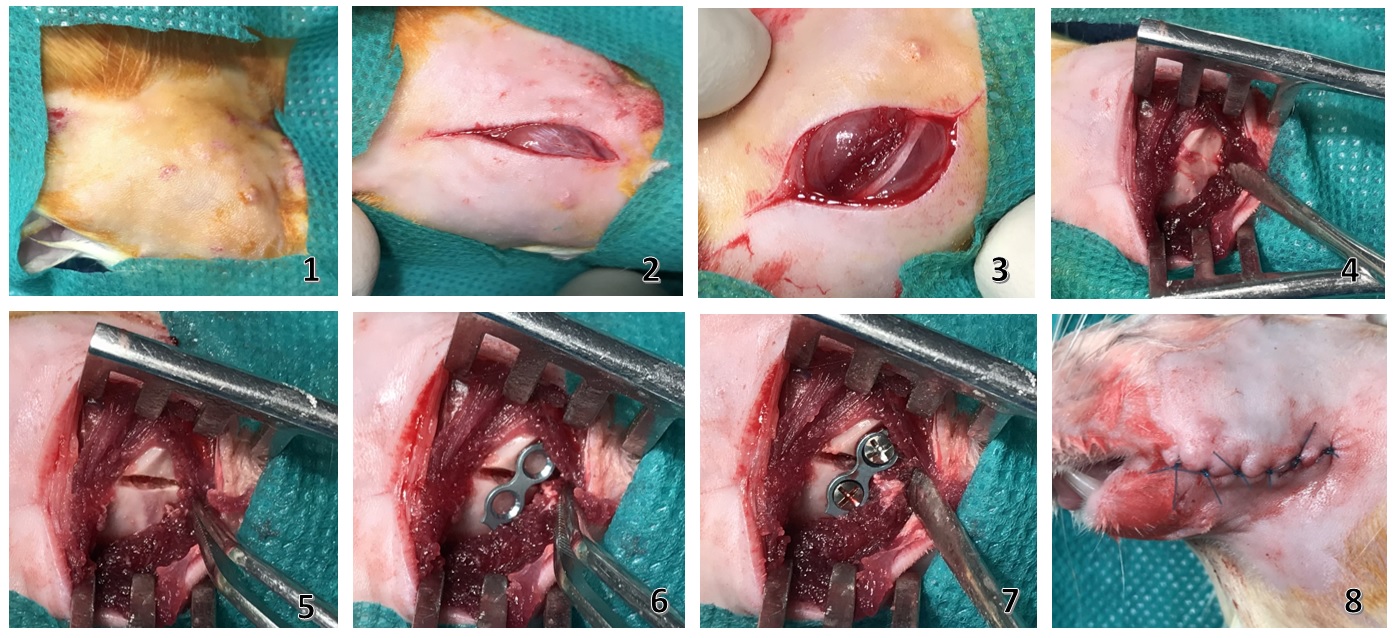
All rats were generally anesthetized by intramuscular injection of 5 mg/kg of ketamine (Ketamine 10%, Alfasan Co., Woerden, Netherlands) and 0.02 ml/kg of acepromazine maleate (Neurotranq, Alfasan Co., Woerden, Netherlands). Next, 0.3 ml of 2% lidocaine with 1:80,000 epinephrine (Persocaine-E; Daroupakhsh, Tehran, Iran) was injected at the surgical site for local anesthesia and hemostasis. The surgical site was shaved and disinfected (Povidone-iodine, Behvazan Co., Rasht, Iran). The rats were placed in a supine position and a 1-cm unilateral submandibular incision was made at the inferior border of the mandible under sterile conditions. After dissecting the masseter muscle, the body of the mandible was exposed. Bicortical osteotomy at the angle of the mandible was performed using a 0.5-mm dental fissure bur (Teezkavan Co., Tehran, Iran) under copious irrigation with sterile saline. The distance between the bone segments was 0.5 mm, which was equal to the bur diameter. The fracture line was fixed using a two-hole microplate (Matrix NEURO adaption plate, thickness: 0.4 mm, pure titanium, Synthes, Switzerland) and two screws with a 1.5-mm diameter (Matrix NEURO screw, self-drilling, 1.5 mm diameter, 3 mm length, Synthes, Switzerland). Subcutaneous and cutaneous tissues were sutured using 5-0 Vicryl sutures (Polyglycolate coated, Supa Co., Tehran, Iran) and 6-0 nylon sutures (Monofilament polyamide, Supa Co., Tehran, Iran). The same surgeon performed all surgical procedures. All rats received 1 mg/kg tramadol (Tramadic, 50mg/ml, Caspian Tamin Co., Rasht, Iran) intramuscularly for pain control and 25 mg/kg cefazolin (Ancef; Kefzol, 1gr, Razi, Iran) intramuscularly for infection control twice a day for 5 days. All rats received a soft diet for one week. Figure 1 shows the surgical steps. The rats were sacrificed by the administration of 200 mg/kg sodium pentobarbital (Pental Sodium®, IE Ulagay, Istanbul, Turkey) after two weeks in groups C2, S2, and P2 and after 6 weeks in groups C6, S6, and P6. The respective hemi-mandible was then resected, and the attached soft tissue was removed. The resected hemi-mandibles were sent for histological analysis. (6)
Figure 1. Surgical steps: (I) shaved surgical site, (II) submandibular cutaneous incision, (III) exposure of the masseter muscle, (IV) dissection of the masseter muscle and exposure of the body of the mandible, (V) fracture line, (VI) placement of a microplate, (VII) fixation with screw, (VIII) suturing
Histological analysis:
A pathologist who was blinded to the group allocation of samples carried out the histological analysis. All specimens were fixed in 10% formalin. After fixing, the specimens were decalcified using ethylene diamine tetra-acetic acid (EDTA). The specimens were then embedded in paraffin blocks and sagittally sectioned into 4µ thick slices. They were then stained with hematoxylin and eosin (H&E). The slides were inspected under a light microscope (Nikon Eclipse E600, Tokyo, Japan). Each specimen was then scored based on the degree of bone healing according to the scoring system suggested by Perry et al, as follows: (11)
Background and Aim: Despite the advances in maxillofacial surgery, impaired bone healing remains a concern for surgical teams. Effects of sildenafil and pentoxifylline on healing of bone fractures have not been well investigated. This study aimed to assess the effects of sildenafil and pentoxifylline phosphodiesterase inhibitors on healing of mandibular fractures in rats.
Materials and Methods: In this animal study, 48 Wistar rats were randomly divided into six groups (n=8). Mandibular fracture was induced in all rats. After the surgical procedure, C2 group (control, 2 weeks) received saline, S2 group (sildenafil, 2 weeks) received 10 mg/kg sildenafil, and P2 group (pentoxifylline, 2 weeks) received 50 mg/kg pentoxifylline. The rats were sacrificed after 2 weeks. C6 (control, 6 weeks), S6 (sildenafil, 6 weeks), and P6 (pentoxifylline, 6 weeks) groups received pharmaceutical therapy as in C2, S2, and P2 but were sacrificed after 6 weeks. The samples then underwent histological analysis. Data were analyzed using SPSS 22 via one-way analysis of variance (ANOVA) and Tukey’s post-hoc test.
Results: The mean rate of healing of mandibular fractures in S2 and P2 was significantly higher than that in C2 after 2 weeks (P<0.001). The mean rate of healing of fractures in P2 was higher than that in S2 after 2 weeks (P=0.04). The mean rate of healing of fractures in S6 (P=0.001) and P6 (P=0.004) was significantly higher than that in C6 after 6 weeks but no significant difference was noted between P6 and S6 in this respect (P=0.53).
Conclusion: Sildenafil and pentoxifylline can be used as adjuncts to enhance bone healing.
Keywords: Bone Healing, Mandibular Fracture, Pentoxifylline, Sildenafil
Introduction
Successful management of maxillofacial fractures depends on correct reduction and precise fixation of broken segments to achieve a normal occlusion, resume function, and properly align the broken pieces next to each other. (1) Despite the advances in maxillofacial surgery, impaired bone healing remains a concern for surgical teams. (2) Mandibular fractures are among the most common fractures of the maxillofacial region accounting for 23% to 97% of all facial fractures. (3,4)
Bone healing is a complex process that includes three stages of inflammation, repair, and delayed remodeling. This biological process is controlled by complex cellular and molecular mechanisms. Systemic and local factors and several cell types and growth factors delivered via the adjacent tissues and bloodstream play a role in bone healing. (5-7) Several studies have evaluated growth factors, injection of medications, and electrical stimulation to accelerate and enhance bone healing. (8-10) In contrast, several studies have indicated that some medications, such as antibiotics and bisphosphonates, delay or impair the process of bone healing. By having comprehensive knowledge about these factors and not prescribing them in case of fracture, complete bone healing can be expected. (11,12) Bleeding at the site of injury is the most important factor for successful bone healing. (13) Decreased angiogenesis at the site of trauma and limited blood supply to the site are known as factors delaying or impairing the process of bone healing. (14,15) Nitric oxide and vasodilation are imperative for angiogenesis. Positive effects of nitric oxide on wound healing are probably due to its functional effects on angiogenesis and inflammation. (16-18)
Sildenafil is a selective phosphodiesterase-5 inhibitor and a potent stimulator of angiogenesis, which prevents the degradation of nitric oxide. Phosphodiesterase-5 results in the degradation of cyclic guanosine monophosphate, which relaxes the smooth muscles. (19) Sildenafil is a vasodilator of the peripheral arteries and veins and prevents the formation of thrombosis. (20,21) Also, it is the most commonly prescribed medication for males with erectile dysfunction. (22)
Pentoxifylline is a non-selective phosphodiesterase inhibitor that decreases inflammation and increases the blood flow and oxygenation of tissues. (23,24) Also, pentoxifylline decreases platelet accumulation and formation of thrombosis. (25) Compared to other medications in this class, pentoxifylline has fewer gastrointestinal side effects at a lower cost. (26,27)
Recent studies have shown that sildenafil affects growth factors such as vascular endothelial growth factor (VEGF) and cysteine rich-61, thereby enhancing bone healing. (14,28,29) Histing et al reported that sildenafil enhances bone healing by increasing bone formation. (19) Kinoshita et al showed that daily injections of pentoxifylline stimulate bone formation and increase bone mass in rats. (30) Labib et al indicated that pentoxifylline administration can be considered as a reliable approach to manage osseointegration. (31) Moreover, several studies have confirmed the positive effect of pentoxifylline for healing of osteoradionecrosis of the mandible. (32,33) Furthermore, pentoxifylline is extensively used in orthopedics to maintain the viability of the grafts and other vascular tissues used for regenerative treatments. (34)
Many studies have assessed the effects of sildenafil and pentoxifylline on wound healing; however, their efficacy for bone healing has not been well investigated. Moreover, no previous study has evaluated the efficacy of sildenafil and pentoxifylline to enhance the healing of maxillofacial fractures. Considering the gap of information in this regard, this study aimed to assess the effect of sildenafil and pentoxifylline on healing of mandibular fractures in rats.
Materials and Methods
The ethics committee of Isfahan Islamic Azad University (IR.IAU.KHUISF.REC.1398.188) has approved the study protocol. All rats received standard laboratory nutrition and were kept in a calm environment with controlled temperature and moisture (22±2°C and 40-60% humidity) and 12:12 h light/dark cycle as instructed by Welfare. (35) Forty-eight male 12-14-week-old Albino Wistar rats weighing 300-360 gr were evaluated. They did not have any infection or pathological condition affecting the experiment. The rats were randomly divided into six groups of 8 samples each.
Surgical phase:
All rats were generally anesthetized by intramuscular injection of 5 mg/kg of ketamine (Ketamine 10%, Alfasan Co., Woerden, Netherlands) and 0.02 ml/kg of acepromazine maleate (Neurotranq, Alfasan Co., Woerden, Netherlands). Next, 0.3 ml of 2% lidocaine with 1:80,000 epinephrine (Persocaine-E; Daroupakhsh, Tehran, Iran) was injected at the surgical site for local anesthesia and hemostasis. The surgical site was shaved and disinfected (Povidone-iodine, Behvazan Co., Rasht, Iran). The rats were placed in a supine position and a 1-cm unilateral submandibular incision was made at the inferior border of the mandible under sterile conditions. After dissecting the masseter muscle, the body of the mandible was exposed. Bicortical osteotomy at the angle of the mandible was performed using a 0.5-mm dental fissure bur (Teezkavan Co., Tehran, Iran) under copious irrigation with sterile saline. The distance between the bone segments was 0.5 mm, which was equal to the bur diameter. The fracture line was fixed using a two-hole microplate (Matrix NEURO adaption plate, thickness: 0.4 mm, pure titanium, Synthes, Switzerland) and two screws with a 1.5-mm diameter (Matrix NEURO screw, self-drilling, 1.5 mm diameter, 3 mm length, Synthes, Switzerland). Subcutaneous and cutaneous tissues were sutured using 5-0 Vicryl sutures (Polyglycolate coated, Supa Co., Tehran, Iran) and 6-0 nylon sutures (Monofilament polyamide, Supa Co., Tehran, Iran). The same surgeon performed all surgical procedures. All rats received 1 mg/kg tramadol (Tramadic, 50mg/ml, Caspian Tamin Co., Rasht, Iran) intramuscularly for pain control and 25 mg/kg cefazolin (Ancef; Kefzol, 1gr, Razi, Iran) intramuscularly for infection control twice a day for 5 days. All rats received a soft diet for one week. Figure 1 shows the surgical steps. The rats were sacrificed by the administration of 200 mg/kg sodium pentobarbital (Pental Sodium®, IE Ulagay, Istanbul, Turkey) after two weeks in groups C2, S2, and P2 and after 6 weeks in groups C6, S6, and P6. The respective hemi-mandible was then resected, and the attached soft tissue was removed. The resected hemi-mandibles were sent for histological analysis. (6)
Figure 1. Surgical steps: (I) shaved surgical site, (II) submandibular cutaneous incision, (III) exposure of the masseter muscle, (IV) dissection of the masseter muscle and exposure of the body of the mandible, (V) fracture line, (VI) placement of a microplate, (VII) fixation with screw, (VIII) suturing
{kind=link}
Histological analysis:
A pathologist who was blinded to the group allocation of samples carried out the histological analysis. All specimens were fixed in 10% formalin. After fixing, the specimens were decalcified using ethylene diamine tetra-acetic acid (EDTA). The specimens were then embedded in paraffin blocks and sagittally sectioned into 4µ thick slices. They were then stained with hematoxylin and eosin (H&E). The slides were inspected under a light microscope (Nikon Eclipse E600, Tokyo, Japan). Each specimen was then scored based on the degree of bone healing according to the scoring system suggested by Perry et al, as follows: (11)
- 1 point, only fibrous tissue
- 2 points, mainly fibrous tissue and a small amount of cartilage tissue
- 3 points, an equal amount of fibrous and cartilage tissue
- 4 points, completely cartilage tissue
- 5 points, mainly cartilage tissue and a small amount of immature (woven) bone
- 6 points, an equal amount of cartilage tissue and immature bone
- 7 points, significantly immature (woven) bone and a small amount of cartilage
- 8 points, completely immature (woven) bone
- 9 points, immature bone and a small amount of mature bone
- 10 points, mature (lamellar) bone. (11)
Rats in the C2 group received saline orally on a daily basis after the surgery and were sacrificed after two weeks.
Rats in the S2 group received 10 mg/kg sildenafil (Sildenafil 50 mg, Marham Daru Co., Tehran, Iran) orally via gavage daily and were sacrificed after two weeks.
Rats in the P2 group received 50 mg/kg pentoxifylline (Pentoxifylline 400 mg; Extended Release, Amin Pharmaceutical Co., Isfahan, Iran) orally via gavage daily and were sacrificed after two weeks.
The C6 (control, 6 weeks), S6 (sildenafil, 6 weeks) and P6 (pentoxifylline, 6 weeks) groups received medications as in groups C2, S2, and P2 but were sacrificed after six weeks.
The dosage of administered medications was determined according to similar previous studies. (34,36-38) Use of higher doses may cause greater vasodilation but may be associated with side effects such as hypotension, decreased tissue perfusion, and severe anti-inflammatory responses. Use of lower doses may have no effect at all. (39)
Statistical analysis:
Data were analyzed using SPSS version 22 (SPSS Inc., Chicago, IL, USA) via one-way analysis of variance (ANOVA) and Tukey’s post-hoc test to find significant differences between groups. The mean and standard deviation (SD) of the findings of the histological analysis were reported.
Results
This study evaluated the effects of two phosphodiesterase inhibitors on bone healing in mandibular fractures in rats. Forty-eight rats were evaluated in six groups of eight. None of the rats expired during the study and no complication occurred. All rats well tolerated the surgical procedure. The mean rate of bone healing was 2.8±0.7, 4.8±0.9, and 5.5±0.9 in C2, S2, and P2 groups, respectively (Table 1).
Table 1: Mean and standard deviation (SD) of bone healing in mandibular fractures in the studied groups
{kind=link}
One-way ANOVA showed that the mean rate of bone healing in mandibular fractures was significantly different among the aforementioned three groups after two weeks (P=0.0005). Tukey’s post-hoc test revealed that the mean rate of bone healing in S2 and P2 groups was significantly higher than that in the C2 group after two weeks (P=0.0005). The mean rate of bone healing in the P2 group was significantly higher than that in the S2 group after two weeks (P=0.04).
The mean rate of bone healing was 7.7±1.06, 9.5±1.08 and 9.2±1.03 in groups C6, S6, and P6, respectively (Table 1). One-way ANOVA revealed that the mean rate of bone healing was significantly different among the aforementioned three groups after 6 weeks (P=0.002). Tukey’s test revealed that the mean rate of bone healing in S6 (P=0.001) and P6 (P=0.004) groups was significantly higher than that in the C6 group after 6 weeks but no significant difference was noted between P6 and S6 groups in this respect (P=0.53).
Figure 2 shows histological images of study groups at x100 magnification.
Figure 2. Histological images of study groups at x100 magnification. (A) A specimen from the C2 group with bone healing score 3 (equal amount of fibrous and cartilage tissue). (B) A specimen from the S2 group with bone healing score 5 [mainly cartilage tissue and a small amount of immature (woven) bone]. (C) A specimen from the P2 group with bone healing score 7 [significantly immature (woven) bone and a small amount of cartilage]. (D) A specimen from the C6 group with bone healing score 8 [completely immature (woven) bone]. (E) A specimen from the S6 group with bone healing score 9 (healing with immature bone and a small amount of mature bone). (F) A specimen from the P6 group with bone healing score 10 [mature (lamellar) bone]
![Figure 2. Histological images of study groups at x100 magnification. (A) A specimen from the C2 group with bone healing score 3 (equal amount of fibrous and cartilage tissue). (B) A specimen from the S2 group with bone healing score 5 [mainly cartilage tissue and a small amount of immature (woven) bone]. (C) A specimen from the P2 group with bone healing score 7 [significantly immature (woven) bone and a small amount of cartilage]. (D) A specimen from the C6 group with bone healing score 8 [completely immature (woven) bone]. (E) A specimen from the S6 group with bone healing score 9 (healing with immature bone and a small amount of mature bone). (F) A specimen from the P6 group with bone healing score 10 [mature (lamellar) bone]](./files/site1/images/20193/article_A-10-598-2--atch-66.jpg){kind=link}
As shown in Figure 3, bone tissue can be divided into lamellar and woven bone according to its level of maturity. An eosinophilic area containing lacunae was noted in lamellar bone tissue under the microscope (marked by *), and lines confirming periodic calcification of bone could be seen. These parts were the old host bone, which were mature and seen on the two sides of the fracture line. The shorter the time duration since fracture, the less mature the tissue around the mature bone margins would be. The size and number of lacunae are also important. In areas marked with * (old bone), the number of lacunae and their size were smaller. The area marked with a circle indicates the newly forming, immature bone. This bone has a cancellous appearance and has differences with mature bone in terms of the number of lacunae (where the osteocytes are present) and their size. The area marked with a square indicates the interface of the newly formed bone and older bone. The area marked with an arrow shows the cartilage tissue. The area marked with x indicates cartilage calcification and its conversion to bone.
Figure 3. Histological image of the P2 group with bone healing score 5 (x100 magnification)
{kind=link}
Discussion
This study assessed the effects of sildenafil and pentoxifylline on bone healing in mandibular fractures in rats. Healing of fractures is an important topic in maxillofacial surgery. The routine function of patients should be reinstated as soon as possible. (40) Many studies have evaluated this topic, (40,41) and evidence shows that the outcome of surgical procedures for treatment of fractures is influenced by several factors such as patient-related factors, type of bone defect, and type of surgical procedure. (40) Adequate blood supply plays a critical role in bone healing. (42,43) Impaired angiogenesis at the site leads to poor healing of bone. Oxygen and nutrients are delivered to the site of bone callus formation through the bloodstream. Moreover, the bloodstream delivers progenitor and inflammatory cells to the site of injury. (20,21,28) Nitric oxide and vasodilation are also imperative for angiogenesis. (44) Positive effects of nitric oxide on wound healing may be related to its functional effects on angiogenesis and inflammation. Sildenafil prevents the breakdown and degradation of nitric oxide, which leads to vasodilation and increased blood supply to the tissue. (16-18) Several studies have shown that sildenafil is effective for different pathological conditions via the nitric oxide pathway. In addition, many studies have focused on the effects of sildenafil on tissue healing. Many clinical and animal studies have shown the positive effects of sildenafil in cases of decreased blood supply to the skin and impaired vascularization as in ischemic wounds. (18,21,29) Moreover, evidence shows that enhanced bone healing by sildenafil can be due to the function of cysteine-rich angiogenic inducer 61 protein, which stimulates endothelial cell migration and induces proliferation and differentiation of osteoblasts and cell adhesion. (14,45) Pentoxifylline is a phosphodiesterase inhibitor derived from xanthine, which has a vasodilatory effect. In contrast to most peripheral vasodilators, pentoxifylline has rheological effects on blood and decreases its viscosity. (24) The therapeutic effects of pentoxifylline are mainly attributed to its potential for increasing the blood flow and oxygenation of tissues due to its hemorheological property. (25) It is not clear whether pentoxifylline increases the number of osteoblasts and osteoclasts or not. Takami et al showed that phosphodiesterase inhibitors increase the number of osteoclasts and their differentiation to osteoblasts. (46) Horiuchi et al demonstrated that pentoxifylline enhances new bone formation by upregulating the bone morphogenetic protein-2. (47,48) Tsutsumimoto et al indicated that pentoxifylline can be used to enhance bone formation. (49)
Many studies have evaluated several medications and factors to enhance bone healing and demonstrated that bone morphogenetic proteins, insulin-like growth factor 1 (IGF1), transforming growth factor B1 (TGFB1), and vitamin E can all enhance the process of bone healing. (50-53) Several studies have evaluated the effects of phosphodiesterase inhibitors on bone healing with results comparable to ours. However, no previous study evaluated the effects of sildenafil and pentoxifylline on maxillofacial fractures. (42,54,55) The current results revealed that pentoxifylline and sildenafil have positive effects on bone healing. Our findings regarding enhanced bone healing by sildenafil were in agreement with those of Yaman et al, Histing et al, and Çakir-Özkan et al. (42,19,56) Aydin et al used pentoxifylline in a dosage similar to ours and showed that pentoxifylline enhances the formation of a hematoma, which is the first phase of bone healing. (34) This result was in agreement with our findings. However, they showed that the anti-inflammatory effects of pentoxifylline might delay bone healing after 3 weeks. (34) This result was in contrast to ours. Our study showed positive effects of pentoxifylline on bone healing in the late stage. Since they evaluated femoral bone fractures, this difference in the results may be related to different rates and modes of metabolism of femoral bone and mandibular bone at the final stages of fracture healing.
Our results regarding enhanced bone healing by sildenafil were in line with those of Histing et al, (19) with the difference that they used 5 mg/kg dose of sildenafil while we used 10 mg/kg dosage according to the previously published studies. The reason behind the use of 5 mg/kg dosage of sildenafil in their study was that the speed of metabolism of sildenafil is higher in rats and sildenafil has a half-life of one hour in rats and four hours in humans. They used 5 mg/kg dosage for rats, which is 5 times the standard dosage for humans (0.7 to 1.5 mg/kg). Despite the different dosages used in the two studies, the outcomes were the same. Atalay et al used the same dosage of pentoxifylline as ours. (40) The mean histological score of bone healing in their study was 7.8 after 6 weeks while it was 9.2 in our study. This difference was probably due to the difference in defect size in the two studies. The bone gap created in their study after osteotomy was 1 mm while it was 0.5 mm in our study. In the present study, bone healing in the pentoxifylline group was significantly higher than that in the sildenafil group after two weeks but the score of bone healing in the sildenafil group was higher than that in the pentoxifylline group after six weeks. It seems that the rheological effects of pentoxifylline and reduction of blood viscosity by this medication in the first two weeks enhanced the primary phase of healing and formation of a hematoma at the site of fracture. However, the authors believe that at the end of the sixth week, the anti-inflammatory effects of pentoxifylline, similar to those of other non-steroidal anti-inflammatory drugs (NSAIDs), delay the process of bone healing. For this reason, at the end of the sixth week, the bone-healing rate in the sildenafil group was higher than that in the pentoxifylline group.
Infection also plays a role in bone healing. Aydin et al (34) showed lower bone healing rate (7.1 versus 9.2) at similar time points and with the use of the same dosage of pentoxifylline, which may be due to no use of antibiotics postoperatively in their study. As they reported, 40% of the samples in the pentoxifylline group had an infection, which seemed to slow down the process of bone healing. (34) Gong et al indicated that the use of tadalafil and vardenafil phosphodiesterase inhibitors decreased the bone mass. (57) Their study was the only one that reported results contrary to ours. This difference may be attributed to different study designs and different types of selective phosphodiesterase inhibitors used.
Despite the abovementioned studies, our knowledge about the effects of phosphodiesterase inhibitors on bone metabolism and healing is insufficient. A good understanding of the biological events that occur in the process of bone healing is imperative to find the most efficient approach to enhance bone healing. This study was the first to show the positive effects of sildenafil and pentoxifylline on healing of mandibular bone fractures. Thus, sildenafil and pentoxifylline can be used as adjuncts to enhance bone healing.
One limitation of this study was the daily use of 50 mg/kg dosage of pentoxifylline and 10 mg/kg dosage of sildenafil; thus, bone healing in response to higher and lower doses remains a matter of question. Also, due to ethical considerations, we could not employ a larger sample size. Finally yet importantly, it is not known to what extent the slight histological differences are clinically important. Clinical studies using different doses of sildenafil and pentoxifylline are required to assess bone healing at different time points. Also, similar studies are recommended on rabbits or dogs since they have higher histological and anatomical similarities with humans, and the surgical procedure of their mandible would be easier to perform. Moreover, radiographic and biomechanical assessments should be carried out in addition to histological analysis, and expression of genes involved in bone healing should be evaluated. Finally yet importantly, similar studies are required on osteoporotic mandibles, those under bisphosphonate therapy, chemotherapy, and radiotherapy to assess the efficacy of these medications to enhance bone healing in pathological conditions.
Conclusion
The results of this study showed that sildenafil and pentoxifylline can be used as adjuncts to enhance bone healing in mandibular fractures.
Type of Study: Original article |
Subject:
Oral & maxillofacial surgery
References
1. 1. Glória JCR, Fernandes IA, da Silveira EM, de Souza GM, Rocha RL, Galvao EL et al. Comparison of Bite Force with Locking Plates versus Non-Locking Plates in the Treatment of Mandibular Fractures: A Meta-Analysis. Int Arch Otorhinolaryngol. 2018 Apr;22(2):181-9. [DOI:10.1055/s-0037-1604056] [PMID] [PMCID]
2. Uçan MC, Koparal M, Ağaçayak S, Gunay A, Ozgoz M, Atilgan S, et al. Influence of caffeic acid phenethyl ester on bone healing in a rat model. J Int Med Res. 2013 Oct;41(5):1648-54. [DOI:10.1177/0300060513490613] [PMID]
3. Fernández JR, Gallas M, Burguera M, Viaño JM. A three-dimensional numerical simulation of mandible fracture reduction with screwed miniplates. J Biomech. 2003 Mar;36(3):329-37. [DOI:10.1016/S0021-9290(02)00416-5]
4. Durmuş K, Turgut NH, Doğan M, Tuncer E, Özer H, Altuntaş EE, et al. Histopathological evaluation of the effect of locally administered strontium on healing time in mandibular fractures: An experimental study. Adv Clin Exp Med. 2017 Oct;26(7):1063-7. [DOI:10.17219/acem/65477] [PMID]
5. Hausman MR, Schaffler MB, Majeska RJ. Prevention of fracture healing in rats by an inhibitor of angiogenesis. Bone. 2001 Dec;29(6):560-4. [DOI:10.1016/S8756-3282(01)00608-1]
6. Dincel YM, Alagoz E, Arikan Y, Caglar AK, Dogru SC, Ortes F, et al. Biomechanical, histological, and radiological effects of different phosphodiesterase inhibitors on femoral fracture healing in rats. J Orthop Surg (Hong Kong). 2018 May-Aug;26(2):2309499018777885. [DOI:10.1177/2309499018777885] [PMID]
7. Hankenson KD, Zimmerman G, Marcucio R. Biological perspectives of delayed fracture healing. Injury. 2014 Jun;45 Suppl 2:S8-S15. [DOI:10.1016/j.injury.2014.04.003] [PMID] [PMCID]
8. Cook JJ, Summers NJ, Cook EA. Healing in the new millennium: bone stimulators: an overview of where we've been and where we may be heading. Clin Podiatr Med Surg. 2015 Jan;32(1):45-59. [DOI:10.1016/j.cpm.2014.09.003] [PMID]
9. Chao EY, Inoue N. Biophysical stimulation of bone fracture repair, regeneration and remodelling. Eur Cell Mater. 2003 Dec;6:72-84. [DOI:10.22203/eCM.v006a07] [PMID]
10. Massari L, Caruso G, Sollazzo V, Setti S. Pulsed electromagnetic fields and low intensity pulsed ultrasound in bone tissue. Clin Cases Miner Bone Metab. 2009 May;6(2):149-54.
11. Perry AC, Prpa B, Rouse MS, Piper KE, Hanssen AD, Steckelberg JM, et al. Levofloxacin and trovafloxacin inhibition of experimental fracture-healing. Clin Orthop Relat Res. 2003 Sep;(414):95-100. [DOI:10.1097/01.blo.0000087322.60612.14] [PMID]
12. Zandi M, Dehghan A, Amini P, Rezaeian L, Doulati S. Evaluation of mandibular fracture healing in rats under zoledronate therapy: A histologic study. Injury. 2017 Dec;48(12):2683-2687. [DOI:10.1016/j.injury.2017.10.026] [PMID]
13. Colnot C, Lu C, Hu D, Helms JA. Distinguishing the contributions of the perichondrium, cartilage, and vascular endothelium to skeletal development. Dev Biol. 2004 May 1;269(1):55-69. [DOI:10.1016/j.ydbio.2004.01.011] [PMID]
14. Lienau J, Schell H, Epari DR, Schütze N, Jakob F, Duda GN, et al. CYR61 (CCN1) protein expression during fracture healing in an ovine tibial model and its relation to the mechanical fixation stability. J Orthop Res. 2006 Feb;24(2):254-62. [DOI:10.1002/jor.20035] [PMID]
15. Keramaris NC, Calori GM, Nikolaou VS, Schemitsch EH, Giannoudis PV. Fracture vascularity and bone healing: a systematic review of the role of VEGF. Injury. 2008 Sep;39 Suppl 2:S45-57. [DOI:10.1016/S0020-1383(08)70015-9]
16. Diwan AD, Wang MX, Jang D, Zhu W, Murrell GA. Nitric oxide modulates fracture healing. J Bone Miner Res. 2000 Feb;15(2):342-51. [DOI:10.1359/jbmr.2000.15.2.342] [PMID]
17. Baldik Y, Talu U, Altinel L, Bilge H, Demiryont M, Aykac-Toker G. Bone healing regulated by nitricoxide: an experimental study in rats. Clin Orthop Relat Res. 2002 Nov;(404):343-52. [DOI:10.1097/00003086-200211000-00051] [PMID]
18. Derici H, Kamer E, Unalp HR, Diniz G, Bozdag AD, Tansug T, et al. Effect of sildenafil on wound healing: an experimental study. Langenbecks Arch Surg. 2010 Aug;395(6):713-8. [DOI:10.1007/s00423-009-0471-2] [PMID]
19. Histing T, Marciniak K, Scheuer C, Garcia P, Holstein JH, Klein M, et al. Sildenafil accelerates fracture healing in mice. J Orthop Res. 2011 Jun;29(6):867-73. [DOI:10.1002/jor.21324] [PMID]
20. Vidavalur R, Penumathsa SV, Zhan L, Thirunavukkarasu M, Maulik N. Sildenafil induces angiogenic response in human coronary arteriolar endothelial cells through the expression of thioredoxin, hemeoxygenase and vascular endothelial growth factor. Vascul Pharmacol. 2006 Aug;45(2):91-5. [DOI:10.1016/j.vph.2006.03.010] [PMID]
21. Hart K, Baur D, Hodam J, Lesoon-Wood L, Parham M, Keith K, et al. Short- and long-term effects of sildenafil on skin flap survival in rats. Laryngoscope. 2006 Apr;116(4):522-8. [DOI:10.1097/01.mlg.0000200792.67802.3b] [PMID]
22. Das A, Xi L, Kukreja RC. Phosphodiesterase-5 inhibitor sildenafil preconditions adult cardiac myocytes against necrosis and apoptosis. Essential role of nitric oxide signaling. J Biol Chem. 2005 Apr 1;280(13):12944-55. [DOI:10.1074/jbc.M404706200] [PMID]
23. Essayan DM. Cyclic nucleotide phosphodiesterases. J Allergy Clin Immunol. 2001;108:671-680. [DOI:10.1067/mai.2001.119555] [PMID]
24. Delanian S, Porcher R, Rudant J, Lefaix JL. Kinetics of response to long-term treatment combining pentoxifylline and tocopherol in patients with superficial radiation-induced fibrosis. J Clin Oncol. 2005 Dec 1;23(34):8570-9 [DOI:10.1200/JCO.2005.02.4729] [PMID]
25. Ward A, Clissold SP. Pentoxifylline. A review of its pharmacodynamic and pharmacokinetic properties, and its therapeutic efficacy. Drugs. 1987 Jul;34(1):50-97. [DOI:10.2165/00003495-198734010-00003] [PMID]
26. Bayat M, Amini A, Rezaie F, Bayat S. Patents of Pentoxifylline Administration on Some Diseases and Chronic Wounds. Recent Pat Regen Med. 2014;4(2):137-43. [DOI:10.2174/2210296504666140813194744]
27. Vashghani Farahani MM, Masteri Farahani R, Mostafavinia A, Abbasian MR, Pouriran R, Noruzian M, et al. Effect of Pentoxifylline Administration on an Experimental Rat Model of Femur Fracture Healing With Intramedullary Fixation. Iran Red Crescent Med J. 2015 Dec 28;17(12):e29513. [DOI:10.5812/ircmj.29513] [PMID] [PMCID]
28. Ghofrani HA, Osterloh IH, Grimminger F. Sildenafil. from angina to erectile dysfunction to pulmonary hypertension and beyond. Nat Rev Drug Discov 2006 Aug;5(8):689-702. [DOI:10.1038/nrd2030] [PMID]
29. Koneru S, Varma Penumathsa S, Thirunavukkarasu M, Vidavalur R, Zhan L, Singal PK, et al. Sildenafil mediated neovascularization and protection against myocardial ischaemia reperfusion injury in rats: role of VEGF/angiopoietin-1. J Cell Mol Med. 2008 Dec;12(6B):2651-64. [DOI:10.1111/j.1582-4934.2008.00319.x] [PMID] [PMCID]
30. Kinoshita T, Kobayashi S, Ebara S, Yoshimura Y, Horiuchi H, Tsutsumimoto T, et al. Phosphodiesterase inhibitors, pentoxifylline and rolipram, increase bone mass mainly by promoting bone formation in normal mice. Bone. 2000 Dec;27(6):811-7. [DOI:10.1016/S8756-3282(00)00395-1]
31. Labib GS, Farid RM. Osteogenic effect of locally applied Pentoxyfilline gel: in vitro and in vivo evaluations. Drug Deliv. 2015 Dec;22(8):1094-1102. [DOI:10.3109/10717544.2014.884193] [PMID]
32. Kahenasa N, Sung EC, Nabili V, Kelly J, Garrett N, Nishimura I. Resolution of pain and complete healing of mandibular osteoradionecrosis using pentoxifylline and tocopherol: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 Apr;113(4):e18-23. [DOI:10.1016/j.oooo.2011.10.014] [PMID]
33. Delanian S, Depondt J, Lefaix JL. Major healing of refractory mandible osteoradionecrosis after treatment combining pentoxifylline and tocopherol: a phase II trial. Head Neck. 2005 Feb;27(2):114-23. [DOI:10.1002/hed.20121] [PMID]
34. Aydin K, Sahin V, Gürsu S, Mercan AS, Demir B, Yildirim T. Effect of pentoxifylline on fracture healing: an experimental study. Eklem Hastalik Cerrahisi. 2011 Dec;22(3):160-5.
35. National Research Council (US) Institute for Laboratory Animal Research. Guide for the Care and Use of Laboratory Animals. Washington (DC): National Academies Press (US); 1996.
36. Schlundt C, El Khassawna T, Serra A, Dienelt A, Wendler S, Schell H, et al. Macrophages in bone fracture healing: Their essential role in endochondral ossification. Bone. 2018 Jan;106:78-89. [DOI:10.1016/j.bone.2015.10.019] [PMID]
37. Rotter N, Haisch A, Bücheler M. Cartilage and bone tissue engineering for reconstructive head and neck surgery. Eur Arch Otorhinolaryngol. 2005 Jul;262(7):539-45. [DOI:10.1007/s00405-004-0866-1] [PMID]
38. Vega LG. Reoperative mandibular trauma: management of posttraumatic mandibular deformities. Oral Maxillofac Surg Clin North Am. 2011 Feb;23(1):47-61, v-vi. [DOI:10.1016/j.coms.2010.12.003] [PMID]
39. Irkorucu O, Taşcilar O, Cakmak GK, Karakaya K, Emre AU, Ucan BH, et al. The effect of sildenafil on an animal model for ischemic colitis. Dig Dis Sci. 2008 Jun;53(6):1618-23. [DOI:10.1007/s10620-007-0033-9] [PMID]
40. Atalay Y, Bozkurt MF, Gonul Y, Cakmak O, Agacayak KS, Köse I, et al. The effects of amlodipine and platelet rich plasma on bone healing in rats. Drug Des Devel Ther. 2015 Apr 7;9:1973-81. [DOI:10.2147/DDDT.S80778] [PMID] [PMCID]
41. Anitua E, Sánchez M, Orive G, Andía I. The potential impact of the preparation rich in growth factors (PRGF) in different medical fields. Biomaterials 2007 Nov;28(31):4551-60. [DOI:10.1016/j.biomaterials.2007.06.037] [PMID]
42. Yaman F, Atilgan S, Günes N, Agacayak S, Günay A, Ucan MC, et al. Phosphodiesterase-5 inhibitors may facilitate bone defect recovery. Eur Rev Med Pharmacol Sci. 2011 Nov;15(11):1301-5.
43. Rajkumar DS, Faitelson AV, Gudyrev OS, Dubrovin GM, Pokrovski MV, Ivanov AV. Comparative evaluation of enalapril and losartan in pharmacological correction of experimental osteoporosis and fractures of its background. J Osteoporos. 2013;2013:325693. [DOI:10.1155/2013/325693] [PMID] [PMCID]
44. Corbett SA, Hukkanen M, Batten J, McCarthy ID, Polak JM, Hughes S. Nitric oxide in fracture repair. Differential localisation, expression and activity of nitric oxide synthases. J Bone Joint Surg Br. 1999 May;81(3):531-7. [DOI:10.1302/0301-620X.81B3.0810531]
45. Si W, Kang Q, Luu HH, Park JK, Luo Q, Song WX, et al. CCN1/Cyr61 is regulated by the canonical Wnt signal and plays an important role in Wnt3A-induced osteoblast differentiation of mesenchymal stem cells. Mol Cell Biol. 2006 Apr;26(8):2955-64. [DOI:10.1128/MCB.26.8.2955-2964.2006] [PMID] [PMCID]
46. Takami M, Cho ES, Lee SY, Kamijo R, Yim M. Phosphodiesterase inhibitors stimulate osteoclast formation via TRANCE/RANKL expression in osteoblasts: possible involvement of ERK and p38 MAPK pathways. FEBS Lett. 2005 Jan 31;579(3):832-8. [DOI:10.1016/j.febslet.2004.12.066] [PMID]
47. Horiuchi H, Saito N, Kinoshita T, Wakabayashi S, Tsutsumimoto T, Otsuru S, et al. Enhancement of recombinant human bone morphogenetic protein-2 (rhBMP-2)-induced new bone formation by concurrent treatment with parathyroid hormone and a phosphodiesterase inhibitor, pentoxifylline. J Bone Miner Metab. 2004;22(4):329-34. [DOI:10.1007/s00774-003-0490-y] [PMID]
48. Horiuchi H, Saito N, Kinoshita T, Wakabayashi S, Tsutsumimoto T, Takaoka K. Enhancement of bone morphogenetic protein-2-induced new bone formation in mice by the phosphodiesterase inhibitor pentoxifylline. Bone. 2001 Mar;28(3):290-4 [DOI:10.1016/S8756-3282(00)00450-6]
49. Tsutsumimoto T, Wakabayashi S, Kinoshita T, Horiuchi H, Takaoka K. A phosphodiesterase inhibitor, pentoxifylline, enhances the bone morphogenetic protein-4 (BMP-4)- dependent differentiation of osteoprogenitor cells. Bone. 2002 Sep;31(3):396-401 [DOI:10.1016/S8756-3282(02)00839-6]
50. Westerhuis RJ, van Bezooijen RL, Kloen P. Use of bone morphogenetic proteins in traumatology. Injury. Injury. 2005 Dec;36(12):1405-12 [DOI:10.1016/j.injury.2005.02.047] [PMID]
51. Einhorn TA. Clinical applications of recombinant human BMPs: early experience and future development. J Bone Joint Surg Am. 2003;85 Suppl 3:82-8. [DOI:10.2106/00004623-200300003-00014] [PMID]
52. Schmidmaier G, Wildemann B, Heeger J, Gäbelein T, Flyvbjerg A, Bail HJ, et al. Improvement of fracture healing by systemic administration of growth hormone and local application of insulin-like growth factor-1 and transforming growth factor-beta1. Bone. 2002 Jul;31(1):165-72. [DOI:10.1016/S8756-3282(02)00798-6]
53. Turk C, Halici M, Guney A, Akgun H, Sahin V, Muhtaroglu S. Promotion of fracture healing by vitamin E in rats. J Int Med Res. 2004 Sep-Oct;32(5):507-12. [DOI:10.1177/147323000403200508] [PMID]
54. Rauch F, Lauzier D, Croteau S, Travers R, Glorieux FH, Hamdy R. Temporal and spatial expression of bone morphogenetic protein-2, -4, and -7 during distraction osteogenesis in rabbits. Bone. 2000 Sep;27(3):453-9. [DOI:10.1016/S8756-3282(00)00337-9]
55. Farhadieh RD, Gianoutsos MP, Yu Y, Walsh WR. The role of bone morphogenetic proteins BMP-2 and BMP-4 and their related postreceptor signaling system (Smads) in distraction osteogenesis of the mandible. J Craniofac Surg. 2004 Sep;15(5):714-8. [DOI:10.1097/00001665-200409000-00003] [PMID]
56. Emami Meibodi SH, Narimani MA, Sarkarat F, Omidsalar P. Evaluation of the Correlation between Vertical Facial Discrepancies and Cervical Vertebral Fusion. J Res Dentomaxillofac Sci. 2018;3(4):38-42. [DOI:10.29252/jrdms.3.4.38]
57. Çakir-Özkan N, Bereket C, Sener I, Alici Ö, Kabak YB, Önger ME. Therapeutic Effects of Sildenafil on Experimental Mandibular Fractures. J Craniofac Surg. 2016 May;27(3):615-20. [DOI:10.1097/SCS.0000000000002527] [PMID]
58. Gong Y, Xu CY, Wang JR, Hu XH, Hong D, Ji X, et al. Inhibition of phosphodiesterase 5 reduces bone mass by suppression of canonical Wnt signaling. Cell Death Dis. 2014 Nov 27;5:e1544. [DOI:10.1038/cddis.2014.510] [PMID] [PMCID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
