

Volume 3, Issue 3 (8-2018)
J Res Dent Maxillofac Sci 2018, 3(3): 1-8 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nazarian N, Abbasi M, Sakhdari S, Ghannad S. Comparison of Canal Transportation and Centering Ability of Wave One and SafeSider in Curved Root Canals Using Cone-Beam
Computed Tomography. J Res Dent Maxillofac Sci 2018; 3 (3) :1-8
URL: http://jrdms.dentaliau.ac.ir/article-1-208-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-208-en.html



1- Dentist
2- Assistant Professor, Endodontics Dept, Faculty of Dentistry, Tehran Medical Sciences, , ma_8498@yahoo.com
3- Assistant Professor, Department of Oral and Maxillofacial Radiology, Faculty of Dentistry,
4- Assistant Professor, Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences,
2- Assistant Professor, Endodontics Dept, Faculty of Dentistry, Tehran Medical Sciences, , ma_8498@yahoo.com
3- Assistant Professor, Department of Oral and Maxillofacial Radiology, Faculty of Dentistry,
4- Assistant Professor, Department of Endodontics, Faculty of Dentistry, Tehran Medical Sciences,
Keywords: Root Canal Preparation, Cone-Beam Computed
Tomography, Rotary instruments, Wave One, Safe Side
Full-Text [PDF 317 kb]
(1243 Downloads)
| Abstract (HTML) (3250 Views)
Abstract
Background and Aim: Maintaining the original central canal path during cleaning and shaping of the root canal system plays an important role in the success of endodontic treatment. This study sought to compare canal transportation and centering ability of WaveOne and SafeSider rotary files using cone-beam computed tomography (CBCT).
Materials and Methods: This in-vitro, experimental study was conducted on 40 mesiobuccal canals of extracted human mandibular first molars with 20° to 40° of curvature. The teeth were randomly divided into two groups (n=20) and mounted in putty. Next, preoperative CBCT scans were obtained. Root canals were prepared using primary file of WaveOne in group A and SafeSider system up to file #25/0.04 taper in group B. Postoperative CBCT scans were taken and cross-sectional images at 1, 3, and 7 mm distances from the anatomic apex were compared. Data were analyzed using t-test and two-way analysis of variance (ANOVA).
Results: WaveOne was significantly superior to SafeSider regarding the canal centering ability and caused significantly less canal transportation (P<0.001). The canal centering ability of both systems was higher at the coronal and middle thirds of the root compared to the apical region (P<0.05).
Conclusion: WaveOne, in contrast to SafeSider, has optimal canal centering ability and less transportation in curved root canals.
Keywords: Root Canal Preparation, Cone-Beam Computed Tomography, Dental Instruments, Stainless Steel, Equipment Design
Introduction
Efficient endodontic treatment requires the complete elimination of bacteria, debris, and necrotic tissues from the root canal system followed by proper shaping and irrigation and subsequent filling of the root canal. (1) In this process, it is important to shape the root canal in accordance with its original path. However, this is difficult to achieve in curved canals and may even result in procedural errors such as canal transportation, ledge formation or perforation. (2-4) These procedural errors occur for straight files tend to return to their straight shape in curved root canals.
Nickel-titanium (NiTi) rotary instruments were introduced to prevent the occurrence of procedural errors since these files have high flexibility and optimal canal centering ability. (1) They facilitate endodontic treatment and result in significantly less procedural errors, which further add to their popularity. (5) However, cyclic fatigue and fracture of these files have also been reported due to their overuse in curved and narrow root canals. (6,7)
Endodontic rotary instruments with reciprocating motion, such as WaveOne system, were later introduced with a lower risk of fracture in curved root canals. (8,9) However, the shaping ability and canal centering ability of recently introduced systems have not been well investigated. (10,11) In 2007, Yared described root canal preparation with a NiTi rotary file; although his emphasis was on the use of one single-file for root canal preparation, his study was unique in that he changed the movement of NiTi rotary files from a 360° rotational movement to back and forth motion. (12) In 2011, Dentsply Tulsa Specialties used Yared’s idea and introduced WaveOne system into the market. (13) The difference between this system and the previous rotary systems was in its back and forth clockwise and counterclockwise motion. This file is made of NiTi M-wire and its high flexibility preserves the root structure and decreases the risk of zipping of the canal while expediting the root canal preparation. (14)
SafeSider system, produced by Essential Dental Systems Inc., has a flat-sided design, which decreases involvement with dentin. SafeSider files have a high fracture resistance during root canal preparation. This system has eight stainless steel and three NiTi files, which are narrow and highly flexible due to their small cross-section and flat-sided design. (15)
Evaluation of the canal centering ability of rotary instruments is highly important to determine their efficacy and safety for use in curved root canals. Electron and light microscopy, micro-computed tomography, high resolution computed tomography and cone-beam computed tomography (CBCT) are used for the evaluation of the canal centering ability of files; (16,17) CBCT is a highly efficient imaging modality, which provides high-resolution, three-dimensional (3D) images, enabling evaluation of changes in the root canal system. Although CBCT has a lower spatial resolution than micro-computed tomography, it provides valuable information regarding the root canal morphology and fracture or changes in the root canal system with lower patient radiation dose than micro-computed tomography. (18,19)
Studies comparing canal centering ability of WaveOne and SafeSider in curved root canals are limited. Thus, this study sought to compare the canal centering ability of WaveOne and SafeSider in curved root canals using CBCT.
Materials and Methods
This ex-vivo, experimental study was conducted on 40 mandibular first molars. The teeth had been extracted for periodontal reasons and had closed apices with no canal calcification, no internal/external root resorption or root caries. Two samples as controls were subjected to primary CBCT scans in this study. They did not undergo root canal preparation and were subjected to postoperative CBCT scans with no manipulation. A special jig made using putty impression material was used to ensure the fixed position, reproducibility, and repeatability of testing and comparability of preoperative and postoperative images. All teeth had separate mesial canals such that a #10 K-file could pass through their apical foramen while a #15 K-file could not pass through their apices. Only teeth with root curvature between 20° to 40° and radius of curvature less than 5 cm were included. The sample size was calculated to be 40 teeth, according to a previous study. (20)
After collection, the teeth were sectioned at the cementoenamel junction (CEJ) to provide a root length of 16±1 mm and immersed in 5.25% sodium hypochlorite solution for one hour for disinfection. Debris and tissue residues were removed using a scaler and a sterile gauze, and the teeth were stored in saline.
Impressions were taken of teeth using putty impression material (Speedex; Coltene, Altstätten, Switzerland) with their roots completely embedded in putty. (21)
Care was taken not to introduce any file into the canal prior to taking preoperative CBCT scans to maintain the original canal anatomy. Also, metal restorations were removed (if present) to prevent metal artifacts.
Next, the teeth underwent CBCT (Rotograph Evo 3D; Villa Sistemi Medicali, Buccinasco MI, Italy) at 60 peak kilovoltage (kVp), 6 milliamperes (mA), and 11.2 seconds time with 0.5-mm slice thickness (0.166-mm voxel size). The CBCT unit used had 0.01-mm accuracy. Using OnDemand software (Cybermed Inc., Seoul, South Korea), sections were made at 1, 3, and 7 mm distances from the apex perpendicular to the longitudinal axis of the canal. All preoperative CBCT scans were obtained by one oral and maxillofacial radiologist. After taking preoperative CBCT scans, a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was introduced into the root canals until its tip was visible at the apex. Working length was determined 0.5 mm short of this length.
The teeth were then randomly divided into two groups (n=13) and their mesiobuccal root canals were prepared with WaveOne (Dentsply Maillefer, Ballaigues, Switzerland) in group A and SafeSider (Essential Dental Systems Inc., NJ, USA) in group B with the speed and torque recommended by the manufacturer.
In group A, root canals were shaped using WaveOne system with crown-down technique using a low-speed handpiece. Only one primary file (#25, 0.08 taper) was used at 250 rpm (revolutions per minute) and a 2.8-Ncm torque. The file was introduced into the canal passively with a gentle in-and-out motion until reaching the working length.
In group B, SafeSider system was used for root canal preparation, and #15 to #35 (0.02 taper) stainless steel files and then a #25 NiTi file (0.06 taper) were consecutively used in an Endo-Express handpiece at 2500 rpm. The files were used passively with gentle motion as recommended by the manufacturer.
In both groups, root canal patency was checked after using each rotary file with a #10 K-file. Each file was replaced with a new one after five canal preparations. After using each file, the canal was rinsed with 2 ml of 2.5% sodium hypochlorite solution with a 27-gauge needle. Samples were then stored in saline. To take postoperative CBCT scans, the teeth were placed in their respective putty impressions, and postoperative images were taken with the same exposure settings and conditions as for the preoperative scans.
Preoperative and postoperative cross-sectional images at 1, 3, and 7 mm distances from the apex were evaluated in the two groups using a software program. The distance between the root canal wall and external root surface was measured at the mesial and distal aspects on both preoperative and postoperative radiographs at 1, 3, and 7 mm distances from the apex (Figure 1). Measurements were made by two observers, and the mean of the values measured by the two observers was calculated and placed in the centering formula below:
or
Canal transportation was also determined using the formula (x2-x1)-(y2-y1), (22) where x1 is the shortest distance from the root surface to the root canal wall at the mesial aspect before preparation, x2 is the same distance after preparation, y1 is the shortest distance from the root surface to the root canal wall at the distal aspect before preparation, and y2 is the same distance after preparation. The canal centering ratio was also calculated using t-test. If the obtained value was 1, it indicated that the file was capable of perfectly maintaining the central canal path. The greater the deviations of this value from 1, the higher the deviation from the central canal path. The closer the transportation value to zero, the smaller the canal transportation. (23) Canal transportation and centering ability of the two systems were compared using t-test. Also, the mean duration of canal preparation at 1, 3, and 7 mm by each system was calculated, and the results were compared using t-test and repeated measures analysis of variance (ANOVA).
Results
Table 1 shows changes in the central canal path at 1, 3, and 7 mm from the apex following the use of WaveOne and SafeSider systems. As shown in Table 1, at 1, 3, and 7 mm from the apex, according to repeated measures ANOVA, the centering value in WaveOne group was greater than that in SafeSider system, and the difference was statistically significant (P=0.0012).
In WaveOne system, canal centering ability was greater at the coronal and middle thirds compared to the apical region, and this difference was statistically significant (P=0.01). The same was true for SafeSider (P=0.002).
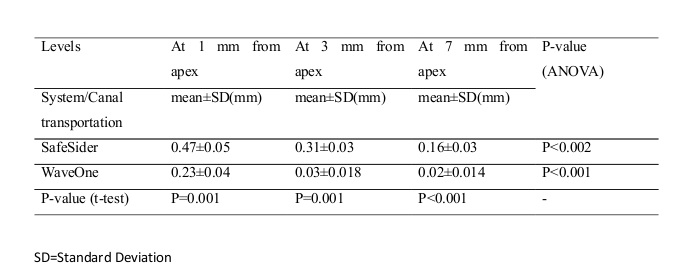
Table 2 shows the root canal transportation at 1, 3, and 7 mm distances from the apex in WaveOne and SafeSider groups. As seen in Table 2, at 1, 3, and 7 mm from the apex, the magnitude of transportation in SafeSider group was greater than the value in WaveOne group, and the difference was statistically significant (P=0.001, P=0.001, and P<0.001, respectively). Apical transportation was significantly greater at the middle and apical thirds compared to the coronal third in SafeSider system. However, apical transport in WaveOne system was significantly greater at the apical third compared to the middle and coronal thirds.
The mean duration of root canal preparation was 69±29.30 seconds in SafeSider and 47.09±16.54 seconds in WaveOne group. According to t-test, root canal preparation was significantly faster with WaveOne compared to SafeSider system (P<0.05).
Table 1. The centering ratios of SafeSider and WaveOne at different levels from the apex
Table 2. Amount of canal transportation in use of SafeSider and WaveOne at different levels from the apex
Figure 1. Schematic representation of the distance between the internal canal wall and external root surface before and after canal preparation.
Discussion
This study compared the canal transportation and centering ability of WaveOne and SafeSider in curved mesiobuccal root canals of mandibular molars at 1, 3, and 7 mm from the apex.
Root canal preparation is performed to eliminate debris and microorganisms from the root canal system; (1) however, deviation from the original central canal path, especially in the apical region, interferes with adequate cleaning, shaping, and filling of root canal and can result in treatment failure. (2)
Several rotary NiTi files have been introduced to overcome the limitations of stainless steel hand files in curved root canals. NiTi rotary instruments facilitate root canal preparation and decrease procedural errors. However, they may undergo cyclic fatigue and break in curved canals. (3) Reciprocating systems were recently introduced to overcome the shortcomings of NiTi systems. However, information about their root canal shaping efficacy is limited. (3) WaveOne and SafeSider reciprocating systems were compared in terms of canal centering ability in this study.
The efficacy of NiTi files in maintaining the central canal path can be evaluated by several methods, including radiographic comparison, (13) sectioning according to the Bramante’s method, (24) clearing of teeth, (25) high-resolution computed tomography, (16,26,27) micro-tomography, (22) and CBCT; (14) CBCT enables high-resolution, reproducible, and accurate 3D assessment of the root canal system without damaging the samples. (28)
Canal transportation can be assessed by two methods. Some researchers superimposed preoperative and postoperative images to assess changes in the canal path caused by root canal preparation. (29) Some others measured the distance from the external root surface to the internal root canal wall at the mesial and distal aspects on preoperative and postoperative images at three levels from the apex. (23,30) This method was also used in our study. Measurements were made at 1, 3, and 7 mm distances from the apex to evaluate changes at the apical and middle thirds of the root caused by preparation because the risk of procedural errors is higher at the apical and middle thirds of the root canal. Also, teeth with 20° to 40° of root curvatures were chosen for this study because they are at higher risks of procedural errors such as ledge formation, transportation, and perforation. (31) The results showed that both systems caused canal transportation, but the magnitude of canal transportation was significantly greater in SafeSider group, especially at 1 mm from the apex, and SafeSider had a poorer canal centering ability than WaveOne. Observing no transportation in the control samples confirmed the high accuracy of the imaging. The curvature of root canals was measured using Schneider’s method which is commonly used for this purpose. (11,32-34)
Our results showed that SafeSider caused greater canal transportation at the apical region compared to WaveOne. Also, SafeSider had a poor canal centering ability. The flat sides of SafeSider files are responsible for improved flexibility of stainless steel files. (11) Moreover, it is expected that the back and forth motion of these files creates a balanced force when inserted into the canal. (11) However, several studies have reported a significant canal transportation following the use of stainless steel files with back and forth motion. (33,34) Rhodes et al reported that SafeSider caused greater canal transportation compared to Vortex 06. (10) Also, many studies have supported the superiority of NiTi files to stainless steel instruments in maintaining root canal curvature. (33,35) Our current results also confirmed that WaveOne was superior to SafeSider in maintaining the original central path of the canal and preventing apical transportation. This finding is in accordance with the result of a study by Abu-Al Shawareb et al, in which WaveOne showed a lower percentage of danger zones and coronal narrowing incidence compared to SafeSider and K-files because larger sized stainless steel files in SafeSider system have more rigidity which increases canal straightening. (36)
Ceyhanli et al reported that canal transportation by SafeSider was greater than that of NiTi instrumentation system. (4) Also, in their study, SafeSider had lower canal centering ability. WaveOne operates with a back and forth motion to enhance root canal preparation. (9) Furthermore, only one file is required for root canal preparation to achieve adequate size and taper. Reciprocating motion applies balanced force to canal walls. (37) This motion decreases stress, fatigue, and locking of the file in canal walls and increases the ability to maintain the original root canal anatomy. (38,39) Previous studies have shown that use of one file with reciprocating motion results in a cleaning and shaping as effective as that obtained by the use of a complete series of rotary files. (40,41)
In our study, in both groups, canal transportation at 1 mm from the apex was significantly greater than that at 3 mm and 7 mm distances from the apex. Also, canal centering ability of both systems was lower at 1 mm from the apex compared to 3 mm and 7 mm levels; these findings were in agreement with those of Ceyhanli et al. (4) They also showed that SafeSider and WaveOne caused greater canal transportation at 1 mm from the apex, and canal transportation caused by SafeSider was greater than that caused by WaveOne.
Wu et al reported that apical transportation greater than 0.3 mm decreased the quality of the apical seal. (42) Our results are in accordance with those reported by Delgoshayi et al, showing that SafeSider system exceeded this critical threshold. (43) This highlights the need for further studies on this system. However, our results confirmed the results reported by Berutti et al, indicating that WaveOne did not exceed the critical threshold. (22)
The preparation time with WaveOne in our study was significantly shorter than that with SafeSider. The reason is the higher number of files used in SafeSider system. Future studies with larger sample sizes are required to evaluate the performance of SafeSider in terms of dentin removal and frequency of crack formation and file fracture. Also, WaveOne should be compared with other reciprocating files available in the market.
Conclusion
Based on the results, WaveOne, in contrast to SafeSider, is suitable for use in curved and narrow root canals since it has optimal canal centering ability and causes minimal canal transportation. Also, WaveOne was significantly faster than SafeSider for canal preparation, which further adds to the efficacy of WaveOne.
Full-Text: (989 Views)
Abstract
Background and Aim: Maintaining the original central canal path during cleaning and shaping of the root canal system plays an important role in the success of endodontic treatment. This study sought to compare canal transportation and centering ability of WaveOne and SafeSider rotary files using cone-beam computed tomography (CBCT).
Materials and Methods: This in-vitro, experimental study was conducted on 40 mesiobuccal canals of extracted human mandibular first molars with 20° to 40° of curvature. The teeth were randomly divided into two groups (n=20) and mounted in putty. Next, preoperative CBCT scans were obtained. Root canals were prepared using primary file of WaveOne in group A and SafeSider system up to file #25/0.04 taper in group B. Postoperative CBCT scans were taken and cross-sectional images at 1, 3, and 7 mm distances from the anatomic apex were compared. Data were analyzed using t-test and two-way analysis of variance (ANOVA).
Results: WaveOne was significantly superior to SafeSider regarding the canal centering ability and caused significantly less canal transportation (P<0.001). The canal centering ability of both systems was higher at the coronal and middle thirds of the root compared to the apical region (P<0.05).
Conclusion: WaveOne, in contrast to SafeSider, has optimal canal centering ability and less transportation in curved root canals.
Keywords: Root Canal Preparation, Cone-Beam Computed Tomography, Dental Instruments, Stainless Steel, Equipment Design
Introduction
Efficient endodontic treatment requires the complete elimination of bacteria, debris, and necrotic tissues from the root canal system followed by proper shaping and irrigation and subsequent filling of the root canal. (1) In this process, it is important to shape the root canal in accordance with its original path. However, this is difficult to achieve in curved canals and may even result in procedural errors such as canal transportation, ledge formation or perforation. (2-4) These procedural errors occur for straight files tend to return to their straight shape in curved root canals.
Nickel-titanium (NiTi) rotary instruments were introduced to prevent the occurrence of procedural errors since these files have high flexibility and optimal canal centering ability. (1) They facilitate endodontic treatment and result in significantly less procedural errors, which further add to their popularity. (5) However, cyclic fatigue and fracture of these files have also been reported due to their overuse in curved and narrow root canals. (6,7)
Endodontic rotary instruments with reciprocating motion, such as WaveOne system, were later introduced with a lower risk of fracture in curved root canals. (8,9) However, the shaping ability and canal centering ability of recently introduced systems have not been well investigated. (10,11) In 2007, Yared described root canal preparation with a NiTi rotary file; although his emphasis was on the use of one single-file for root canal preparation, his study was unique in that he changed the movement of NiTi rotary files from a 360° rotational movement to back and forth motion. (12) In 2011, Dentsply Tulsa Specialties used Yared’s idea and introduced WaveOne system into the market. (13) The difference between this system and the previous rotary systems was in its back and forth clockwise and counterclockwise motion. This file is made of NiTi M-wire and its high flexibility preserves the root structure and decreases the risk of zipping of the canal while expediting the root canal preparation. (14)
SafeSider system, produced by Essential Dental Systems Inc., has a flat-sided design, which decreases involvement with dentin. SafeSider files have a high fracture resistance during root canal preparation. This system has eight stainless steel and three NiTi files, which are narrow and highly flexible due to their small cross-section and flat-sided design. (15)
Evaluation of the canal centering ability of rotary instruments is highly important to determine their efficacy and safety for use in curved root canals. Electron and light microscopy, micro-computed tomography, high resolution computed tomography and cone-beam computed tomography (CBCT) are used for the evaluation of the canal centering ability of files; (16,17) CBCT is a highly efficient imaging modality, which provides high-resolution, three-dimensional (3D) images, enabling evaluation of changes in the root canal system. Although CBCT has a lower spatial resolution than micro-computed tomography, it provides valuable information regarding the root canal morphology and fracture or changes in the root canal system with lower patient radiation dose than micro-computed tomography. (18,19)
Studies comparing canal centering ability of WaveOne and SafeSider in curved root canals are limited. Thus, this study sought to compare the canal centering ability of WaveOne and SafeSider in curved root canals using CBCT.
Materials and Methods
This ex-vivo, experimental study was conducted on 40 mandibular first molars. The teeth had been extracted for periodontal reasons and had closed apices with no canal calcification, no internal/external root resorption or root caries. Two samples as controls were subjected to primary CBCT scans in this study. They did not undergo root canal preparation and were subjected to postoperative CBCT scans with no manipulation. A special jig made using putty impression material was used to ensure the fixed position, reproducibility, and repeatability of testing and comparability of preoperative and postoperative images. All teeth had separate mesial canals such that a #10 K-file could pass through their apical foramen while a #15 K-file could not pass through their apices. Only teeth with root curvature between 20° to 40° and radius of curvature less than 5 cm were included. The sample size was calculated to be 40 teeth, according to a previous study. (20)
After collection, the teeth were sectioned at the cementoenamel junction (CEJ) to provide a root length of 16±1 mm and immersed in 5.25% sodium hypochlorite solution for one hour for disinfection. Debris and tissue residues were removed using a scaler and a sterile gauze, and the teeth were stored in saline.
Impressions were taken of teeth using putty impression material (Speedex; Coltene, Altstätten, Switzerland) with their roots completely embedded in putty. (21)
Care was taken not to introduce any file into the canal prior to taking preoperative CBCT scans to maintain the original canal anatomy. Also, metal restorations were removed (if present) to prevent metal artifacts.
Next, the teeth underwent CBCT (Rotograph Evo 3D; Villa Sistemi Medicali, Buccinasco MI, Italy) at 60 peak kilovoltage (kVp), 6 milliamperes (mA), and 11.2 seconds time with 0.5-mm slice thickness (0.166-mm voxel size). The CBCT unit used had 0.01-mm accuracy. Using OnDemand software (Cybermed Inc., Seoul, South Korea), sections were made at 1, 3, and 7 mm distances from the apex perpendicular to the longitudinal axis of the canal. All preoperative CBCT scans were obtained by one oral and maxillofacial radiologist. After taking preoperative CBCT scans, a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was introduced into the root canals until its tip was visible at the apex. Working length was determined 0.5 mm short of this length.
The teeth were then randomly divided into two groups (n=13) and their mesiobuccal root canals were prepared with WaveOne (Dentsply Maillefer, Ballaigues, Switzerland) in group A and SafeSider (Essential Dental Systems Inc., NJ, USA) in group B with the speed and torque recommended by the manufacturer.
In group A, root canals were shaped using WaveOne system with crown-down technique using a low-speed handpiece. Only one primary file (#25, 0.08 taper) was used at 250 rpm (revolutions per minute) and a 2.8-Ncm torque. The file was introduced into the canal passively with a gentle in-and-out motion until reaching the working length.
In group B, SafeSider system was used for root canal preparation, and #15 to #35 (0.02 taper) stainless steel files and then a #25 NiTi file (0.06 taper) were consecutively used in an Endo-Express handpiece at 2500 rpm. The files were used passively with gentle motion as recommended by the manufacturer.
In both groups, root canal patency was checked after using each rotary file with a #10 K-file. Each file was replaced with a new one after five canal preparations. After using each file, the canal was rinsed with 2 ml of 2.5% sodium hypochlorite solution with a 27-gauge needle. Samples were then stored in saline. To take postoperative CBCT scans, the teeth were placed in their respective putty impressions, and postoperative images were taken with the same exposure settings and conditions as for the preoperative scans.
Preoperative and postoperative cross-sectional images at 1, 3, and 7 mm distances from the apex were evaluated in the two groups using a software program. The distance between the root canal wall and external root surface was measured at the mesial and distal aspects on both preoperative and postoperative radiographs at 1, 3, and 7 mm distances from the apex (Figure 1). Measurements were made by two observers, and the mean of the values measured by the two observers was calculated and placed in the centering formula below:
or
Canal transportation was also determined using the formula (x2-x1)-(y2-y1), (22) where x1 is the shortest distance from the root surface to the root canal wall at the mesial aspect before preparation, x2 is the same distance after preparation, y1 is the shortest distance from the root surface to the root canal wall at the distal aspect before preparation, and y2 is the same distance after preparation. The canal centering ratio was also calculated using t-test. If the obtained value was 1, it indicated that the file was capable of perfectly maintaining the central canal path. The greater the deviations of this value from 1, the higher the deviation from the central canal path. The closer the transportation value to zero, the smaller the canal transportation. (23) Canal transportation and centering ability of the two systems were compared using t-test. Also, the mean duration of canal preparation at 1, 3, and 7 mm by each system was calculated, and the results were compared using t-test and repeated measures analysis of variance (ANOVA).
Results
Table 1 shows changes in the central canal path at 1, 3, and 7 mm from the apex following the use of WaveOne and SafeSider systems. As shown in Table 1, at 1, 3, and 7 mm from the apex, according to repeated measures ANOVA, the centering value in WaveOne group was greater than that in SafeSider system, and the difference was statistically significant (P=0.0012).
In WaveOne system, canal centering ability was greater at the coronal and middle thirds compared to the apical region, and this difference was statistically significant (P=0.01). The same was true for SafeSider (P=0.002).
Table 2 shows the root canal transportation at 1, 3, and 7 mm distances from the apex in WaveOne and SafeSider groups. As seen in Table 2, at 1, 3, and 7 mm from the apex, the magnitude of transportation in SafeSider group was greater than the value in WaveOne group, and the difference was statistically significant (P=0.001, P=0.001, and P<0.001, respectively). Apical transportation was significantly greater at the middle and apical thirds compared to the coronal third in SafeSider system. However, apical transport in WaveOne system was significantly greater at the apical third compared to the middle and coronal thirds.
The mean duration of root canal preparation was 69±29.30 seconds in SafeSider and 47.09±16.54 seconds in WaveOne group. According to t-test, root canal preparation was significantly faster with WaveOne compared to SafeSider system (P<0.05).
Table 1. The centering ratios of SafeSider and WaveOne at different levels from the apex
{kind=link}
Table 2. Amount of canal transportation in use of SafeSider and WaveOne at different levels from the apex
{kind=link}
Figure 1. Schematic representation of the distance between the internal canal wall and external root surface before and after canal preparation.
{kind=link}
Discussion
This study compared the canal transportation and centering ability of WaveOne and SafeSider in curved mesiobuccal root canals of mandibular molars at 1, 3, and 7 mm from the apex.
Root canal preparation is performed to eliminate debris and microorganisms from the root canal system; (1) however, deviation from the original central canal path, especially in the apical region, interferes with adequate cleaning, shaping, and filling of root canal and can result in treatment failure. (2)
Several rotary NiTi files have been introduced to overcome the limitations of stainless steel hand files in curved root canals. NiTi rotary instruments facilitate root canal preparation and decrease procedural errors. However, they may undergo cyclic fatigue and break in curved canals. (3) Reciprocating systems were recently introduced to overcome the shortcomings of NiTi systems. However, information about their root canal shaping efficacy is limited. (3) WaveOne and SafeSider reciprocating systems were compared in terms of canal centering ability in this study.
The efficacy of NiTi files in maintaining the central canal path can be evaluated by several methods, including radiographic comparison, (13) sectioning according to the Bramante’s method, (24) clearing of teeth, (25) high-resolution computed tomography, (16,26,27) micro-tomography, (22) and CBCT; (14) CBCT enables high-resolution, reproducible, and accurate 3D assessment of the root canal system without damaging the samples. (28)
Canal transportation can be assessed by two methods. Some researchers superimposed preoperative and postoperative images to assess changes in the canal path caused by root canal preparation. (29) Some others measured the distance from the external root surface to the internal root canal wall at the mesial and distal aspects on preoperative and postoperative images at three levels from the apex. (23,30) This method was also used in our study. Measurements were made at 1, 3, and 7 mm distances from the apex to evaluate changes at the apical and middle thirds of the root caused by preparation because the risk of procedural errors is higher at the apical and middle thirds of the root canal. Also, teeth with 20° to 40° of root curvatures were chosen for this study because they are at higher risks of procedural errors such as ledge formation, transportation, and perforation. (31) The results showed that both systems caused canal transportation, but the magnitude of canal transportation was significantly greater in SafeSider group, especially at 1 mm from the apex, and SafeSider had a poorer canal centering ability than WaveOne. Observing no transportation in the control samples confirmed the high accuracy of the imaging. The curvature of root canals was measured using Schneider’s method which is commonly used for this purpose. (11,32-34)
Our results showed that SafeSider caused greater canal transportation at the apical region compared to WaveOne. Also, SafeSider had a poor canal centering ability. The flat sides of SafeSider files are responsible for improved flexibility of stainless steel files. (11) Moreover, it is expected that the back and forth motion of these files creates a balanced force when inserted into the canal. (11) However, several studies have reported a significant canal transportation following the use of stainless steel files with back and forth motion. (33,34) Rhodes et al reported that SafeSider caused greater canal transportation compared to Vortex 06. (10) Also, many studies have supported the superiority of NiTi files to stainless steel instruments in maintaining root canal curvature. (33,35) Our current results also confirmed that WaveOne was superior to SafeSider in maintaining the original central path of the canal and preventing apical transportation. This finding is in accordance with the result of a study by Abu-Al Shawareb et al, in which WaveOne showed a lower percentage of danger zones and coronal narrowing incidence compared to SafeSider and K-files because larger sized stainless steel files in SafeSider system have more rigidity which increases canal straightening. (36)
Ceyhanli et al reported that canal transportation by SafeSider was greater than that of NiTi instrumentation system. (4) Also, in their study, SafeSider had lower canal centering ability. WaveOne operates with a back and forth motion to enhance root canal preparation. (9) Furthermore, only one file is required for root canal preparation to achieve adequate size and taper. Reciprocating motion applies balanced force to canal walls. (37) This motion decreases stress, fatigue, and locking of the file in canal walls and increases the ability to maintain the original root canal anatomy. (38,39) Previous studies have shown that use of one file with reciprocating motion results in a cleaning and shaping as effective as that obtained by the use of a complete series of rotary files. (40,41)
In our study, in both groups, canal transportation at 1 mm from the apex was significantly greater than that at 3 mm and 7 mm distances from the apex. Also, canal centering ability of both systems was lower at 1 mm from the apex compared to 3 mm and 7 mm levels; these findings were in agreement with those of Ceyhanli et al. (4) They also showed that SafeSider and WaveOne caused greater canal transportation at 1 mm from the apex, and canal transportation caused by SafeSider was greater than that caused by WaveOne.
Wu et al reported that apical transportation greater than 0.3 mm decreased the quality of the apical seal. (42) Our results are in accordance with those reported by Delgoshayi et al, showing that SafeSider system exceeded this critical threshold. (43) This highlights the need for further studies on this system. However, our results confirmed the results reported by Berutti et al, indicating that WaveOne did not exceed the critical threshold. (22)
The preparation time with WaveOne in our study was significantly shorter than that with SafeSider. The reason is the higher number of files used in SafeSider system. Future studies with larger sample sizes are required to evaluate the performance of SafeSider in terms of dentin removal and frequency of crack formation and file fracture. Also, WaveOne should be compared with other reciprocating files available in the market.
Conclusion
Based on the results, WaveOne, in contrast to SafeSider, is suitable for use in curved and narrow root canals since it has optimal canal centering ability and causes minimal canal transportation. Also, WaveOne was significantly faster than SafeSider for canal preparation, which further adds to the efficacy of WaveOne.
Type of Study: Original article |
Subject:
Radiology
References
1. 1. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974 Apr;18(2):269-96.
2. Abou-Rass M, Frank AL, Glick DH. The anticurvature filing method to prepare the curved root canal. J Am Dent Assoc. 1980 Now;101(5):792-4. [DOI:10.14219/jada.archive.1980.0427] [PMID]
3. Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005 Oct;38(10):743-52. [DOI:10.1111/j.1365-2591.2005.01010.x] [PMID]
4. Ceyhanli KT, Erdilek N, Tatar I, Cetintav B. Comparative micro-computed tomography evaluation of apical root canal transportation with the use of ProTaper, RaCe and Safesider systems in human teeth. Aust Endod J. 2014 Apr;40(1):12-6. [DOI:10.1111/aej.12014] [PMID]
5. Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001 Sep;34(6):476-84. [DOI:10.1046/j.1365-2591.2001.00422.x] [PMID]
6. Pruett JP, Clement DJ, Carnes DL, Jr. Cyclic fatigue testing of nickel-titanium endodontic instruments. J Endod. 1997 Feb;23(2):77-85. [DOI:10.1016/S0099-2399(97)80250-6]
7. Haikel Y, Serfaty R, Bateman G, Senger B, Allemann C. Dynamic and cyclic fatigue of engine-driven rotary nickel-titanium endodontic instruments. J Endod. 1999 Jun;25(6):434-40. [DOI:10.1016/S0099-2399(99)80274-X]
8. You SY, Bae KS, Baek SH, Kum KY, Shon WJ, Lee W. Lifespan of one nickel-titanium rotary file with reciprocating motion in curved root canals. J Endod. 2010 Dec;36(12):1991-4. [DOI:10.1016/j.joen.2010.08.040] [PMID]
9. De-Deus G, Moreira EJ, Lopes HP, Elias CN. Extended cyclic fatigue life of F2 ProTaper instruments used in reciprocating movement. Int Endod J. 2010 Dec;43(12):1063-8. [DOI:10.1111/j.1365-2591.2010.01756.x] [PMID]
10. Rhodes SC, Hulsmann M, McNeal SF, Beck P, Eleazer PD. Comparison of root canal preparation using reciprocating Safesiders stainless steel and Vortex nickel-titanium instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 May;111(5):659-67. [DOI:10.1016/j.tripleo.2010.11.021] [PMID]
11. You SY, Kim HC, Bae KS, Baek SH, Kum KY, Lee W. Shaping ability of reciprocating motion in curved root canals: a comparative study with micro-computed tomography. J Endod. 2011 Sep;37(9):1296-300. [DOI:10.1016/j.joen.2011.05.021] [PMID]
12. Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J. 2008 Apr;41(4):339-44. [DOI:10.1111/j.1365-2591.2007.01351.x] [PMID]
13. Tofangchiha M, Adel M, Bakhshi M, Esfehani M, Nazeman P, Ghorbani Elizeyi M, et al. Digital radiography with computerized conventional monitors compared to medical monitors in vertical root fracture diagnosis. Iran Endod J. 2013 Winter;8(1):14-7.
14. Webber J, Machtou P, Pertot W, Kuttler S, Ruddle C, West J. The WaveOne single-file reciprocating system. Roots. 2011;1(1):28-33.
15. Musikant BL, Cohen BI, Deutsch AS. Comparison instrumentation reamers and files versus a flat-sided design of conventional noninterrupted, flat-sided design. J Endod. 2004 Feb;30(2):107-9. [DOI:10.1097/00004770-200402000-00011] [PMID]
16. Sydney GB, Batista A, de Melo LL. The radiographic platform: a new method to evaluate root canal preparation in vitro. J Endod. 1991 Nov;17(11):570-2. [DOI:10.1016/S0099-2399(06)81724-3]
17. Peters OA, Peters CI, Schonenberger K, Barbakow F. ProTaper rotary root canal preparation: effects of canal anatomy on final shape analysed by micro CT. Int Endod J. 2003 Feb;36(2):86-92. [DOI:10.1046/j.1365-2591.2003.00626.x] [PMID]
18. Hartmann MS, Barletta FB, Camargo Fontanella VR, Vanni JR. Canal transportation after root canal instrumentation: a comparative study with computed tomography. J Endod. 2007 Aug;33(8):962-5. [DOI:10.1016/j.joen.2007.03.019] [PMID]
19. Bernardes RA, Rocha EA, Duarte MA, Vivan RR, de Moraes IG, Bramante AS, et al. Root canal area increase promoted by the EndoSequence and ProTaper systems: comparison by computed tomography. J Endod. 2010 Jul;36(7):1179-82. [DOI:10.1016/j.joen.2009.12.033] [PMID]
20. Madani Z, Soleymani A, Bagheri T, Moudi E, Bijani A, Rakhshan V. Transportation and Centering Ability of Neoniti and ProTaper Instruments; A CBCT Assessment. Iran Endod J. 2017 Winter;12(1):43-9.
21. Khademi A, Yazdizadeh M, Feizianfard M. Determination of the minimum instrumentation size for penetration of irrigants to the apical third of root canal systems. J Endod. 2006 May;32(5):417-20. [DOI:10.1016/j.joen.2005.11.008] [PMID]
22. Berutti E, Chiandussi G, Paolino DS, Scotti N, Cantatore G, Castellucci A, et al. Canal shaping with WaveOne Primary reciprocating files and ProTaper system: a comparative study. J Endod. 2012 Apr;38(4):505-9. [DOI:10.1016/j.joen.2011.12.040] [PMID]
23. Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996 Jul;22(7):369-75. [DOI:10.1016/S0099-2399(96)80221-4]
24. Bramante CM, Berbert A, Borges RP. A methodology for evaluation of root canal instrumentation. J Endod. 1987 May;13(5):243-5. [DOI:10.1016/S0099-2399(87)80099-7]
25. Barthel CR, Gruber S, Roulet JF. A new method to assess the results of instrumentation techniques in the root canal. J Endod. 1999 Aug;25(8):535-8. [DOI:10.1016/S0099-2399(99)80374-4]
26. Gergi R, Rjeily JA, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J Endod. 2010 May;36(5):904-7. [DOI:10.1016/j.joen.2009.12.038] [PMID]
27. Estrela C, Bueno MR, Sousa-Neto MD, Pécora JD. Method for determination of root curvature radius using cone-beam computed tomography images. Braz Dent J. 2008;19(2):114-8. [DOI:10.1590/S0103-64402008000200005] [PMID]
28. Hashem AA, Ghoneim AG, Lutfy RA, Foda MY, Omar GA. Geometric analysis of root canals prepared by four rotary NiTi shaping systems. J Endod. 2012 Jul;38(7):996-1000. [DOI:10.1016/j.joen.2012.03.018] [PMID]
29. Özer SY. Comparison of root canal transportation induced by three rotary systems with noncutting tips using computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Feb;111(2):244-50. [DOI:10.1016/j.tripleo.2010.08.017] [PMID]
30. Freire LG, Gavini G, Branco-Barletta F, Sanches-Cunha R, dos Santos M. Microscopic computerized tomographic evaluation of root canal transportation prepared with twisted or ground nickel-titanium rotary instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Dec;112(6):e143-8. [DOI:10.1016/j.tripleo.2011.06.029] [PMID]
31. Taşdemir T, Aydemir H, Inan U, Unal O. Canal preparation with Hero 642 rotary Ni-Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int Endod J. 2005 Jun;38(6):402-8. [DOI:10.1111/j.1365-2591.2005.00961.x] [PMID]
32. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971 aug;32(2):271-5. [DOI:10.1016/0030-4220(71)90230-1]
33. Paqué F, Barbakow F, Peters OA. Root canal preparation with Endo-Eze AET: changes in root canal shape assessed by micro-computed tomography. Int Endod J. 2005 Jul;38(7):456-64. [DOI:10.1111/j.1365-2591.2005.00968.x] [PMID]
34. Frank AL. An evaluation of the Giromatic endodontic handpiece. Oral Surg Oral Med Oral Pathol. 1967 Sep;24(3):419-21. [DOI:10.1016/0030-4220(67)90082-5]
35. Hülsmann M, Schade M, Schafers F. A comparative study of root canal preparation with HERO 642 and Quantec SC rotary Ni-Ti instruments. Int Endod J. 2001 Oct;34(7):538-46. [DOI:10.1046/j.1365-2591.2001.00431.x] [PMID]
36. Abu-Al Shawareb SA, Saeed MH, Al Hadi DZ. The shaping ability of two reciprocating file systems in s-shaped simulated root canals. Int J Recent Sci Res. 2016;7(11):14222-9.
37. Roane JB, Sabala CL, Duncanson MG Jr. The "balanced force" concept for instrumentation of curved canals. J Endod. 1985 May;11(5):203-11. [DOI:10.1016/S0099-2399(85)80061-3]
38. Southard DW, Oswald RJ, Natkin E. Instrumentation of curved molar root canals with the Roane technique. J Endod. 1987 Oct;13(10):479-89. [DOI:10.1016/S0099-2399(87)80015-8]
39. Roane JB, Sabala C. Clockwise or counterclockwise. J Endod. 1984 Aug;10(8):349-53. [DOI:10.1016/S0099-2399(84)80153-3]
40. Paqué F, Zehnder M, De-Deus G. Microtomography-based comparison of reciprocating single-file F2 ProTaper technique versus rotary full sequence. J Endod. 2011 Oct;37(10):1394-7. [DOI:10.1016/j.joen.2011.06.031] [PMID]
41. De-Deus G, Barino B, Zamolyi RQ, Souza E, Fonseca A Jr., Fidel S, et al. Suboptimal debridement quality produced by the single-file F2 ProTaper technique in oval-shaped canals. J Endod. 2010 Nov;36(11):1897-900. [DOI:10.1016/j.joen.2010.08.009] [PMID]
42. Wu MK, Fan B, Wesselink PR. Leakage along apical root fillings in curved root canals. Part I: effects of apical transportation on seal of root fillings. J Endod. 2000 Apr;26(4):210-6. [DOI:10.1097/00004770-200004000-00003] [PMID]
43. Delgoshayi N, Abbasi M, Bakhtiar H, Sakhdari S, Ghannad S, Ellini MR. Canal Transportation and Centering Ability of ProTaper and SafeSider in Preparation of Curved Root Canals: A CBCT Evaluation. Iran Endod J. 2018 Spring;13(2):240-5.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
