

Volume 3, Issue 3 (8-2018)
J Res Dent Maxillofac Sci 2018, 3(3): 33-41 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khalifeh S, Rezaee E, Azizi A, Ebrahimi H. Efficacy of Low-Level Laser Versus Transcutaneous Electrical Nerve Stimulation for Treatment of Myofascial Pain Syndrome: A Clinical Trial. J Res Dent Maxillofac Sci 2018; 3 (3) :33-41
URL: http://jrdms.dentaliau.ac.ir/article-1-207-en.html
URL: http://jrdms.dentaliau.ac.ir/article-1-207-en.html



1- Dentist
2- Assistant professor, Oral Medicine Dept, Faculty of Dentistry, Tehran Medical Sciences,
3- Professor, Oral Medicine Dept, Faculty of Dentistry, Tehran Medical Sciences,
2- Assistant professor, Oral Medicine Dept, Faculty of Dentistry, Tehran Medical Sciences,
3- Professor, Oral Medicine Dept, Faculty of Dentistry, Tehran Medical Sciences,
Keywords: Myofascial Pain Syndromes, Transcutaneous Electrical Nerve Stimulation, Low-Level Laser Therapy
Full-Text [PDF 329 kb]
(1256 Downloads)
| Abstract (HTML) (3563 Views)
Abstract
Background and Aim: Myofascial pain syndrome (MPS) is the most common cause of facial muscle pain. This study sought to assess the efficacy of transcutaneous electrical nerve stimulation (TENS) and low-level laser (LLL) for treatment of MPS in comparison with a sham laser control group.
Materials and Methods: In this randomized controlled clinical trial, 55 MPS patients between 18-60 years old were randomly assigned to TENS, LLL (810 nm) or sham laser group. At the onset of treatment, 500 mg of methocarbamol and 250 mg of naproxen t.i.d. were prescribed for 10 days as the standard treatment protocol. Tenderness and pain of major muscles of mastication, minor muscles, and temporomandibular joint (TMJ) were evaluated using a visual analog scale (VAS). Maximum mouth opening and deviation and deflection of the jaw were also evaluated before and one month after the intervention. Data were analyzed using Kruskal-Wallis test and non-parametric Dunn’s test.
Results: Pain severity (VAS score) in the masseter, lateral pterygoid, and trapezius muscles (at the side of greater involvement) significantly decreased in both TENS and LLL groups after the treatment. In the sternocleidomastoid (SCM) and anterior temporalis muscles, significant pain reduction only occurred in LLL group. Mouth opening significantly increased in TENS group and decreased in LLL group. TMJ pain significantly decreased only in TENS group.
Conclusion: Both TENS and LLL were efficient for treatment of MPS; however, the efficacy of TENS was found to be slightly higher than that of LLL.
Keywords: Myofascial Pain Syndromes, Transcutaneous Electrical Nerve Stimulation, Low-Level Laser Therapy
Introduction
Myofascial pain syndrome (MPS) is the most common cause of facial muscle pain; patients suffering from MPS often complain of pain, jaw movement limitation, and tenderness of the muscles of mastication. (1) MPS is the most common muscle disorder in patients suffering from temporomandibular disorders (TMDs). (2) Late diagnosis or insufficient treatment of MPS may lead to its progression to chronic complex pain. (3) The gnathological theory was first suggested in the 1920s, discussing the causes and treatment of TMDs. (4) The myotomal pain referral patterns were later described by Kellgren in the 1930s, which became the cornerstone of diagnosis of referred pain of facial muscles. (5) Facial muscle pain can interrupt daily activities and decrease the quality of life of patients similar to other chronic pains. (2)
Several modalities are currently used for treatment of MPS such as occlusal adjustment, self-help behavior therapy, physiotherapy, transcutaneous electrical nerve stimulation (TENS), low-level laser therapy (LLLT), use of intraoral appliances, pharmaceutical therapy, relaxation methods, trigger point technique, and acupuncture. (2)
LLLT is performed to enhance tissue repair, to decrease pain, and to reduce inflammation; this phenomenon is technically known as photobiomodulation therapy. Laser enhances the treatment goals in organismal, systemic, cellular, and subcellular levels. In the clinical setting, LLLT is used mainly for tissue repair and pain control. LLL induces mitochondrial activity and tissue regeneration by increasing cell turnover, selective absorption, nerve injury repair, angiogenesis, controlling inflammation, vasodilation, release of endogenous endorphins, increasing the oxygen supply, and changing the permeability of tissues. (6-14) Although the exact mechanism of analgesia by laser has yet to be fully understood, some in-vitro studies have shown that LLLT inhibits the cyclooxygenase 2 synthesis and prevents the conversion of arachidonic acid to prostaglandins E2 and F2 and thromboxane, resulting in analgesia. (15) Some clinical studies have concluded that increased level of beta-endorphin in the central nervous system and the consequently increased pain threshold are the main mechanisms of analgesia by laser application. (15) In 2013, de Godoy et al evaluated the efficacy of LLLT for treatment of TMD and reported that this modality decreased pain and inflammation and enhanced tissue repair. (16)
TENS is a non-pharmaceutical and non-invasive method of pain control; it reduces pain via both peripheral and central mechanisms. (17) In the central mechanism, TENS activates some opioid, serotonin and muscarinic receptors in the spinal cord and the brain stem. In the peripheral mechanism, opioid and alpha2 noradrenergic receptors at the site of TENS are stimulated and induce analgesia. (17) In 2005, Kato et al compared the efficacy of TENS and LLLT and found that both modalities were effective for treatment of TMD. (17)
Many studies have evaluated the efficacy of different modalities for treatment of MPS, reporting variable, and sometimes, controversial results. (1-3,15-23) Considering the existing controversy in the efficacy of MPS treatments, this study sought to assess the efficacy of TENS and LLL for treatment of MPS in comparison with a sham laser.
Materials and Methods
This randomized controlled clinical trial was conducted on MPS patients presenting to the Oral Medicine Department of Islamic Azad University, Dental Faculty, and to the TMJ Department of School of Dentistry of Tehran University of Medical Sciences.
The inclusion criteria were the age range of 18 to 60 years, diagnosis of MPS based on its signs and symptoms, signing the written informed consent form, having not more than three missing teeth in each jaw (not replaced), and no receipt of treatment for MPS in the past two weeks.
The exclusion criteria were pregnancy, psychological conditions, and depression for which patients took medications, (1,2,12,19) missing of more than three teeth in each jaw (not replaced), except for the third molars, ages below 18 and over 60 years, systemic diseases other than MPS, (24) contraindication for laser therapy or TENS, (2) contraindication for administration of methocarbamol or naproxen, (2) and history of receiving MPS treatment in the past two weeks. (1,12,19)
Based on previous studies and a pilot study (power of 80), the sample size was calculated to be 60 patients. Sampling was sequential randomized, and patients who met the inclusion criteria were randomly assigned to the test or control groups. Sampling was continued until the sample size was reached.
The study protocol was approved in the Committee of Medical Ethics of Islamic Azad University, Dental Faculty and registered in the Iranian Registry of Clinical Trials (Code: IRCT2014022116660N1r2). The study was thoroughly explained to patients and they all signed written informed consent forms.
Patients complaining of pain in the muscles of mastication and tenderness in at least one of the four major muscles of mastication (medial pterygoid, lateral pterygoid, anterior temporalis, and masseter) were diagnosed as having MPS. The pain in MPS often has a trigger point and is referral. These patients may suffer from impaired mastication or speech due to muscle contraction subsequent to pain. Other possible symptoms include mouth opening limitation, jaw deviation, articular sounds, neck pain, earache, and headache. (2) Clinical examination included the followings:
Full-Text: (1140 Views)
Abstract
Background and Aim: Myofascial pain syndrome (MPS) is the most common cause of facial muscle pain. This study sought to assess the efficacy of transcutaneous electrical nerve stimulation (TENS) and low-level laser (LLL) for treatment of MPS in comparison with a sham laser control group.
Materials and Methods: In this randomized controlled clinical trial, 55 MPS patients between 18-60 years old were randomly assigned to TENS, LLL (810 nm) or sham laser group. At the onset of treatment, 500 mg of methocarbamol and 250 mg of naproxen t.i.d. were prescribed for 10 days as the standard treatment protocol. Tenderness and pain of major muscles of mastication, minor muscles, and temporomandibular joint (TMJ) were evaluated using a visual analog scale (VAS). Maximum mouth opening and deviation and deflection of the jaw were also evaluated before and one month after the intervention. Data were analyzed using Kruskal-Wallis test and non-parametric Dunn’s test.
Results: Pain severity (VAS score) in the masseter, lateral pterygoid, and trapezius muscles (at the side of greater involvement) significantly decreased in both TENS and LLL groups after the treatment. In the sternocleidomastoid (SCM) and anterior temporalis muscles, significant pain reduction only occurred in LLL group. Mouth opening significantly increased in TENS group and decreased in LLL group. TMJ pain significantly decreased only in TENS group.
Conclusion: Both TENS and LLL were efficient for treatment of MPS; however, the efficacy of TENS was found to be slightly higher than that of LLL.
Keywords: Myofascial Pain Syndromes, Transcutaneous Electrical Nerve Stimulation, Low-Level Laser Therapy
Introduction
Myofascial pain syndrome (MPS) is the most common cause of facial muscle pain; patients suffering from MPS often complain of pain, jaw movement limitation, and tenderness of the muscles of mastication. (1) MPS is the most common muscle disorder in patients suffering from temporomandibular disorders (TMDs). (2) Late diagnosis or insufficient treatment of MPS may lead to its progression to chronic complex pain. (3) The gnathological theory was first suggested in the 1920s, discussing the causes and treatment of TMDs. (4) The myotomal pain referral patterns were later described by Kellgren in the 1930s, which became the cornerstone of diagnosis of referred pain of facial muscles. (5) Facial muscle pain can interrupt daily activities and decrease the quality of life of patients similar to other chronic pains. (2)
Several modalities are currently used for treatment of MPS such as occlusal adjustment, self-help behavior therapy, physiotherapy, transcutaneous electrical nerve stimulation (TENS), low-level laser therapy (LLLT), use of intraoral appliances, pharmaceutical therapy, relaxation methods, trigger point technique, and acupuncture. (2)
LLLT is performed to enhance tissue repair, to decrease pain, and to reduce inflammation; this phenomenon is technically known as photobiomodulation therapy. Laser enhances the treatment goals in organismal, systemic, cellular, and subcellular levels. In the clinical setting, LLLT is used mainly for tissue repair and pain control. LLL induces mitochondrial activity and tissue regeneration by increasing cell turnover, selective absorption, nerve injury repair, angiogenesis, controlling inflammation, vasodilation, release of endogenous endorphins, increasing the oxygen supply, and changing the permeability of tissues. (6-14) Although the exact mechanism of analgesia by laser has yet to be fully understood, some in-vitro studies have shown that LLLT inhibits the cyclooxygenase 2 synthesis and prevents the conversion of arachidonic acid to prostaglandins E2 and F2 and thromboxane, resulting in analgesia. (15) Some clinical studies have concluded that increased level of beta-endorphin in the central nervous system and the consequently increased pain threshold are the main mechanisms of analgesia by laser application. (15) In 2013, de Godoy et al evaluated the efficacy of LLLT for treatment of TMD and reported that this modality decreased pain and inflammation and enhanced tissue repair. (16)
TENS is a non-pharmaceutical and non-invasive method of pain control; it reduces pain via both peripheral and central mechanisms. (17) In the central mechanism, TENS activates some opioid, serotonin and muscarinic receptors in the spinal cord and the brain stem. In the peripheral mechanism, opioid and alpha2 noradrenergic receptors at the site of TENS are stimulated and induce analgesia. (17) In 2005, Kato et al compared the efficacy of TENS and LLLT and found that both modalities were effective for treatment of TMD. (17)
Many studies have evaluated the efficacy of different modalities for treatment of MPS, reporting variable, and sometimes, controversial results. (1-3,15-23) Considering the existing controversy in the efficacy of MPS treatments, this study sought to assess the efficacy of TENS and LLL for treatment of MPS in comparison with a sham laser.
Materials and Methods
This randomized controlled clinical trial was conducted on MPS patients presenting to the Oral Medicine Department of Islamic Azad University, Dental Faculty, and to the TMJ Department of School of Dentistry of Tehran University of Medical Sciences.
The inclusion criteria were the age range of 18 to 60 years, diagnosis of MPS based on its signs and symptoms, signing the written informed consent form, having not more than three missing teeth in each jaw (not replaced), and no receipt of treatment for MPS in the past two weeks.
The exclusion criteria were pregnancy, psychological conditions, and depression for which patients took medications, (1,2,12,19) missing of more than three teeth in each jaw (not replaced), except for the third molars, ages below 18 and over 60 years, systemic diseases other than MPS, (24) contraindication for laser therapy or TENS, (2) contraindication for administration of methocarbamol or naproxen, (2) and history of receiving MPS treatment in the past two weeks. (1,12,19)
Based on previous studies and a pilot study (power of 80), the sample size was calculated to be 60 patients. Sampling was sequential randomized, and patients who met the inclusion criteria were randomly assigned to the test or control groups. Sampling was continued until the sample size was reached.
The study protocol was approved in the Committee of Medical Ethics of Islamic Azad University, Dental Faculty and registered in the Iranian Registry of Clinical Trials (Code: IRCT2014022116660N1r2). The study was thoroughly explained to patients and they all signed written informed consent forms.
Patients complaining of pain in the muscles of mastication and tenderness in at least one of the four major muscles of mastication (medial pterygoid, lateral pterygoid, anterior temporalis, and masseter) were diagnosed as having MPS. The pain in MPS often has a trigger point and is referral. These patients may suffer from impaired mastication or speech due to muscle contraction subsequent to pain. Other possible symptoms include mouth opening limitation, jaw deviation, articular sounds, neck pain, earache, and headache. (2) Clinical examination included the followings:
- Maximum active mouth opening (without the help of the dentist, with/without pain) was measured using a caliper. The distance between the incisal edges of the maxillary and mandibular incisors was measured. Normally, maximum mouth opening is 40 mm or more; smaller values indicate mouth opening limitation. Open bite or deep bite and the initial distance between the incisal edges of the upper and lower incisors must be taken into account as well when assessing mouth opening limitation. (2,24)
- Palpation of the muscles of mastication: The respective muscle was held by the index finger and the thumb, and approximately 2 pounds of pressure (1 kg equals approximately 2.2 pounds) was applied. Presence of pain and tenderness was assessed. The four major muscles of mastication (medial and lateral pterygoids, masseter, and temporalis) and the minor muscles (SCM and trapezius) were examined. The medial and lateral pterygoids were palpated intraorally with face in a relaxed position. The lateral pterygoid muscle was palpated by the small finger in the posterior maxillary vestibule along the molar teeth. The medial pterygoid muscle was palpated by the index finger in an open mouth at the internal border of the pterygomandibular raphe. (2)
- Pain of the TMJ when opening or closing the mouth actively by the patient was recorded using a VAS (visual analog scale). (1,12,19)
- Jaw deviation at maximum opening was measured by a caliper relative to the midline. (2) Deflection is defined as jaw deviation when opening the mouth; in this state, the midline in maximum opening does not correspond to its position in the closed mouth. Deviation is defined as jaw deviation in the path of mouth opening; however, in maximum opening, the midline corresponds to its position in the closed mouth. (19)
- Patients were asked about headache, earache or neck pain experience (related muscles); if the answer was positive, the patients were asked to express their level of pain using a VAS. (19)
After applying the inclusion and exclusion criteria, 55 subjects were enrolled; 18 subjects were assigned to group A and subjected to TENS and pharmaceutical therapy; 19 subjects were assigned to group B and received LLLT and pharmaceutical therapy, and 18 subjects were assigned to group C or the control group and underwent sham laser therapy and pharmaceutical therapy. Assignment of subjects to the groups was via block randomization; 20 blocks of three subjects each were used.
Subjects in all groups were evaluated in terms of demographic information (age and sex), history of MPS, the presence of parafunctional habits such as clenching and bruxism, and Angle’s class of malocclusion.
In group A (TENS and pharmaceutical therapy), patients (n=18) were subjected to TENS (Smart Series, Stimulator 710P, Novin Medical Engineering, Iran) in 10 sessions, each time for 20 minutes continuously with 100-μs pulse width and 10-Hz frequency in normal mode. (17,20)
In group B (LLLT and pharmaceutical therapy), patients (n=19) underwent LLLT with Gallium-Aluminum-Arsenide (GaAlAs) laser (Thor Co., London, UK) at 810-nm wavelength (808±5nm) and continuous-wave frequency three times a week for a total of 10 sessions. At each session, the laser was irradiated to the trigger points for 10 seconds. In case of absence of a specific trigger point, the laser was irradiated to several foci in the linear path of pain with the exposure settings of 200 mW/cm2 average power, 10s duration, 2 J/cm2 energy density, and 810-nm wavelength using a DD2 probe with an oval tip (1×1). (12) In terms of safety, this laser is classified as the 3B class with linear polarization (Thor Laser System, RN Medical, USA).
Eighteen controls received sham laser irradiation; however, patients were not aware whether they were receiving actual or sham laser irradiation. For the control group, the same laser handpiece was used but instead of the actual laser beam, only the guiding light was irradiated. A control group was included in this study to assess the psychological effect of treatment on the recovery of patients. (12)
All case and control groups received 500 mg of methocarbamol and 250 mg of naproxen t.i.d. for 10 days. (2,12)
To determine the level of pain of patients, a 10-point horizontal VAS was used before the treatment (baseline) and at one month after the treatment. Zero indicated no pain, while 10 indicated maximum pain. (2,12) The scores were recorded. The operator was blinded to the effects of treatment, and patients were also blinded to the phases of treatment. The person analyzing the results was also blinded to the effects of treatment.
In the examination of the major and minor muscles of mastication and the TMJ, right and left sides were separately examined. The side with higher VAS score was considered for data analysis. Kruskal-Wallis test was used to compare the three groups. In case of significant differences, pairwise comparisons were made by Dunn’s test.
Results
In this study, 55 patients with MPS were treated in three groups of TENS, LLLT, and sham laser. Patients were followed up after one month. At one month, 16 patients in TENS group, 18 patients in LLL group, and 15 patients in sham laser group showed up for the follow-up.
The VAS findings for tenderness of the muscles of mastication are as follows:
Table 1 shows the level of pain of the muscles of mastication in MPS patients at different time points. In the masseter muscle, the level of pain (VAS score) decreased in both TENS and LLLT groups after the treatment. The pain (VAS score) increased in sham laser group, and these changes in the three groups were statistically significant (P=0.001 for TENS, P=0.003 for LLLT, and P=0.028 for sham laser; Table 1). In the temporalis muscle, the level of pain decreased after treatment in TENS group but this reduction was not significant. In LLLT and sham laser groups, pain reduction was significant (P=0.843 for TENS, P=0.050 for LLLT, and P=0.001 for sham laser; Table 1). In the medial pterygoid muscle, pain severity decreased after treatment in TENS group but this reduction was not significant. Pain reduction in LLLT group was not significant either. Pain increased in sham laser group after treatment (P=0.160 for TENS, P=0.190 for LLLT, and P=0.001 for sham laser; Table 1). In the lateral pterygoid muscle, pain significantly decreased in TENS, LLLT, and sham laser groups (P=0.021 for TENS, P=0.006 for LLLT, and P=0.001 for sham laser; Table 1).
In the SCM muscle, pain significantly decreased in TENS group but this reduction was not significant in LLLT group. In sham laser group, tenderness significantly increased after treatment (P=0.049 for TENS, P=0.185 for LLLT, and P=0.001 for sham laser group; Table 1). In the trapezius muscle, pain significantly decreased in TENS and LLLT groups. In sham laser group, pain severity significantly increased (P=0.048 for TENS, P=0.027 for LLLT, and P=0.001 for sham laser; Table 1).
The amount of mouth opening in MPS patients at different time points is shown in Table 2. Mouth opening significantly increased in TENS group, while it significantly decreased in LLLT group after the treatment. The reduction in mouth opening was significant in sham laser group (P=0.051 for TENS, P=0.001 for LLLT, and P=0.001 for sham laser; Table 2).
Jaw deviation in MPS patients at different time points is presented in Table 3. Deflection and deviation were evaluated with respect to midline deviation when opening the mouth. Deflection increased in TENS and decreased in LLLT and sham laser groups; however, none of these changes were statistically significant (P=0.785 for TENS, P=0.063 for LLLT, and P=0.414 for sham laser; Table 3). Deviation increased in the three groups after the intervention but the increases were not statistically significant (P=0.180 for TENS, P=1 for LLLT, and P=1 for sham laser; Table 3).
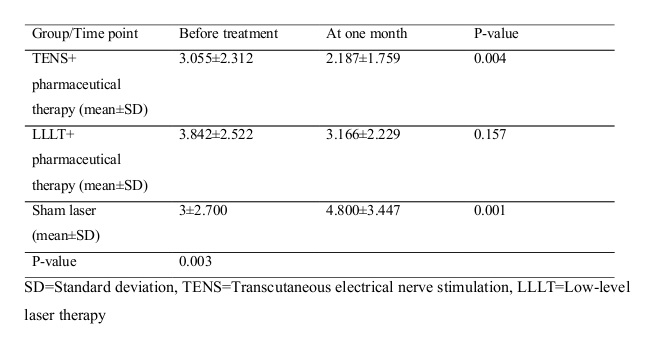
Table 4 presents the level of TMJ pain in MPS patients. Regarding TMJ pain when opening/closing the mouth, pain significantly decreased in TENS group but this reduction was not significant in LLLT group. In sham laser group, TMJ pain significantly increased; the difference of sham laser group with LLLT and TENS was statistically significant in this respect (P=0.004 for TENS, P=0.157 for LLL, and P=0.001 for sham laser; Table 4).
The level of neck pain, earache, and headache in MPS patients at different time points is presented in Table 5. With regard to pain in the minor muscles of mastication, neck pain significantly decreased in TENS and LLLT groups, while it significantly increased in sham laser group (P=0.015 for TENS, P=0.056 for LLLT, and P=0.001 for sham laser; Table 5). Earache significantly decreased in TENS group but the reduction in pain in LLLT group was not statistically significant. Pain significantly increased in sham laser group after the intervention (P=0.013 for TENS, P=0.159 for LLLT, and P=0.013 for sham laser; Table 5). Headache decreased in TENS and LLLT groups after the intervention but not significantly. Headache significantly increased in sham laser group after the intervention (P=0.302 for TENS, P=0.099 for LLLT, and P=0.001 for sham laser; Table 5).
Comparison of TENS and LLLT for pain in the masseter and medial pterygoid muscles revealed that TENS was more efficient than LLLT in significantly decreasing the pain. For pain in the lateral pterygoid muscle, LLLT was more efficient than TENS. No significant difference was noted between TENS and LLLT for the other muscles.
Table 1. Pain scores of the muscles of mastication in MPS patients in the three groups at different time points
Table 2. Amount of mouth opening (mm) in MPS patients in the three groups at different time points
Table 3. Jaw deviation (mm) in MPS patients in the three groups at different time points
Table 4. TMJ pain score in MPS patients in the three groups at different time points
Table 5. The severity (VAS score) of headache, neck pain, and earache in MPS patients in the three groups at different time points
Discussion
MPS is a chronic disease with a relatively high prevalence. It affects the quality of life and can impair daily activities. (2) It is responsible for many lost work days. Thus, it is important to find non-invasive methods for treatment of MPS. In this study, we assessed non-invasive treatment methods for MPS, namely electro-physiotherapy by TENS and LLLT, in comparison with a sham laser control group to find the most efficient technique. New treatment modalities can decrease the dose and duration of pharmaceutical therapy for pain control. Comparison of VAS scores in TENS and LLLT groups before and after the intervention revealed that both modalities could be used for treatment of myofascial pain. The relationship of TMD with psychological disorders has been confirmed. Since it is believed that laser has psychological effects in addition to its somatic effects, we included a sham laser control group in our study; but apparently, this psychological effect cannot treat MPS alone, and the somatic effect of laser is dominant.
In 2013, de Godoy et al used a laser in the case group and had a placebo control group; their results were in accordance with our findings in the LLLT group. In our study, the laser was extra-orally irradiated on the painful muscles. Their results showed that laser decreased muscle pain and enhanced the quality of life of patients. (16) However, they only evaluated temporalis and masseter muscles, while we compared the level of pain and tenderness of the four muscles of mastication and the neck muscles.
In 2010, Mortazavi et al evaluated the factors related to MPS and found results similar to ours. Moreover, in their study, the number of females was higher than males, which was the same as in our study. This dominance may be due to the fact that female patients are more likely to seek treatment and show up for the follow-ups. (19) In 2005, Kato et al assessed tenderness of temporalis and masseter muscles but they did not examine medial and lateral pterygoids. (17) The level of pain was not significantly different between the two groups of TENS and LLLT but pain in each group significantly decreased after the intervention. Their results regarding the masseter muscle were similar to ours. However, no significant change occurred in the level of pain of the temporalis muscle in TENS group, and we only noted a significant reduction in pain in LLLT group. This difference may be due to the methodology of the two studies and to the method of using the tools at the trigger points; for instance, in TENS group, we used the handpiece extra-orally at the site of the muscle with maximum pain (which was mainly the masseter muscle). (8) Kato et al did not assess the psychological effect of laser but we had a sham laser group despite the self-limiting nature of muscle problems in TMD and thus, we can state with more certainty that both TENS and LLLT were efficient for pain relief, and partial recovery of patients cannot be exclusively attributed to time lapse because the results in the control group were not satisfactory.
In 2013, Amanat et al evaluated the efficacy of laser therapy along with pharmaceutical therapy for treatment of MPD. (12) In their study, GaAs laser at 980-nm wavelength was used, while we used GaAlAs laser at 810-nm wavelength; this may explain some differences in the results of the two studies. In contrast to our study, Amanat et al did not find a significant difference in pain intensity between the case and control groups. (12) In our study, significant pain reduction after treatment only occurred in the lateral pterygoid and temporalis muscles of the sham group while pain increased in their medial pterygoid and masseter muscles; therefore, the psychological effect of laser on muscle pain reduction was not confirmed in our study.
The mechanism of the analgesic (somatic) effect of the laser can partly be related to the release of endogenous endorphins, which has been confirmed in vitro. (25) This effect of laser depends on its intensity and specific wavelength. On the other hand, laser has an anti-inflammatory effect and not only increases the activity of macrophages and neutrophils but also enhances the secretion of specific inflammatory mediators. (10,26,27)
In 2007, Azizi et al evaluated the efficacy of laser for treatment of MPS and found a significant reduction in pain in the masseter, lateral pterygoid, and temporalis muscles, (1) which is similar to our findings; for the medial pterygoid, we found no significant change in LLLT group. In our study, the laser was used extra-orally on the skin; some previous studies have reported laser penetration depth of 2 to 5 cm in this position. (21,28,29) Thus, it is logical to assume that lower effect of LLLT on the medial pterygoid muscle in our study may be due to the deeper position of this muscle (in comparison with other muscles) and the consequently lower dose of laser absorbed by this muscle. Azizi et al only evaluated the somatic effect of the laser and had no control group to assess its psychological effect; (1) this was a limitation of their study.
In the current study, we evaluated the therapeutic effect of TENS on MPS. Evidence shows that TENS has both local and central analgesic effects. (20,22) Some studies have concluded that if a muscle is painful, treatment of its counterpart with TENS would decrease the intensity of pain in the primarily painful muscle. (20,22) As described earlier, TENS decreases pain via both peripheral and central mechanisms. Chronic muscle pain may be the result of the production and progressive accumulation of metabolic oxidation products in the muscle, stimulating the peripheral pain receptors. (24) Thus, pain control tools should act both centrally and peripherally. Both TENS and LLLT are capable of inhibiting pain via central and peripheral mechanisms. Thus, further studies on their pain control mechanisms can result in their more extensive and targeted use for pain relief.
Conclusion
Application of LLL can be successful for treatment of MPS. TENS is also an efficient modality for treatment of these patients.
Subjects in all groups were evaluated in terms of demographic information (age and sex), history of MPS, the presence of parafunctional habits such as clenching and bruxism, and Angle’s class of malocclusion.
In group A (TENS and pharmaceutical therapy), patients (n=18) were subjected to TENS (Smart Series, Stimulator 710P, Novin Medical Engineering, Iran) in 10 sessions, each time for 20 minutes continuously with 100-μs pulse width and 10-Hz frequency in normal mode. (17,20)
In group B (LLLT and pharmaceutical therapy), patients (n=19) underwent LLLT with Gallium-Aluminum-Arsenide (GaAlAs) laser (Thor Co., London, UK) at 810-nm wavelength (808±5nm) and continuous-wave frequency three times a week for a total of 10 sessions. At each session, the laser was irradiated to the trigger points for 10 seconds. In case of absence of a specific trigger point, the laser was irradiated to several foci in the linear path of pain with the exposure settings of 200 mW/cm2 average power, 10s duration, 2 J/cm2 energy density, and 810-nm wavelength using a DD2 probe with an oval tip (1×1). (12) In terms of safety, this laser is classified as the 3B class with linear polarization (Thor Laser System, RN Medical, USA).
Eighteen controls received sham laser irradiation; however, patients were not aware whether they were receiving actual or sham laser irradiation. For the control group, the same laser handpiece was used but instead of the actual laser beam, only the guiding light was irradiated. A control group was included in this study to assess the psychological effect of treatment on the recovery of patients. (12)
All case and control groups received 500 mg of methocarbamol and 250 mg of naproxen t.i.d. for 10 days. (2,12)
To determine the level of pain of patients, a 10-point horizontal VAS was used before the treatment (baseline) and at one month after the treatment. Zero indicated no pain, while 10 indicated maximum pain. (2,12) The scores were recorded. The operator was blinded to the effects of treatment, and patients were also blinded to the phases of treatment. The person analyzing the results was also blinded to the effects of treatment.
In the examination of the major and minor muscles of mastication and the TMJ, right and left sides were separately examined. The side with higher VAS score was considered for data analysis. Kruskal-Wallis test was used to compare the three groups. In case of significant differences, pairwise comparisons were made by Dunn’s test.
Results
In this study, 55 patients with MPS were treated in three groups of TENS, LLLT, and sham laser. Patients were followed up after one month. At one month, 16 patients in TENS group, 18 patients in LLL group, and 15 patients in sham laser group showed up for the follow-up.
The VAS findings for tenderness of the muscles of mastication are as follows:
Table 1 shows the level of pain of the muscles of mastication in MPS patients at different time points. In the masseter muscle, the level of pain (VAS score) decreased in both TENS and LLLT groups after the treatment. The pain (VAS score) increased in sham laser group, and these changes in the three groups were statistically significant (P=0.001 for TENS, P=0.003 for LLLT, and P=0.028 for sham laser; Table 1). In the temporalis muscle, the level of pain decreased after treatment in TENS group but this reduction was not significant. In LLLT and sham laser groups, pain reduction was significant (P=0.843 for TENS, P=0.050 for LLLT, and P=0.001 for sham laser; Table 1). In the medial pterygoid muscle, pain severity decreased after treatment in TENS group but this reduction was not significant. Pain reduction in LLLT group was not significant either. Pain increased in sham laser group after treatment (P=0.160 for TENS, P=0.190 for LLLT, and P=0.001 for sham laser; Table 1). In the lateral pterygoid muscle, pain significantly decreased in TENS, LLLT, and sham laser groups (P=0.021 for TENS, P=0.006 for LLLT, and P=0.001 for sham laser; Table 1).
In the SCM muscle, pain significantly decreased in TENS group but this reduction was not significant in LLLT group. In sham laser group, tenderness significantly increased after treatment (P=0.049 for TENS, P=0.185 for LLLT, and P=0.001 for sham laser group; Table 1). In the trapezius muscle, pain significantly decreased in TENS and LLLT groups. In sham laser group, pain severity significantly increased (P=0.048 for TENS, P=0.027 for LLLT, and P=0.001 for sham laser; Table 1).
The amount of mouth opening in MPS patients at different time points is shown in Table 2. Mouth opening significantly increased in TENS group, while it significantly decreased in LLLT group after the treatment. The reduction in mouth opening was significant in sham laser group (P=0.051 for TENS, P=0.001 for LLLT, and P=0.001 for sham laser; Table 2).
Jaw deviation in MPS patients at different time points is presented in Table 3. Deflection and deviation were evaluated with respect to midline deviation when opening the mouth. Deflection increased in TENS and decreased in LLLT and sham laser groups; however, none of these changes were statistically significant (P=0.785 for TENS, P=0.063 for LLLT, and P=0.414 for sham laser; Table 3). Deviation increased in the three groups after the intervention but the increases were not statistically significant (P=0.180 for TENS, P=1 for LLLT, and P=1 for sham laser; Table 3).
Table 4 presents the level of TMJ pain in MPS patients. Regarding TMJ pain when opening/closing the mouth, pain significantly decreased in TENS group but this reduction was not significant in LLLT group. In sham laser group, TMJ pain significantly increased; the difference of sham laser group with LLLT and TENS was statistically significant in this respect (P=0.004 for TENS, P=0.157 for LLL, and P=0.001 for sham laser; Table 4).
The level of neck pain, earache, and headache in MPS patients at different time points is presented in Table 5. With regard to pain in the minor muscles of mastication, neck pain significantly decreased in TENS and LLLT groups, while it significantly increased in sham laser group (P=0.015 for TENS, P=0.056 for LLLT, and P=0.001 for sham laser; Table 5). Earache significantly decreased in TENS group but the reduction in pain in LLLT group was not statistically significant. Pain significantly increased in sham laser group after the intervention (P=0.013 for TENS, P=0.159 for LLLT, and P=0.013 for sham laser; Table 5). Headache decreased in TENS and LLLT groups after the intervention but not significantly. Headache significantly increased in sham laser group after the intervention (P=0.302 for TENS, P=0.099 for LLLT, and P=0.001 for sham laser; Table 5).
Comparison of TENS and LLLT for pain in the masseter and medial pterygoid muscles revealed that TENS was more efficient than LLLT in significantly decreasing the pain. For pain in the lateral pterygoid muscle, LLLT was more efficient than TENS. No significant difference was noted between TENS and LLLT for the other muscles.
Table 1. Pain scores of the muscles of mastication in MPS patients in the three groups at different time points
{kind=link}
Table 2. Amount of mouth opening (mm) in MPS patients in the three groups at different time points
{kind=link}
Table 3. Jaw deviation (mm) in MPS patients in the three groups at different time points
{kind=link}
Table 4. TMJ pain score in MPS patients in the three groups at different time points
{kind=link}
Table 5. The severity (VAS score) of headache, neck pain, and earache in MPS patients in the three groups at different time points
{kind=link}
Discussion
MPS is a chronic disease with a relatively high prevalence. It affects the quality of life and can impair daily activities. (2) It is responsible for many lost work days. Thus, it is important to find non-invasive methods for treatment of MPS. In this study, we assessed non-invasive treatment methods for MPS, namely electro-physiotherapy by TENS and LLLT, in comparison with a sham laser control group to find the most efficient technique. New treatment modalities can decrease the dose and duration of pharmaceutical therapy for pain control. Comparison of VAS scores in TENS and LLLT groups before and after the intervention revealed that both modalities could be used for treatment of myofascial pain. The relationship of TMD with psychological disorders has been confirmed. Since it is believed that laser has psychological effects in addition to its somatic effects, we included a sham laser control group in our study; but apparently, this psychological effect cannot treat MPS alone, and the somatic effect of laser is dominant.
In 2013, de Godoy et al used a laser in the case group and had a placebo control group; their results were in accordance with our findings in the LLLT group. In our study, the laser was extra-orally irradiated on the painful muscles. Their results showed that laser decreased muscle pain and enhanced the quality of life of patients. (16) However, they only evaluated temporalis and masseter muscles, while we compared the level of pain and tenderness of the four muscles of mastication and the neck muscles.
In 2010, Mortazavi et al evaluated the factors related to MPS and found results similar to ours. Moreover, in their study, the number of females was higher than males, which was the same as in our study. This dominance may be due to the fact that female patients are more likely to seek treatment and show up for the follow-ups. (19) In 2005, Kato et al assessed tenderness of temporalis and masseter muscles but they did not examine medial and lateral pterygoids. (17) The level of pain was not significantly different between the two groups of TENS and LLLT but pain in each group significantly decreased after the intervention. Their results regarding the masseter muscle were similar to ours. However, no significant change occurred in the level of pain of the temporalis muscle in TENS group, and we only noted a significant reduction in pain in LLLT group. This difference may be due to the methodology of the two studies and to the method of using the tools at the trigger points; for instance, in TENS group, we used the handpiece extra-orally at the site of the muscle with maximum pain (which was mainly the masseter muscle). (8) Kato et al did not assess the psychological effect of laser but we had a sham laser group despite the self-limiting nature of muscle problems in TMD and thus, we can state with more certainty that both TENS and LLLT were efficient for pain relief, and partial recovery of patients cannot be exclusively attributed to time lapse because the results in the control group were not satisfactory.
In 2013, Amanat et al evaluated the efficacy of laser therapy along with pharmaceutical therapy for treatment of MPD. (12) In their study, GaAs laser at 980-nm wavelength was used, while we used GaAlAs laser at 810-nm wavelength; this may explain some differences in the results of the two studies. In contrast to our study, Amanat et al did not find a significant difference in pain intensity between the case and control groups. (12) In our study, significant pain reduction after treatment only occurred in the lateral pterygoid and temporalis muscles of the sham group while pain increased in their medial pterygoid and masseter muscles; therefore, the psychological effect of laser on muscle pain reduction was not confirmed in our study.
The mechanism of the analgesic (somatic) effect of the laser can partly be related to the release of endogenous endorphins, which has been confirmed in vitro. (25) This effect of laser depends on its intensity and specific wavelength. On the other hand, laser has an anti-inflammatory effect and not only increases the activity of macrophages and neutrophils but also enhances the secretion of specific inflammatory mediators. (10,26,27)
In 2007, Azizi et al evaluated the efficacy of laser for treatment of MPS and found a significant reduction in pain in the masseter, lateral pterygoid, and temporalis muscles, (1) which is similar to our findings; for the medial pterygoid, we found no significant change in LLLT group. In our study, the laser was used extra-orally on the skin; some previous studies have reported laser penetration depth of 2 to 5 cm in this position. (21,28,29) Thus, it is logical to assume that lower effect of LLLT on the medial pterygoid muscle in our study may be due to the deeper position of this muscle (in comparison with other muscles) and the consequently lower dose of laser absorbed by this muscle. Azizi et al only evaluated the somatic effect of the laser and had no control group to assess its psychological effect; (1) this was a limitation of their study.
In the current study, we evaluated the therapeutic effect of TENS on MPS. Evidence shows that TENS has both local and central analgesic effects. (20,22) Some studies have concluded that if a muscle is painful, treatment of its counterpart with TENS would decrease the intensity of pain in the primarily painful muscle. (20,22) As described earlier, TENS decreases pain via both peripheral and central mechanisms. Chronic muscle pain may be the result of the production and progressive accumulation of metabolic oxidation products in the muscle, stimulating the peripheral pain receptors. (24) Thus, pain control tools should act both centrally and peripherally. Both TENS and LLLT are capable of inhibiting pain via central and peripheral mechanisms. Thus, further studies on their pain control mechanisms can result in their more extensive and targeted use for pain relief.
Conclusion
Application of LLL can be successful for treatment of MPS. TENS is also an efficient modality for treatment of these patients.
Type of Study: Original article |
Subject:
Oral & maxillofacial surgery
References
1. 1. Azizi A, Sahebjamee M, Lawaf SH, Jamalee F, Maroofi N. Effects of Low-level Laser in the Treatment of Myofascial Pain Dysfunction Syndrome. J Dent Res Dent Clin Dent Prospects. 2007 Summer;1(2):53-8.
2. Gil-Martínez A, Paris-Alemany A, López-deUralde-Villanueva I, Touche R L. Management of pain in patients with temporomandibular disorder (TMD): challenges and solutions J Pain Res. 2018; 11: 571-7. [DOI:10.2147/JPR.S127950] [PMID] [PMCID]
3. Fricton JR, Kroening R, Haley D, Siegert R. Myofascial pain syndrome of the head and neck: a review of clinical characteristics of 164 patients. Oral Surg Oral Med Oral Pathol. 1985 Dec;60(6):615-23. [DOI:10.1016/0030-4220(85)90364-0]
4. Pokorny PH, Wiens JP, Litvak H. Occlusion for fixed prosthodontics: a historical perspective of the gnathological influence. J Prosthet Dent. 2008 Apr;99(4):299-313. [DOI:10.1016/S0022-3913(08)60066-9]
5. Bennett R. Myofascial pain syndromes and their evaluation. Best Pract Res Clin Rheumatol. 2007 Jun;21(3):427-45. [DOI:10.1016/j.berh.2007.02.014] [PMID]
6. Silveira PC, Streck EL, Pinho RA. Evaluation of mitochondrial respiratory chain activity in wound healing by low-level laser therapy. J Photochem Photobiol B. 2007 Mar 1;86(3):279-82. [DOI:10.1016/j.jphotobiol.2006.10.002] [PMID]
7. Basso FG, Oliveira CF, Kurachi C, Hebling J, Costa CA. Biostimulatory effect of low-level laser therapy on keratinocytes in vitro. Lasers Med Sci. 2013 Feb;28(2):367-74. [DOI:10.1007/s10103-012-1057-8] [PMID]
8. Akgul T, Gulsoy M, Gulcur HO. Effects of early and delayed laser application on nerve regeneration. Lasers Med Sci. 2014 Jan;29(1):351-7. [DOI:10.1007/s10103-013-1355-9] [PMID]
9. Cury V, Moretti AI, Assis L, Bossini P, Crusca Jde S, Neto CB, et al. Low level laser therapy increases angiogenesis in a model of ischemic skin flap in rats mediated by VEGF, HIF-1α and MMP-2. J Photochem Photobiol B. 2013 Aug 5;125:164-70. [DOI:10.1016/j.jphotobiol.2013.06.004] [PMID] [PMCID]
10. Fukuda TY, Tanji MM, Silva SR, Sato MN, Plapler H. Infrared low-level diode laser on inflammatory process modulation in mice: pro- and anti-inflammatory cytokines. Lasers Med Sci. 2013 Sep;28(5):1305-13. [DOI:10.1007/s10103-012-1231-z] [PMID]
11. Gorshkova OP, Shuvaeva VN, Dvoretsky DP. Role of nitric oxide in responses of pial arterial vessels to low-intensity red laser irradiation. Bull Exp Biol Med. 2013 Sep;155(5):598-600. [DOI:10.1007/s10517-013-2203-4] [PMID]
12. Amanat D, Ebrahimi H, Lavaee F, Alipour A. The adjunct therapeutic effect of lasers with medication in the management of orofacial pain: double blind randomized controlled trial. Photomed Laser Surg. 2013 Oct;31(10):474-9. [DOI:10.1089/pho.2013.3555] [PMID]
13. Heu F, Forster C, Namer B, Dragu A, Lang W. Effect of low-level laser therapy on blood flow and oxygen- hemoglobin saturation of the foot skin in healthy subjects: a pilot study. Laser Ther. 2013;22(1):21-30. [DOI:10.5978/islsm.13-OR-03] [PMID] [PMCID]
14. Hudson DE, Hudson DO, Wininger JM, Richardson BD. Penetration of laser light at 808 and 980 nm in bovine tissue samples. Photomed Laser Surg. 2013 Apr;31(4):163-8. [DOI:10.1089/pho.2012.3284] [PMID] [PMCID]
15. Chang WD, Lee CL, Lin HY, Hsu YC, Wang CJ, Lai PT. A Meta-analysis of Clinical Effects of Low-level Laser Therapy on Temporomandibular Joint Pain. J Phys Ther Sci. 2014 Aug;26(8):1297- 300. [DOI:10.1589/jpts.26.1297] [PMID] [PMCID]
16. de Godoy CH, Silva PF, de Araujo DS, Motta LJ, Biasotto-Gonzalez DA, Politti F, et al. Evaluation of effect of low-level laser therapy on adolescents with temporomandibular disorder: study protocol for a randomized controlled trial. Trials. 2013 Jul 22;14:229. [DOI:10.1186/1745-6215-14-229] [PMID] [PMCID]
17. Kato MT, Kogawa EM, Santos CN, Conti PC. TENS and low-level laser therapy in the management of temporomandibular disorders. J Appl Oral Sci. 2006 Apr;14(2):130-5. [DOI:10.1590/S1678-77572006000200012] [PMID] [PMCID]
18. Huang YY, Chen AC, Carroll JD, Hamblin MR. Biphasic dose response in low level light therapy. Dose Response. 2009 Sep 1;7(4):358-83. [DOI:10.2203/dose-response.09-027.Hamblin] [PMID] [PMCID]
19. Mortazavi H, Javadzadeh A, Delavarian Z, Mahmoodabadi R. Myofascial pain dysfunction syndrome. IJOL. 2010 Autumn;22(61):131-6.
20. De Santana JM, Walsh DM, Vance C, Rakel BA, Sluka KA. Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain. Curr Rheumatol Rep. 2008 Dec;10(6):492-9. [DOI:10.1007/s11926-008-0080-z] [PMID] [PMCID]
21. Di Giacomo P, Orlando S, Dell' Ariccia M, Brandimarte B. Low level laser therapy: Laser radiation absorption in biological tissues. Appl Phys A. 2013;112:71-5. [DOI:10.1007/s00339-012-7204-z]
22. Bennett MI, Hughes N, Johnson MI. Methodological quality in randomised controlled trials of transcutaneous electric nerve stimulation for pain: low fidelity may explain negative findings. Pain. 2011 Jun;152(6):1226-32. [DOI:10.1016/j.pain.2010.12.009] [PMID]
23. Hakgüder A, Birtane M, Gürcan S, Kokino S, Turan FN. Efficacy of low level laser thera- py in myofascial pain syndrome: an algometric and thermographic evaluation. Lasers Surg Med. 2003;33(5):339-43. [DOI:10.1002/lsm.10241] [PMID]
24. Lawaf SH, Azizi A, Tabarestani T. Comparison of serum and salivary antioxidants in patients with temporomandibular joint disorders and healthy subjects. J Dent (Tehran). 2015 Apr;12(4):263-70.
25. Hagiwara S, Iwasaka H, Okuda K, Noguchi T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid analgesia in rats. Lasers Surg Med. 2007 Dec;39(10):797-802. [DOI:10.1002/lsm.20583] [PMID]
26. Mafra de Lima F, Villaverde AB, Salgado MA, Castro-Faria-Neto HC, Munin E, Albertini R, et al. Low intensity laser therapy (LILT) in vivo acts on the neutrophils recruitment and chemokines/ cytokines levels in a model of acute pulmonary inflammation induced by aerosol of lipopolysaccharide from Escherichia coli in rat. J Photochem Photobiol B. 2010 Dec 2;101(3):271-8. [DOI:10.1016/j.jphotobiol.2010.07.012] [PMID]
27. Ma WJ, Li XR, Li YX, Xue ZX, Yin HJ, Ma H. Antiinflammatory effect of low-level laser therapy on Staphylococcus epidermidis endophthalmitis in rabbits. Lasers Med Sci. 2012 May;27(3):585-91. [DOI:10.1007/s10103-011-0991-1] [PMID]
28. Joensen J, Ovsthus K, Reed RK, Hummelsund S, Iversen VV, Lopes-Martins RÁ, et al. Skin penetration time-profiles for continuous 810 nm and Superpulsed 904 nm lasers in a rat model. Photomed Laser Surg. 2012 Dec;30(12):688-94. [DOI:10.1089/pho.2012.3306] [PMID]
29. Hudson DE, Hudson DO, Wininger JM, Richardson BD. Penetration of laser light at 808 and 980 nm in bovine tissue samples. Photomed Laser Surg. 2013 Apr;31(4):163-8. [DOI:10.1089/pho.2012.3284] [PMID] [PMCID]
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
