



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-198-en.html


2- Dentist
3- Post Graduate Student, Oral and Maxillofacial Department, Dental Branch of Tehran, , kmesgari@gmail.com
Abstract
Background and aim: Neurosensory disorders after implant insertion are one of the main concerns in implant treatments. Neurosensory disorders can be driven by different factors including the contact of the implant with the nerve, pressure of edema, hematoma, scar, or dental injections. This study aimed at investigating the distance between the implant and the inferior alveolar nerve (IAN) and its impact on neurosensory disorders.
Materials and methods: In this descriptive study, panoramic radiographs were taken from 100 patients experiencing neurosensory changes after 10 days of implantation. The patients were reassessed 4 weeks later, and the distance (mm) between the implants and the IAN was measured. Data were analyzed using descriptive statistics.
Results: All patients experienced neurosensory changes 10 days after implantation. Four weeks after surgery, 82 patients healed: the distance between the implants and the IAN was 1-2 mm in 16 patients and 2 mm in 66 patients. In 18 patients, neurosensory changes persisted; in this group, the distance between the implants and the IAN was less than 1 mm in 11 patients, 1-2 mm in 6 patients, and more than 2 mm in 1 patient. The results indicated that the chance of healing of neurosensory changes is significantly correlated with the distance between the implant and the IAN (P<0.01). This correlation was not significant with respect to age or gender (P<0.9).
Conclusion: It seems that the lesser is the distance between the implant and the IAN, the lower is the chance of healing of neurosensory changes.
Key words: Dental Implant, Inferior Alveolar Nerve, Paresthesia, Nerve Injuries, Sensation Disorder
Introduction
One of the main concerns in implant surgery is neural changes following implantation. (1,2) Some studies have reported neurosensory changes in the lower lip after implantation in 8.5%, 11%, and 24% of patients. In other studies, symptoms of neurosensory changes appeared one year following implantation in 1% of the patients, while in another investigation, 16 months after implant surgery, 7% of the patients suffered from neurosensory changes; however, there were no persistent neurosensory changes 4 months after implantation. (3-5) Neural disturbance can be caused by different factors, including the pressure exerted by a full denture or a partial denture on the mental nerve (MN), the contact of the implant with the nerve, the pressure caused by edema, hematoma, scar, or dental injections. (6-8) The consequences of this damage include paresthesia, hypoesthesia, hyperesthesia, dysesthesia, and anesthesia of the teeth, lower lip, skin, or mucosa. (8) This damage may cause arterial or venous bleeding, whereas peri-implantitis can induce paresthesia. (9,10)
In some studies, a distance of 2 mm from the inferior alveolar nerve (IAN) has been recommended for implant insertion. (11,12). Also, the use of an appropriate treatment plan has been recommended to reduce neurosensory changes after implantation. (13) Different studies have assessed the risk of damages to the IAN after implant placement in the mandibular bone (1-3,10,13). However, limited information is available regarding the correlation between the implant-IAN distance and neurosensory changes.
Considering the importance of implant treatments and the consequences of an improper implant-IAN distance and its relationship with neural damages caused by an improper implant position, research in this field is considered the main priority in dental studies. In addition, according to the current studies on implant surgery methods, data collection was simple. Therefore, considering that few studies are available regarding the distance between the IAN and the implant, in this research, this distance and its relationship with neurosensory changes were studied on the patients presenting to Bu-Ali hospital and the dental branch of Islamic Azad University of Tehran in 2015.
Materials and Methods
In this descriptive study, the dependent variables were neurosensory changes of the lower lip and the surrounding skin and mucosa, including paresthesia, hypoesthesia, hyperesthesia, dysesthesia, and anesthesia. The measurement scale of these indices is qualitative-nominal, and they were measured through interviewing the patients. The independent variable was the distance (mm) between the implant and the IAN, and its measurement scale is quantitative-interval. The intervening variables were the age and gender.
The statistical population included all patients with neurosensory changes after implantation at Bu-Ali Hospital, Tehran, Iran and at the dental branch of Islamic Azad University of Tehran in 2015. One-hundred patients were selected randomly.
The information form consisted of two sections: a section about neurosensory changes after surgery, and a section about the distance from the implant apex to the IAN supplemented with other patient information. It should be noted that any direct canal invasion was excluded.
The patients (n=100) included 43 women and 57 men, averagely 53 years old, who experienced neurosensory changes 10 days after implantation, and panoramic radiographs (CRANEX® D Panoramic Dental X-Ray Machine, Soredex, Orion Co. Ltd., Helsinki, Finland) were taken as soon as they reported the neural changes. (14-16) The purpose of the study was explained to the patients, and written informed consent forms were received.
The patients were asked to sit on the dental unit and to close their eyes. Both sides of the lip were examined using a swap and a catheter tip in order to compare senses. Then, areas with sensory changes such as paresthesia, dysesthesia, or anesthesia, were determined for each patient (mapping). Paresthesia is an unusual sensation such as tingling, prickling, numbness, or burning of the skin with no obvious physical cause. (17) Dysesthesia is defined as an unpleasant or unusual sense of touch, which may present as pain or as an inappropriate sensation; it is caused by lesions of the peripheral or central nervous system, and it comprises impulsive or induced sensations of burning, wetness, itching, and electric shock. (18) Dysesthesia can comprise sensations in any tissue including the mouth, scalp, skin, or legs. (18) Anesthesia is "a state of temporary induced loss of sensation". (19) Four weeks after the operation, panoramic radiography was retaken (with the same radiography machine and in the same manner), and the patients were studied and examined again. (16) Next, the distances between the implants and the IAN were measured on the panoramic radiographs using the measuring tool provided by the manufacturer (Soredex). The collected data were analyzed using descriptive statistics.
Results
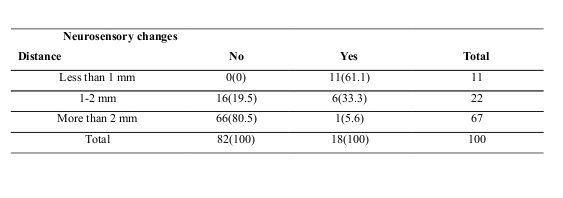
In this study, 100 patients (43 women and 57 men), averagely 53 years old, who experienced neurosensory changes 10 days after implantation were examined. After 4 weeks, the patients were distributed according to neurosensory changes (Table 1). The sensory changes in 82% of the patients healed; the distance between the implant and the IAN was 1-2 mm in 16 patients and more than 2 mm in 66 patients. In the other 18 patients with persistent neural changes, the distance between the implant and the IAN was less than 1 mm in 11 patients, 1-2 mm in 6 patients, and more than 2 mm in 1 patient. In addition, 61 patients suffered from hypoesthesia, 22 patients had paresthesia, 13 patients had anesthesia, and 4 patients had dysesthesia. The results indicated that the healing of neurosensory changes is significantly correlated with the distance between the implant and the IAN (P<0.01).
The distribution of the patients according to neurosensory changes and categorized by age and gender is presented in Table 2.
Table 1: Patients’ distribution according to neurosensory changes and the distance between the implant and the inferior alveolar nerve (IAN)
Table 2: Patients’ distribution according to neurosensory changes categorized by age and gender
Discussion
{kind=link}
{kind=link}
The present research indicates that there is a close relationship between the implant-IAN distance and neurosensory changes such that if the distance becomes shorter, the chances of the recovery of neural changes would get lower; these changes have no correlation with age or gender.
Implant treatment planning needs to be accurate in order to achieve predictable results. Radiography is carried out for evaluating the quantity and morphology of the remaining peri-implant alveolar bone and its surrounding anatomical structures, especially the position of the IAN and the maxillary sinus (14,15).
Some studies have assessed the IAN damage after placing an implant in the mandibular bone (16-26). Lin et al studied the IAN damage during immediate implantation. (1) They did not assess other implant placement techniques, or a safe distance for preventing sensory disorders caused by nerve damage, or the relationship between neurosensory changes and age or gender. In the present study, no significant relationship was found between neurosensory changes and age or gender. Also, Their results indicated that, compared to other dental areas, placing an implant in the mandibular second molar area has a higher risk of damaging the IAN, and this risk is 3.82 times more than the risk of implant placement in the mandibular second premolar area. (1) In addition, their results revealed that IAN damage is 26% reduced per 1 mm increase in the distance from the tooth apex to the IAN (1).
Kim et al studied neurosensory changes caused by peri-implantitis; (10) however, they did not study the distance between the implant and the IAN. Nevertheless, they concluded that placing an implant in the mandibular molar-premolar area or close to the IAN or the MN causes inflammation and paresthesia (10).
Juodzbalys et al systematically studied the diagnostic methods and harmful factors for the IAN and identified the time interval between nerve damage and its diagnosis after implant placement. (27) Shavit et al studied sensory changes of the MN after implant insertion. (28) Their results illustrated that few patients suffer from sensory changes after placing an implant in the mandibular bone. In contrast to other studies, no persistent neurosensory changes were encountered. In addition, they recommended using a correct treatment plan for reducing the chance of sensory changes after placing dental implants. However, they did not study sensory changes after other implant treatments in which the implant is not placed immediately (28).
We measured the distance between the implant and the IAN and assessed its correlation with neurosensory disorders and found a significant correlation between this distance and neurosensory disturbances.
Conclusion
Based on the results of the present study, it seems that the lesser is the distance between the implant and the IAN, the lower is the chance of healing of neurosensory changes, and these changes have no correlation with age or gender.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
