



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://jrdms.dentaliau.ac.ir/article-1-106-en.html


2- Assistant Professor, Removable Prosthodontics Dept,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran.
3- Assistant Professor, Dental biomaterial Dept,Dental School,Shahid BeheshtiUniversity of Medical sciences, Tehran ,Iran.
4- Dental Student,Dental Branch of Tehran, Islamic Azad University, Tehran, Iran.
Abstract
Background and Aim: Resin cements are used widely in restorative dentistry regardless of their biocompatibility. The aim of this study was to compare the cytotoxicity of two categories of dental cements consisting of three chemically set cements (Fuji I, Fuji PLUS and Harvard) and two dual curing cements (BisCem and Duo-Link) by use of MTT assay.
Materials and Methods: In this experimental study, four round-shaped samples of each specimen were placed in DMEM culture medium for 24, 48 and 72 hours. The extracts from each sample were applied on L929 mouse fibroblasts. At the end of each period, MTT assay was carried out to estimate the mitochondrial respiration. Data were analyzed by one-way analysis of variance (ANOVA) followed by Tukey's post-hoc test. The degree of cytotoxicity for each sample was determined according to the reference value of the control group.
Results: Fuji I cement showed the least cytotoxicity while Harvard and BisCem cements showed the highest cytotoxic effect. The differences were not significant compared to the positive control (distilled water).
Conclusion: This study showed that dental cements are capable of eliciting biological response in gingival and pulpal cells. They present a potential risk of tissue damage which depends on the cement's brand and curing modes.
Keywords: cytotoxicity test; dental cements; biocompatibility; fibroblasts.
Introduction
The biocompatibility of dental materials is a field of increasing interest among dental professionals and patients.1 The study of dental materials has received great attention, since the toxic compounds released from these materials may interfere with healing processes or cause allergic reactions which would lead to tissue damage.2 In fixed prosthodontics, dental cements are used to enhance tooth-restoration adhesion. For over a century, Zinc Phosphate Cement has been the most successful cementing medium in dental practice.3-6 However, the mentioned cement shows polymerization shrinkage, solubility, low pH and inability to chemically bond with the tooth. Therefore, Glass Ionomer Cements (GIC) have been introduced to dentistry. These bioactive materials were first introduced in the early 70s by Wilson and Kent (1972) however their chemical composition has majorly changed since then.7 Conventional GICs present several beneficial properties such as biocompatibility, fluoride release, and coefficient of thermal expansion and modulus of elasticity similar to dentin. Despite their advantages, conventional GICs have limitations related to their susceptibility to dehydration and poor physical properties such as high solubility and a slow setting rate. Further developments in the field of GICs have led to the introduction of Resin Modified Glass Ionomer Cements (RM-GICs) with improved physical and mechanical properties compared with conventional GICs. 8 Recently, resin cements have been introduced to dentistry. They contain a major composite resin portion which chemically bonds with the tooth.9 Since these cements are reported to enhance retention of the restorations, they have been utilized increasingly by dentists regardless of their biocompatibility. However, cytotoxicity of these materials remains a concern due to the presence of TEGDMA or hydroxyethyl methacrylate (HEMA) that penetrate into the dentinal tubules and cause an inflammatory response in the pulp.
Many in vitro studies have shown that resin cements never completely polymerize and can cause reactions in the pulp and gingival cells.8,10-12
Moreover, despite the improved mechanical properties of RM- GICs, only a few studies have demonstrated their degree of biocompatibility and cytotoxic effects. Therefore, the aim of the present study was to evaluate the cytotoxicity of Zinc Phosphate cement (Harvard), conventional GIC (Fuji I), RM-GIC (Fuji PLUS), and two types of resin cements (BisCem and Duo-Link).
Materials and Methods
In this experimental study, two different categories of dental cements were evaluated: category 1: chemically set cements (Fuji I, Fuji PLUS, and Harvard) and category 2: Dual curing resin cements (BisCem, Duo-Link).
L929 fibroblasts culture protocol:
The murine fibroblast cell line L929 was obtained from the Pasteur Institute of Iran. Cells were initially passaged on culture flasks. (Passaging: induction of fibroblast proliferation and changing the culture medium). Once the adequate number of cells proliferated and adhered to the flask, trypsin / ethylenediamine tetraacetic acid (EDTA) solution (Gibco, Scotland) was applied for 2 minutes at 37°C to detach the cells. These cells were subsequently cultured in 96-well plates, 3 × 103 cells per 200 µl of Dulbecco`s Modified Eagle`s Medium (DMEM) ( Gibco, Scotland) supplemented with 10% fetal bovine serum, penicillin and streptomycin and were incubated in the dark for 24 hours at 37°C with 5% CO2 and 95% air.
Preparation of specimens:
Round-shaped samples (4 for each experimental cement, with 2 mm height and 4 mm diameter) were prepared and placed inside 24-well plates (Costar Corp, Cambridge, MA, USA). The samples were divided into two categories:
Category 1: Chemically set cements consisting of three groups:
Group 1: Fuji I (GC, Tokyo, Japan)
Group 2: Fuji PLUS (GC, Tokyo, Japan)
Group 3: Harvard Zinc oxide phosphate cement (Richter & Hoffmann, Berlin, Germany)
Category 2: Dual cure cements consisting of two groups:
Group 4: Duo-Link (Bisco, Schaumburg, IL, USA)
Group 5: BisCem (Bisco, Schaumburg, IL, USA)
Cultured cells in distilled water served as positive controls and culture medium solutions were used as negative controls. Specimens were prepared in glass tubes (hollow cylinders with an internal diameter of 4 mm and height of 5 mm).
Harvard (Zinc phosphate cement), Fuji I (GIC) and Fuji PLUS (RM-GIC) were mixed according to the manufacturers` instructions using the recommended powder / liquid ratio by weight and were poured into the glassy mold (Table 1). For BisCem and Duo-Link cements, after mixing and pouring the mixture into the mold, they were light cured with a curing device (Optilux500, Demetron/Kerr, Danbury, CT, USA) for 40 seconds through one side of the mold. The light intensity was monitored with a radiometer(Optilux500, Demetron / Kerr , Danbury, CT, USA , 530 mW/cm3).3 Immediately after setting, the samples were removed from the mold and were exposed to UV light for 15 minutes to prevent bacterial contamination and were placed inside 24-well plates (Costar Corp, Cambridge, MA, USA) containing 1.1ml of DMEM culture medium (Dulbecco`s Modified Eagle`s Medium, Sigma Chemical Co, St. Louis, MO, USA) without fetal bovine serum. The samples immersed in DMEM were incubated with the conditions previously described for 24 hours. The specimens were then discarded and the extracts were filtered by membranes with 0.22 µm pore size (Millipore, Billerica, MA, USA). The cultured medium of fibroblast cells was discarded and replaced by eluate extracts for 24, 48 and 72 hours. At that point, the extracts were presented to the fibroblast cells for 24 hours. Afterwards, the cells were subjected to the 3-(4, 5- dimethylthiazol-2-yl)-2, 5-diphenyl-2H-tetrazolium bromide (MTT) assay for cytotoxicity assessment.8
MTT assay:
The cell metabolic activity was evaluated by succinic dehydrogenase (SDH) activity which is a measure of the mitochondrial respiration of the cells. This test was performed through 3 independent experiments for each cell type, according to the guideline in ISO 10993-5:2009. Subsequently, 10 µl of the MTT solution (Sigma-Aldrich, St. Louis, MO, USA) was added to each well and incubated for 3 to 4 hours in standard conditions. Then the culture medium was removed and 100µl of dimethyl sulfoxide (DMSO), (Panreac Quimica) was added to each well. The plates were vibrated for 5 minutes before being placed in a microplate reader (Synergy HT, BioTek Instruments, Winooski, VT, USA). The absorbance was read at a wavelength of 570 nm .13
Data analysis:
Statistical analysis was performed using Graph Pad Prism5 (Graph Pad software, La Jolla, CA, USA). The results were subjected to one-way analysis of variance (ANOVA) followed by Tukey`s post-hoc test for comparison between pairs of groups. The significance level was set at p< 0.05.
Results
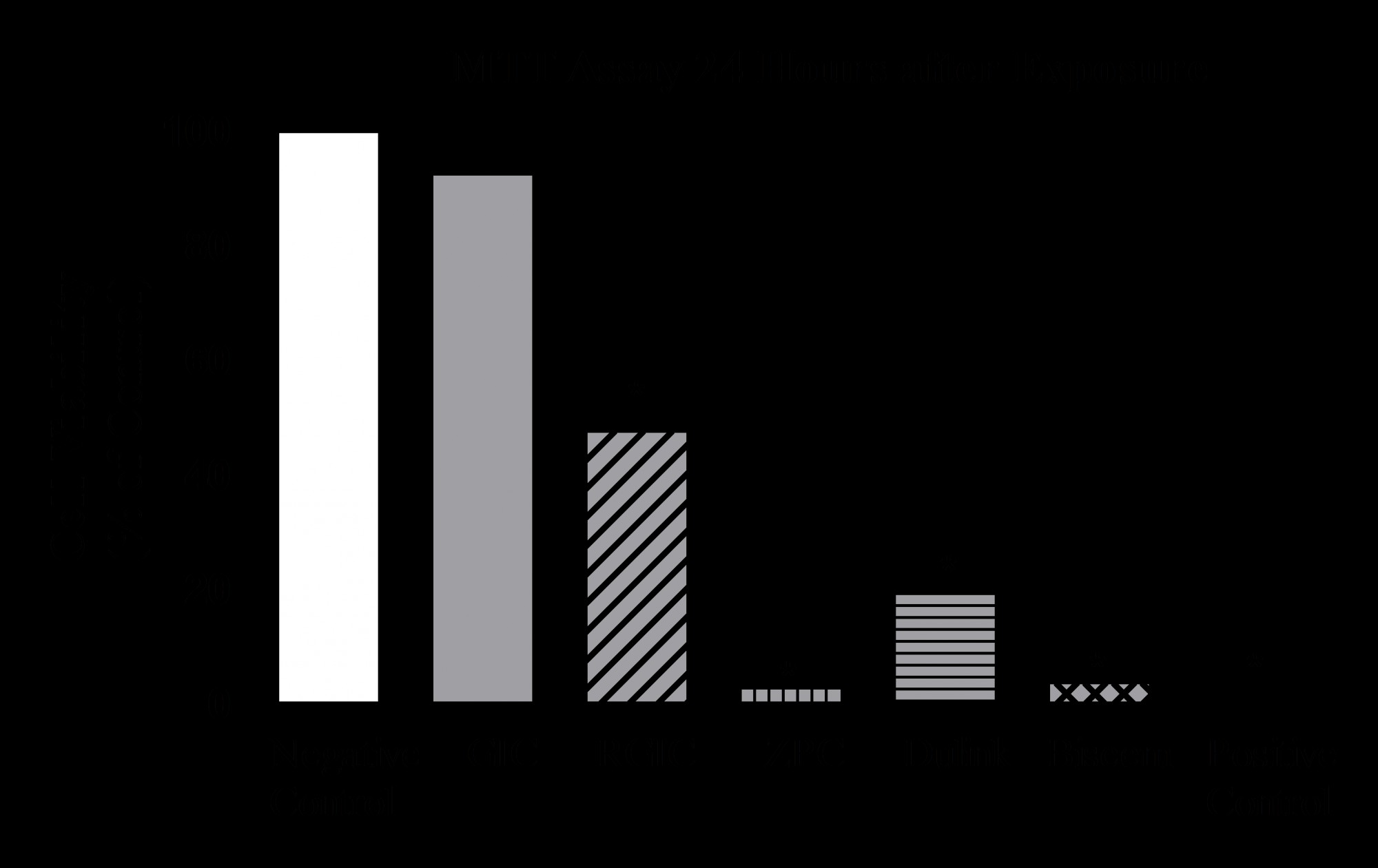
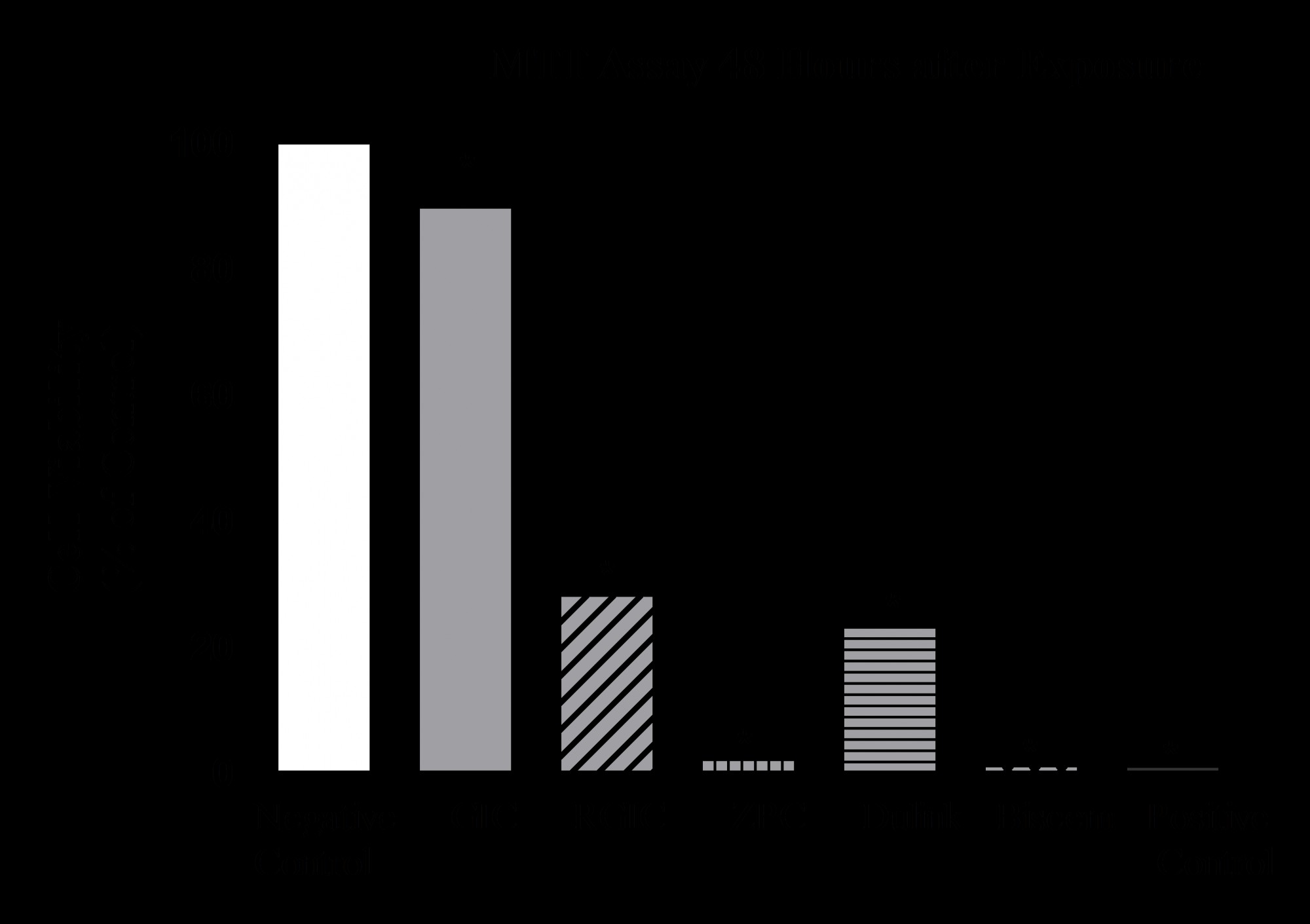
The mean cytotoxicity values of the five types of dental cement specimens represented by the standardized cell numbers and the corresponding 95% confidence intervals are presented in Figures 1 to 3.
Figure 1- MTT assay, 24 hours after exposure
Figure 2- MTT assay, 48 hours after exposure
Figure 3- MTT assay, 72 hours after exposure
In the category of chemically set cements, Fuji I (GIC) was generally less cytotoxic than Fuji PLUS (RM-GIC) (P=0.001) while Harvard (zinc phosphate cement) was more cytotoxic than the two mentioned cements. (P=0.001).
In the category of dual cure adhesive cements, BisCem and Duo-Link cements showed differences which were significant at 24 hours (P= 0.001). However, BisCem specimens showed significantly more cytotoxicity than Duo-Link at 48 and 72 hours (p<0.001). (Fig. 1) Overall, the extracts obtained after 24 hours of incubation were more cytotoxic than the extracts obtained after 48 and 72 hours. Harvard zinc phosphate and BisCem cements showed the highest cytotoxic effects which were not significant compared with the positive control group (distilled water). These cements decreased the cell viability by 99%, 99% and 99.9 % after 24, 48 and 72 hours, respectively. The cytotoxic effect of Fuji I cement was not significantly different from the negative control group at 24 hours evaluation (p>0.05). However, Fuji I presented higher cytotoxic effects on the cultured cells after 48 and 72 hours, decreasing the cell viability by 24% after 72 hours. (Fig. 4)
Figure 4- Multiple comparisons at 24, 48 and 72 hours
Table 1- Tested dental cements and their properties
Although Fuji I cement was less cytotoxic than the other specimens, all the cements significantly decreased the cell metabolism in comparison with the negative control group.
Discussion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This experimental study used a standardized protocol to identify and compare the cytotoxic potential of dental cements.
In vitro cytotoxic tests allow easy control of experimental factors that are often challenging when performing experiments in vivo. In vitro methods are reproducible, cost effective, applicable and suitable for the evaluation of basic biological properties of dental materials.14-16
Different in vitro testing methods and cell lines have been used to determine the cytotoxicity of dental materials. In this study, the effect of Harvard (zinc phosphate cement), Fuji I (GIC), Fuji PLUS (RM- GIC), Duo-Link and BisCem (adhesive resin cements) on L929 fibroblast cell line was investigated using the MTT assay.
Fibroblasts are the targets of chemical components released from dental restorative materials. L929 mouse fibroblasts were chosen in the present research because they are easy to prepare and culture. Other advantages include popularity, efficiency to grow in vitro and reproducibility of the results. These cells show comparable results to primary human gingival fibroblasts and therefore, might represent a model for gingival toxicity in vitro .17,18,19 The MTT assay is a well-established method for analyzing the cell viability.
MTT is reduced to purple formazan in the mitochondria of living cells. Solubilization of the purple formazan produces a colored solution. The absorbance of the colored solution can be quantified by a spectrophotometer.
Cytotoxicity responses were rated as sever (30%>), moderate (30-60%), mild (60-90%) and nontoxic (>90%).14
In the present study, Harvard zinc phosphate and BisCem cements showed the highest cytotoxicity with no significant difference from the positive control (P>0.05). Cell cytotoxicity was severe in zinc phosphate cement samples (less than 30% cell viability). Cell viability equaled 2.9%, 2.2% and 0.9 % at 24, 48 and 72 hours, respectively. Leirskar and Helgeland analyzed the culture media of zinc phosphate cement and showed a slow but similar decrease in the phosphate concentration. They stated that zinc was rapidly released into the medium from the disks of zinc phosphate cement during incubation which has been shown to be toxic to the studied cell line. Moreover, a small amount of fluoride was found in the medium. They reported that the pH of the culture media containing zinc phosphate decreased slowly during the incubation period from 7 to 6.6 after two days .4 Since some cell death was observed from the first day to the third day in the presence of zinc phosphate cement, additional factors besides acidification must have been involved. These observations are in agreement with the findings of Welker and Neupert (1974) and also Leirskar et al (1977).14,15 PH corrections of the media with zinc phosphate cement could not eliminate the toxicity of the cement on monolayer cultures of mouse fibroblasts and substantial amounts of zinc released during incubation have been shown to be toxic to the studied cell line. Considering the amount of zinc released from zinc phosphate cement, higher levels of cytotoxic effects were anticipated, which suggests that other elements such as acid released from this cement might modify the effect of zinc. It has been shown that the uptake of zinc in murine macrophages, platelets and lymphocytes is reduced when the pH is lowered (Karl, Chvapil and Zukoski 1973).20
In this study, Harvard zinc phosphate cement was shown to be more cytotoxic than Fuji PLUS (RM-GIC). Fuji PLUS showed moderate to severe cytotoxic effects (cell viability at 24, 48, and 72 hours was 47.7%, 37.7% and 11.7% respectively). Fuji I GIC had the least cytotoxic effect and was in the nontoxic to mildly toxic category (cell viability after 24, 48 and 72 hours was 92.6%, 89.9% and 67.2% respectively). Several in vitro studies have assessed the cytotoxicity of conventional and resin-modified glass ionomers on cultured cells. Most of these in vitro studies have supported the concept that leachable components of dental materials are responsible for the adverse effects on cell culture. On the other hand, Lewis et al reported that leachable components of GICs may affect the rate of progression of oral epithelial cells through the cell cycle rather than causing toxic effects on the cells resulting in cell death.20
Oliva et al showed that RM-GIC exhibited high cytotoxic effects. The adverse effect caused by RM-GIC was attributed to the leaching of poly acidic phase (HEMA).21 In many studies, HEMA has been shown to diffuse rapidly across dentin due to its low molecular weight and high solubility in water. Residual methacrylate monomers are incorporated into the lipid bilayer of the cell membrane leading to the solubilization of this structure. This phenomenon is responsible for cell death and indicates that HEMA plays an important role in the cytotoxicity of RM-GICs.22-24The liquid of Fuji PLUS cement is composed of 20-30 % of HEMA while the concentration of this component is only 8-10% in the liquid of Fuji I cement. It may be suggested that the concentration of HEMA could be one of the factors responsible for the higher cytotoxicity of Fuji PLUS compared to Fuji I .12,25,26
However, the concentrations of HEMA that can diffuse into the pulpal tissue are significantly lower than the concentrations which cause acute toxicity. Therefore, for RM-GIC, the leaching of the combination of toxic components including resin monomers and fluoride ions can be suspected. 21,22Recently, Kanjevac et al (2012) reported a correlation between cytotoxicity and fluoride release of modern glass ionomer cements. They also pointed out that the leaching of other components such as strontium (Sr 2+) and aluminum ions (AL 3+) presented more cytotoxic effects on cell cultures. They found that Fuji PLUS (RM-GIC) was more cytotoxic than Fuji I (GIC) due to higher fluoride release.27,28
Previous in vitro studies have demonstrated a reduced apparent cytotoxicity of diffusates when the materials are separated from cells by dentin barrier test device and have shown the low toxicity of zinc phosphate and RM-GIC .29As reported by Hanks et al (1994), dentin can absorb substances in the tubules and limit the diffusion of noxious substances into the pulp.30
In the present paper, dual cured specimens of resin-based cements (Duo-Link and BisCem) showed higher toxicity than the chemically set cements and were in the severely toxic category. Ulker and Sengun reported that BisCem was more cytotoxic than Rely- XTM Unicem.31
In the present study, BisCem was found to be more cytotoxic than Duo-Link at 48 and 72 hours. This concurs with the results of a study by Schmid – Schwap et al who stated that self-adhesive cements (Rely- XTM Plus) exhibited more cytotoxicity compared to adhesive resin cements.
However, Bis-GMA, UDMA, TEGDMA, Camphor Quinone and HEMA in resin composite cements may penetrate through dentin tubules, exert potential pulpal injury and inhibit pulp tissue repair.32-34According to Goldberg (2008), these monomers are cytotoxic in vitro for pulp and gingival cells. Leaching of some ions may cause cell alterations and some molecular mechanisms have been identified as key factors leading to apoptosis and / or pulp necrosis .35Bakopoulou et al (2009) investigated the genotoxicity and cytotoxicity of eluates derived from different types of dental cements on normal cultured human lymphocytes and reported that the released substances such as TEGDMA included in the resin cements' composition were responsible for the cytogenetic effects.36,37,38 A previous study demonstrated that the cytotoxicity ranking of the most widely used monomers was as follows: Bis-GMA> UDMA>TEGDMA> HEMA>MMA .39,40
UDMA and inorganic fluoride contents of Duo-Link cement may be responsible for the observed cytotoxic effects.
BisCem composite resin cement which contains TEGDMA and HEMA showed the most severe cytotoxic effects in the present study. In addition, BisCem reduced the pH to 3-4 which may be another reason for decreased cell viability compared to the effect of Duo-Link cement.
According to Gulferm et al (2011), reduced curing time significantly enhances the cytotoxicity of resin cements .Therefore, sufficient duration of curing should be considered.40
Conclusions
The experimental set up of this study showed that dental cements are capable of eliciting biological responses. Both gingival and pulpal cells might be affected by the released substances, since they are in close contact with the cement during cementation. The level of in vivo cytotoxicity depends on the amount of cement in contact with the oral tissue and the amount of the components released into the aqueous environment. According to this research, dental cements present a potential risk of tissue damage, although the risk depends on the cement's brands and curing modes.
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
